










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 no.1 Madrid ene./feb. 2016
https://dx.doi.org/10.20960/nh.13
TRABAJO ORIGINAL / Nutrición en el anciano
Compliance in food consumption of young and long-lived elderly of a city in southern Brazil
Adecuación en el consumo de alimentos en ancianos y ancianos longevos de una ciudad en el sur de Brasil
Fhaira Petter da Silva1, Loiva Beatriz Dallepiane2, Vanessa Ramos Kirsten2 and Rosane Maria Kirchner2
1Nutrition. Federal University of Santa Maria. Campus Palmeira das Missões. Postgraduate Program in Human Aging. University of Passo Fundo. Scholarship from CAPES/FAPERGS.
2Department of Foods and Nutrition. Federal University of Santa Maria. Palmeira das Missões, Brazil
ABSTRACT
Introduction: Life expectancy is increasing and becoming a characteristic phenomenon of developed countries and, increasingly, of developing countries, such as Brazil. The aging process causes changes of some physiological functions such as loss of smell, taste, loss of appetite, among other things that end up changing the food intake of these individuals.
Objectives: This study aimed to assess food consumption of the young and long-lived elderly in a city in southern Brazil.
Methods: A cross-sectional survey conducted through home visits in Palmeira das Missões - RS, Brazil. The sociodemographic, anthropometrical and dietary data were collected through questionnaires and 24-hour recall. The adequacy of nutrients was assessed according to the Dietary Reference Intakes. Data were analyzed using SPSS 18.0 software.
Results: The study included 424 older adults, 84,4% (n = 358) aged less than 80 years old and 15,6% (n = 66) older than 80. The intake of energy and protein was insufficient for both young elderly and the oldest. The consumption of vitamins and minerals has been insufficient in all seniors except for iron, which presented an excessive intake. There was a statistically significant difference between the elderly and oldest only for the consumption of lipids and vitamin B12.
Conclusion: The majority of studies with elderly corroborate the results found in this article. An inadequate intake of nutrients can develop nutritional deficiencies, and consequently it can result in physiological and pathological changes which would compromise the functional capacity of the elderly.
Energy consumption was insufficient and macronutrients were inadequate, both for the young elderly as for the oldest. Additionally, the consumption of vitamins and minerals was insufficient to everyone except the iron, which presented excessive intake for young and oldest elderly.
Key words: Elderly. Aging. Food consumption in the elderly. Nutrients.
RESUMEN
Introducción: la esperanza de vida está aumentando y convirtiéndose en un fenómeno característico de los países desarrollados y, cada vez más, de los países en desarrollo, como Brasil. El proceso de envejecimiento produce cambios en algunas funciones fisiológicas, como la pérdida del olfato o gusto o pérdida de apetito, entre otros, que terminan alterando la ingesta de alimentos de estos individuos.
Objetivos: este estudio tuvo como objetivo evaluar el consumo de alimentos de los ancianos y de los ancianos más longevos en una ciudad del sur de Brasil.
Métodos: un estudio transversal realizado mediante visitas a domicilio en Palmeira das Missões - RS, Brasil. Los datos sociodemográficos, antropométricos y dietéticos fueron recogidos a través de cuestionarios y recordatorio de 24 horas. La adecuación de nutrientes se evaluó de acuerdo con las ingestas de referencia en la dieta. Los datos fueron analizados utilizando el software SPSS 18.0.
Resultados: el estudio incluyó a 424 adultos mayores, el 84.4% (n = 358) de ellos menores de 80 años y el 15.6% (n = 66) con más de 80 años. La ingesta de energía y proteínas fue insuficiente tanto para jóvenes adultos como para los más ancianos. El consumo de vitaminas y minerales ha sido insuficiente en todos los adultos mayores a excepción del hierro, que presentaba una ingesta excesiva. Hubo una diferencia estadísticamente significativa entre las personas de edad y mayores sólo en cuanto al consumo de lípidos y vitamina B12.
Conclusión: la mayoría de los estudios con personas mayores corrobora los resultados obtenidos en este artículo. Una ingesta inadecuada de nutrientes puede dar lugar a deficiencias nutricionales y, por lo tanto, a cambios fisiológicos y patológicos que pondrían en peligro la capacidad funcional de los ancianos.
El consumo de energía y de macronutrientes resultó insuficiente tanto para los ancianos como para los ancianos más longevos. Además, el consumo de vitaminas y minerales fue insuficiente para todos, excepto el hierro, que presentaba una ingesta excesiva tanto en adultos jóvenes como de edad más avanzada.
Palabras clave: Ancianos. Envejecimiento. Consumo de alimentos en ancianos. Nutrientes.
Introduction
Aging is a dynamic and ongoing process in which there are morphological, functional and biochemical changes, which gradually transform the body. These changes require an attentive look from health professionals of the elderly since in this life cycle there is an increased susceptibility to the development of diseases (1). These changes, as well as the diversity among the elderly, can contribute to change their nutritional status (2).
It is known that in old age certain sensory changes occur. Reduced sensitivity to sweet tastes primary, bitter, sour and salty, with possible loss of visual acuity, hearing and smell, are one of the main factors in the reduction of food intake the elderly (3).
In old age inadequacies in food intake begin to emerge. Those related to some particular food groups are extremely important at this stage of life and, taking into account the high prevalence of chronic diseases, it is worth noting the importance of a healthy and varied diet, both regarding energy and the variety of food groups to avoid nutritional imbalances in order to have a longer life with better quality of life (4).
This study aimed to evaluate the food consumption of the young and long-lived elderly in a city in southern Brazil.
Methodology
Cross-sectional survey of individuals of both genders over 60 years old, considered as elderly in Brazil (5), living in a city in southern Brazil. The sample was calculated taking into account the inclusion of 424 elderly (≥ 60 years old), with an error margin of 5%. There were excluded from the sample immobility. The residences were randomly selected, with an interview in the home of the elderly.
The variables analyzed were: a) socio-demographic data: age, gender, education (years of schooling) and income of the elderly (according to minimum wages); b) anthropometric: for the assessment of nutritional status we used the BMI (Body Mass Index). BMI was estimated after measuring the weight (kg) and height (m). The calculation was made by dividing weight in kilograms by the square of height in meters and the result was expressed in kg/m2. For the BMI classification NSI (Nutrition Screening Initiative) parameters were used (6). Waist circumference was determined with a flexible and inextensible tape measure, measured at the midpoint between the lower border of the last rib and the iliac crest. The calf circumference was taken with the knee bent at 90-level turn, heel resting in bed or chair, measuring the largest circumference with tape measure (7); c) diet: The food intake assessment was made by applying a 24-hour dietary recall (24 h). The calculations of the 24-hour recalls were made using the online software Avanutri (8).
To evaluate the adequacy of energy consumption we used the recommendation of the Institute of Medicine (9.10) which calls for men a total energy value (TEV) of 3.067 kcal and 2,403 kcal for women, subtracting from this value 10 kcal/day for men and 7 kcal/day for women for each year over 19 years old. For assessing the suitability of macronutrients (proteins, carbohydrates and lipids) the Institute of Medicine's recommendations were also used (11). With respect to micronutrients, calculations were made based on the Reference Intakes Dietary (Dietary Reference Intakes - DRIs) Institute of Medicine/Food and Nutrition Board, considering the estimated average requirement (Estimate Average Requirement - EAR) as the cutoff point, except for calcium, which was rated having as the benchmark the Adequate Intake (AI) (9-12). The macro and micronutrients energy consumption was classified as inadequate, adequate and excessive, according to the categories used by Galeasi et al. (2008) (13).
The elderly were divided into two categories: young elderly (aged 60 to 79 years old) and long-lived elderly (80 and over) (14).
Data were analyzed using SPSS 18.0 software. The analytical methods used were descriptive statistics, Chi-square test, Student's t test and Fisher's exact test considered as significant at p < 0,05.
The study was approved by the Research Ethics Committee of the Federal University of Santa Maria, under the number of CAAE 0135.0.243.000-10.
Results
The study included 424 elderly, 68.4% (n = 290) were female and 81.4% (n = 345) had an income of less than two minimum wages. The average age was 70.83 ± 7.8 years old, 84.4% (n = 358) between 60 and 79 and 15.6% (n = 66) were more than 80 years old.
Most participants had schooling below 5 years of study and the nutritional status is in overweight. It is observed that among the oldest there is 16.7% of thinness, although there was no statistically significant difference when compared to the percentage of leanness of the young elderly (10.3%). Similarly, more than a half of them had waist circumference (WC) above the recommended, indicating cardiometabolic. Despite the risk of most elderly people are with the circumference of the calf (CP) within the recommended levels, it is observed that among long there is a growing trend CP for smaller values indicating loss of muscle mass. It must be noted that there is a relationship between being old or young long-lived as the variables of sociodemographic characteristics and anthropometric parameters (Table I).

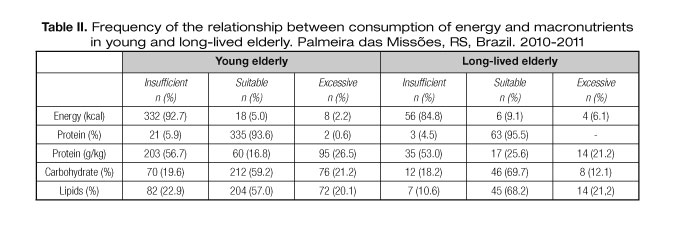
According to table II, the condition of insufficient intake was observed for energy and protein/kg/weight for both young elderly and for the oldest. Have the condition of fitness was observed in more frequently for protein, carbohydrate and lipids in young and long-lived elderly.
According to table III, the intake of vitamins A, D, E, B1, B2, B5, B6, B12, C, folate and the minerals calcium, phosphorus, magnesium, zinc, copper, iodine and selenium are insufficient both in young and long-lived elderly. Excessive intake of condition was checked only for the iron for young and long-lived elderly.

Table IV shows a statistically significant difference between the young and long-lived elderly only for the consumption of lipids, though both are below 30% of TEV.

In table V it is observed that there is a statistically significant difference between the young and long-lived elderly only regarding the consumption of vitamin B12. In the group of young elderly consumption of vitamin B12 average intake was below the recommended, while in long-lived elderly the average intake was greater than recommended, which is 2.4 μg.

Discussion
Inadequate food consumption observed in the present study was similar to the results found in a survey conducted in Europe, especially for vitamins A, D, B1, B2, B5, B6, B12, C, E and folate and the minerals calcium, phosphorus, magnesium, zinc, copper, iodine and selenium, presented insufficiently among adults and the elderly (15).
This inadequacy is worrying as vitamins and minerals are very important for maintaining various metabolic functions of the body, while macronutrients are important energy sources and help tissue regeneration (16).
Low energy intake among the young and long-lived elderly can be compared with the results of a study that investigated energy consumption in the elderly living in individual houses in Long Term Care Institutions, finding insufficient values in all groups categorized by the nutritional status (13). Similarly, a study of the power of the elderly in Fortaleza/CE (Brazil), found the average energy value was lower than the average value of the average estimated need in men and women (17).
In Brazil, studies carried out in the city of Joinville -SC and Fortaleza show that the amount of energy consumed by the elderly is low, both in institutionalized and non-institutionalized elderly (18,19). As a result of low energy intake by the elderly, there is also an insufficient intake of micronutrients, observed not only when the intake is below 1,500 kcal but above 1,500 kcal (20). Aging characteristic functional changes can be highlighted as contributing to inadequate dietary intake. In addition, poor nutrition has severe consequences for the immune response in the elderly and it becomes even more serious health the same when associated with typical immunosenescence frame. Thus, the vicious cycle between nutritional deficiencies and infections related to immunosenescence is a very vulnerable condition in the population above 60 years old (21).
In the present study a statistically significant difference between young and long-lived elderly regarding the consumption of vitamin B12 was found. B vitamins, including B12, operate in different systems and in different enzyme forms, participating as coenzymes in the activation of various metabolic processes, and they play a fundamental role in the metabolism of carbohydrates, lipids and proteins. Vitamin B12 is an essential micronutrient for various metabolic pathways in the central nervous system and also acts in the production of red series (22). Low intake leads to a deficiency which can not only be associated with macrocytic anemia but with other diseases such as dementia, sub-acute degeneration, peripheral neuropathy and with diseases of cardiac origin. Similar results of low intake of vitamin B12 were found in previous studies (23,24).
Corroborating the study, according to a survey by Lopes et al. 2005 (25) shown below, suitability for calcium, zinc, vitamins C, B6, E, A, and excessive intake of iron were found. However, there were results divergences in these studies as the consumption of proteins and carbohydrates was insufficient, while the match was overconsumption.
Insufficient intake of antioxidant vitamins and zinc can cause the appearance of cardiovascular diseases, cancers, and other disorders in the elderly population (26,27). Inadequate food intake leading to enough calcium and zinc contributes to the high incidence of bone abnormalities such as osteoporosis and fractures, especially in older women (28,29). Osteoporosis is a cause for pathological fractures and loss of autonomy and validism (30). Older adults have a lower calcium absorption rate due to the following factors: low dietary intake, reduction in endogenous production of vitamin D and gastric atrophy, responsible for the increase in gastric pH, reducing acidification, a vital phase for a better absorption of calcium diet (31).
In this study, both young and elderly to the long-lived nutrient iron showed a significant prevalence of excessive intake. However, it should be considered that despite the iron intake is high, this population may have iron deficiency to risks as iron absorption may be impaired, as well as the fact that this deficiency may not only be determined by the low iron intake, but by the possibility of noticeable bleeding due to disease processes (32). However they were not evaluated in this study.
The study had some limitations, especially the performance of the 24-hour food recall only and underreporting of food consumption by individuals over 60 years old, which may have influenced the results. However, compared with other studies, similar results were found, even in researches including more than one recall. In population surveys with questions about feeding, the underreporting of food that may be inconsistent or consistently should be taken into account (33). Underreporting involves moral, emotional, social, physical and cognitive factors, expressively compromising the inferences made from assessment studies of food intake (34). The conscious omission is due to the constraint in reporting certain foods considered as "unhealthy" or unsavory (35).
A balanced diet should include vitamins, minerals and antioxidants, which are critical to the performance of many chemicals present in the human body. The beneficial and desirable effects of these substances are proven in improving organ dysfunction, resulting from the aging process (36).
Inadequate nutrient intake leads to nutritional deficiencies that merit special attention, since they result in functional and pathological changes that compromise the functional capacity of the elderly. It is essential that there care practices to senescent, towards health promotion, always seeking healthy and proper habits. This practice is supported in the National Health Promotion Policy itself, which provides for the promotion of healthy eating as one of its specific actions (37).
Conclusion
The study population consisted of young and long-lived elderly, predominantly female, with low education and income, overweight, cardiovascular risk assessed by waist circumference, but not showing loss of muscle mass, assessed by the circumference of the calf of leg.
The energy consumption was insufficient and the macronutrients were adequate for both the young elderly and the oldest. The consumption of vitamins and minerals was insufficient in all participants, except for iron, that showed an excessive intake for the young and long-lived elderly. There was no statistically significant difference regarding nutrients intake between groups of young people and the oldest.
References
1. Chagas AM, Rocha ED. Aspectos fisiológicos do envelhecimento e contribuição da Odontologia na saúde do idoso. Rev Bras Odontol 2012;69(1):94-6. [ Links ]
2. De Sousa VMC, Guariento ME. Avaliação do idoso desnutrido. Rev Bras Clin Med 2009;7:46-9. [ Links ]
3. Monteiro MAM. Percepção sensorial dos alimentos em idosos. Rev Espaço para a Saúde 2009;10(2):34-42. [ Links ]
4. Papini SJ, Corrente JE, Corren JE. Avaliação da alimentação de idosos de município paulista - Aplicação do Índice de Alimentação Saudável Assessment of the diets of elderly people in a city in São Paulo state - Application of the Healthy Eating Index. Cien Saude Colet 2013;18(2):377-84. [ Links ]
5. World Health Organization. Envelhecimento ativo: uma política de saúde. Organ Pan-Americana da Saúde; 2005. [ Links ]
6. The Nutrition Screening Initiative. Incorporating nutrition screening and interventions into medical practice. A monograph for physicians. Washington, DC: American Academy of Family Physicians. The American Dietetic Association. National Council on Aging Inc; 1994. [ Links ]
7. Orientações para a coleta e análise de dados antropométricos em serviços de saúde: Norma Técnica do Sistema de Vigilância Alimentar e Nutricional - SISVAN. Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica. 1st ed. Brasília: Ministério da Saúde; 2011. [ Links ]
8. Avanutri: Programa de Avaliação Nutricional. Cited Oct 3rd 2012. Available in: http://www.avanutrionline.com/. [ Links ]
9. Institute of Medicine. Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. Journal of the American Dietetic Association. Washington, DC: National Academy Press; 2002 Nov. p. 697-736. [ Links ]
10. Institute of Medicine. Food and Nutrition Board. Dietary reference intakes: for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids. Washington: National Academy Press; 2002/2005. [ Links ]
11. Institute of Medicine. Dietary reference intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. Washington: National Academy Press; 2002. [ Links ]
12. Institute of Medicine. Dietary reference intakes for vitamin C, vitamin E, selenium, and carotenoids. Washington: National Academy Press; 2000. [ Links ]
13. Galesi LF, Rita M, Oliveira M de, Cristina K, Fogaça P. Perfil alimentar e nutricional de idosos residentes em moradias individuais numa instituição de longa permanência no leste do estado de São Paulo. Alim Nutr 2008;19(3):283-90. [ Links ]
14. Instituto de Pesquisa Econômica Aplicada. IPEA. Cited Mar 21st 2012. Available in: http://www.ipea.gov.br/portal/. [ Links ]
15. Viñas BR, Barba LR, Ngo J, Gurinovic M, Novakovic R, Cavelaars A, et al. Projected prevalence of inadequate nutrient intakes in Europe. Ann Nutr Metab 2011;59(2-4):84-95. Cited Jun 1st 2014. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22142665. [ Links ]
16. Velásquez-Meléndez G, Martins IS, Cervato AM, Fornés NSM, Nunes M de F. Consumo alimentar de vitaminas e minerais em adultos residentes em área metropolitana de São Paulo, Brasil. Rev Saúde Pública 1997;31(2):157-62. [ Links ]
17. Menezes TN de, Souza JMP de, Marucci M de FN. Necessidade energética estimada, valor energético e adequação de macronutrientes da alimentação dos idosos de Fortaleza - CE Estimated energy requirement, energy value and adequacy of food macronutrients in the diet of elderly in Fortaleza - Ceará 1. Nutr Rev Soc Bras Alim Nutr = J Brazilian Soc Food Nutr 2004;34(3):17-30. [ Links ]
18. Mastroeni MF. Estado nutricional e consumo de macronutrientes de idosos da cidade de Joinville, SC. s.n; 2004. Cited Jun 17th 2014. Available in: http://bases.bireme.br/cgi-bin/wxislind.exe/iah/online/?IsisScript=iah/iah.xis & src=google & base=LILACS & lang=p & nextAction=lnk & exprSearch=359312 & indexSearch=ID. [ Links ]
19. Menezes TN de, Marucci M de FN. Oferta e consumo alimentar de idosos residentes em instituições geriátricas: diferença no valor energético total. Fortaleza/Ceará. Nutr Rev Soc Bras Aliment Nutr 2006;31(2):1-11. Cited Jun 17th 2014. Available in: http://bases.bireme.br/cgi-bin/wxislind.exe/iah/online/?IsisScript=iah/iah.xis & src=google & base=LILACS & lang=p & nextAction=lnk & exprSearch=455662 & indexSearch=ID. [ Links ]
20. De Groot CP, Perdigao AL, Deurenberg P. Longitudinal changes in anthropometric characteristics of elderly Europeans. SENECA Investigators. Eur J Clin Nutr 1996;50 (2):S9-15. Cited Jun 15tth 2014. Available in: http://www.ncbi.nlm.nih.gov/pubmed/8841780. [ Links ]
21. Meydani A, Ahmed T, Meydani SN. Aging, nutritional status, and infection in the developing world. Nutr Rev 2005;63(7):233-46. Cited Jun 15th 2014. Available in: http://www.ncbi.nlm.nih.gov/pubmed/16121477. [ Links ]
22. Hugo Sánchez R, Masferrer D, Lera L, Arancibia E, Ángel B, Albala C. Déficit de vitamina B12 asociado con altas dosis de metformina en adultos mayores diabéticos. Nutr Hosp 2014;29(6):1394-400. [ Links ]
23. Soncini F, Costa MJ, Oliveira Tania MT de. Perfil audiológico de indivíduos na faixa etária entre 50 e 60 anos. Fono atual 2004;7(28):21-9. Cited Jun 15th 2014. Available in: http://bases.bireme.br/cgi-bin/wxislind.exe/iah/online/?IsisScript=iah/iah.xis&src=google&base=LILACS&lang=p&nextAction=lnk&exprSearch=417493&indexSearch=ID. [ Links ]
24. Martins V de O, Andrade CRF de. Study of pauses in elderly. Rev da Soc Bras Fonoaudiol. Sociedade Brasileira de Fonoaudiologia 2011;16(3):344-9. Cited Jun 15th 2014. Available in: http://www.scielo.br/scielo.php?script=sci_arttext & pid=S1516-80342011000300017 & lng=en & nrm=iso & tlng=pt. [ Links ]
25. Lopes ACS, Caiaffa WT, Sichieri R, Mingoti SA, Lima-Costa MF. Consumo de nutrientes em adultos e idosos em estudo de base populacional. Projeto Bambuí Nutrient consumption by adults and seniors in a population-based study: The Bambuí Project. Cad Saúde Pública 2005;21(4):1201-9. [ Links ]
26. Castro LCV, Franceschini S do CC, Priore SE, Pelúzio M do CG. Nutrição e doenças cardiovasculares: os marcadores de risco em adultos. Rev Nutr 2004;17(3):369-77. [ Links ]
27. Yakoob J, Jafri W, Abid S. Helicobacter pylori infection and micronutrient deficiencies. World J Gastroenterol 2003;9(10):2137-9. Cited Jun 16th 2014. Available in: http://www.ncbi.nlm.nih.gov/pubmed/14562364. [ Links ]
28. Michaëlsson K, Melhus H, Bellocco R, Wolk A. Dietary calcium and vitamin D intake in relation to osteoporotic fracture risk. Bone 2003;32(6):694-703. Cited Jun 16th 2014. Available in: http://www.ncbi.nlm.nih.gov/pubmed/12810177. [ Links ]
29. Montilla R das NG, Aldrighi JM, Marucci M de FN. Relação cálcio/proteína da dieta de mulheres no clima tério. Rev Assoc Med Bras 2004;50(1):52-4. [ Links ]
30. Ortiz SLB. Densidad mineral ósea, calcio dietético y factores presuntivos de riesgo de osteoporosis en mujeres ecuatorianas de la tercera edad. Nutr Hosp 2014;30(2):372-84. [ Links ]
31. Buzinaro EF, Almeida RNA De, Mazeto GMFS. Biodisponibilidade do Cálcio Dietético. Arq Bras Endocrinol Metab 2006;50(5):852-61. [ Links ]
32. Curiati J, Alencar Y. Nutrição e envelhecimento. Ateneu. São Paulo; 2004. [ Links ]
33. Tomoyasu NJ, Toth MJ, Poehlman ET. Misreporting of total energy intake in older men and women. J Am Geriatr Soc 1999;47(6):710-5. Cited Jun 16th 2014. Available in: http://www.ncbi.nlm.nih.gov/pubmed/10366171. [ Links ]
34. Scagliusi FB, Júnior AHL. Subnotificação da ingestão energética na avaliação do consumo alimentar Underreporting of energy intake in dietary assessment methods. Rev Nutr 2003;16(4):471-81. [ Links ]
35. Kretsch MJ, Fong AKH, Green MW. Behavioral and body size correlates of energy intake underreporting by obese and normal-weight women. J Am Diet Assoc 1999;99(3):300-6. [ Links ]
36. Carvalho JAM de, Garcia RA. O envelhecimento da população brasileira: um enfoque demográfico. Cad Saúde Pública 2003;19(2):725-33. Cited Jun 17th 2014. Available in: http://www.scielosp.org/pdf/csp/v19n3/15876.pdf. [ Links ]
37. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Política Nacional de Promoção da Saúde. 3rd ed. Brasília: Ministério da Saúde; 2010. [ Links ]
![]() Correspondence:
Correspondence:
Loiva Beatriz Dallepiane.
Department of Foods and Nutrition.
Federal University of Santa Maria.
Campus Palmeira das Missões.
Av. Independência, 3751.
Bairro Vista Alegre 98.300-000.
Palmeira das Missões, Brazil
e-mail: loiva.dallepiane@hotmail.com
Received: 02/04/2015
Accepted: 18/05/2015
