










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.34 no.1 Madrid ene./feb. 2017
https://dx.doi.org/10.20960/nh.971
TRABAJO ORIGINAL / Paciente crítico
Underfeeding versus full enteral feeding in critically ill patients with acute respiratory failure: a systematic review with meta-analysis of randomized controlled trials
Subalimentación versus alimentación enteral completa en pacientes críticamente enfermos con insuficiencia respiratoria aguda: una revisión sistemática con metaanálisis de ensayos controlados aleatorios
Oellen Stuani Franzosi1, Anize Delfino von Frankenberg2, Sergio Henrique Loss1-3, Diego Silva Leite Nunes1-3 and Silvia Regina Rios Vieira1,3,4
1Postgraduate Program in Medical Sciences. School of Medicine. Federal University of Rio Grande do Sul. Porto Alegre, Brazil.
2Postgraduate Program in Health Science: Endocrinology. Medical School. Federal University of Rio Grande do Sul. Porto Alegre, Brazil.
3Intensive Care Unit. Hospital de Clínicas de Porto Alegre. Porto Alegre, Brazil.
4Department of Internal Medicine. Medical School. Federal University of Rio Grande do Sul. Porto Alegre, Brazil
Systematic review registration number: International prospective register of systematic reviews: identifier: CRD42014013041.
Authors' contributions to manuscript: 1) designed research (O.S.F, A.D.v.F, S.H.L); 2) conducted research (O.S.F, A.D.v.F, S.H.L); 3) analyzed data or performed statistical analysis (O.S.F, A.D.v.F, S.H.L); 4) wrote paper (O.S.F, A.D.v.F, S.H.L, D.S.L.N, S.R.R.V); 5) had primary responsibility for final content (all authors). All authors read and approved the final manuscript.
ABSTRACT
Introduction: Although guidelines emphasize that the provision of enteral nutrition (EN) should be as close as the patient's needs, prospective studies question this strategy.
Objective: To compare the effect of two EN strategies (underfeeding versus full-feeding) on ICU and overall mortality (hospital mortality or 60-day mortality) and length of stay (LOS), duration of mechanical ventilation (MV), infectious complications, and gastrointestinal tolerance in ICU patients.
Methods: Random effects meta-analysis of randomized controlled trials (RCT). Our search covered MEDLINE, EMBASE, SCOPUS and CENTRAL databases until May 2015. Underfeeding was assigned into two different groups according to the level of energy intake achieved (moderate feeding 46-72% and trophic feeding 16-25%) for subgroup analysis.
Results: Five RCTs were included among the 904 studies retrieved (n = 2,432 patients). No difference was found in overall mortality when all five studies were combined. In the subgroup analysis, moderate feeding (three studies) showed lower mortality compared with full-feeding (RR 0.82; 95% CI, 0.68-0.98; I2 0% p = 0.59 for heterogeneity). No differences were found for ICU mortality, ICU and hospital LOS, duration of MV, and infectious complications. Underfeeding showed lower occurrence of GI signs and symptoms except for aspiration and abdominal distention (no difference was found).
Conclusions: This meta-analysis found no differences in ICU and overall mortality, ICU and hospital LOS, duration of MV, and infectious complications between underfeeding and full-feeding. The subgroup analysis showed lower overall mortality among patients receiving moderate underfeeding. This result should be cautiously interpreted due to the limitations of the small number of studies analyzed and their methodology.
Key words: Enteral nutrition. Critical care. Mortality. Artificial respiration. Digestive signs and symptoms.
RESUMEN
Introducción: a pesar de las directrices que hacen hincapié en que la cantidad de la Nutrición Enteral (NE) administrada debe estar próxima a las necesidades del paciente, los estudios prospectivos cuestionan esta estrategia.
Objetivo: comparar el efecto de dos estrategias de NE (subalimentación vs. alimentación completa) sobre la mortalidad en la UCI y general (mortalidad hospitalaria o la mortalidad en 60 días), el tiempo de internación en la UCI y en el hospital, duración de la ventilación mecánica (VM), complicaciones infecciosas y la tolerancia gastrointestinal en pacientes críticos.
Métodos: metaanálisis de efectos aleatorios de ensayos clínicos aleatorizados (ECA). Nuestra búsqueda se basa en MEDLINE, EMBASE, SCOPUS y CENTRAL hasta mayo de 2015. La subalimentación fue asignada a dos grupos diferentes de acuerdo con el nivel de consumo de energía (alimentación moderada 46-72% y la alimentación trófica 16-25%) para el análisis de subgrupos.
Resultados: se incluyeron cinco ECA entre los 904 estudios que se encontraron en la búsqueda (n = 2.432 pacientes). No se encontraron diferencias en la mortalidad general cuando se combinaron los cinco estudios. En el análisis de subgrupos, la alimentación moderada (tres estudios) mostró una mortalidad más baja en comparación con la alimentación completa (RR 0,82; IC 95% 0,68-0,98; I2 0% p = 0,59 para la heterogeneidad). No se encontraron diferencias de mortalidad en la UCI ni en el tiempo de internación hospitalaria, la duración de la VM y las complicaciones infecciosas. La subalimentación mostró menor aparición de signos y síntomas gastrointestinales, excepto para aspiración y distensión abdominal (no se encontró ninguna diferencia).
Conclusiones: este metaanálisis no encontró diferencias significativas de mortalidad, duración de la estancia, duración de VM ni complicaciones infecciosas en la UCI o hospitalización total entre los grupos de subalimentación y alimentación completa. El análisis de subgrupos mostró menor mortalidad global entre los pacientes que recibieron la subalimentación moderada. Este resultado debe interpretarse con cautela debido a las limitaciones del pequeño número de estudios analizados y su metodología.
Palabras clave: Nutrición enteral. Cuidados críticos. Mortalidad. Respiración artificial. Signos y síntomas digestivos.
Introduction
Critically ill patients are characterized by high metabolism due to stress response. Cytokine and stress hormones predispose patients to high protein catabolism due to muscular proteolysis, allowing the synthesis of acute-phase protein (1). As a result of this stress response, critically ill patients are bound to develop protein and energy deficits, added by total or partial inability of oral feeding. In order to prevent nutrition deficits related with the morbidity and mortality of hospitalized patients (2) and their associated worse clinical outcomes, enteral nutrition (EN) is the recommended first-line therapy for critically ill patients (3).
Full-feeding (targeting the estimated energy requirement) is recommended by the main guidelines to prevent nutritional deficits, mitigate lean mass loss, prevent complications, and improve clinical outcomes (4-6). Observational data suggest that energy deficits (energy received-energy requirements) are associated with worse patient outcomes (7). However, prospective studies found no association with improvement in clinical outcomes with full-feeding (8,9).
Intentional calorie restriction (permissive underfeeding) has been associated with improvements in longevity biomarkers in overweight individuals (10). However, during a period of critical illness, the relevance of the potential mechanisms by which calorie restriction would be beneficial still unclear. In critical care, moderate feeding (lower-than-target) is supported by observational and prospective studies and thought to be as beneficial or at least as effective as full-feeding (11,12). Trophic feeding (EN infusion rate of 10-30 ml/h) has been proposed as a strategy to maintain gut integrity and function due to the reduced feeding complications and gastrointestinal intolerances.
There is still no consensus regarding the optimal amount of calories that critically ill patients should receive. Additionally, comparisons among studies are challenging because depending on how caloric goals are estimated, full-feeding in one study turns out to mean the same number of calories as underfeeding in another. However, taking into account that this topic has being highly debated and there is literature showing results in opposite directions, it is important to summarize data to better understand which approach may improve outcomes in this population. Therefore, the aim of this study is to systematically review and analyze randomized controlled trials (RCTs) comparing the effects of underfeeding with full-feeding strategy in patients with acute respiratory failure requiring mechanical ventilation (MV) on ICU and overall mortality, ICU and hospital length of stay (LOS), duration of MV, infectious complications, and gastrointestinal tolerability.
Materials and methods
PROTOCOL AND REGISTRATION
A predetermined protocol established according to Cochrane Handbook recommendations (13) was registered at the international prospective register of systematic reviews under the number CRD42014013041. The PRISMA statement is used to improve the reporting of results (14).
INCLUSION AND EXCLUSION CRITERIA
We considered all RCTs comparing underfeeding and full-feeding strategies in adult patients with acute respiratory failure requiring MV. Data from at least one major clinical outcome (ICU and overall mortality, ICU and hospital LOS and duration of MV) had to be available for study inclusion. In addition to major clinical outcomes, infectious complications and gastrointestinal signs and symptoms (regurgitation, aspiration, vomiting, diarrhea, constipation, abdominal distention, elevated gastric residual volume (GRV) and use of prokinetic agents) were analyzed. If data necessary for the review were missing, we contacted the authors by e-mail. The study was excluded if no answer was received within four weeks. We also excluded studies that did not report outcomes and/or used supplementary parenteral nutrition. No language, date or publication status restrictions were imposed.
SEARCH STRATEGY AND INFORMATION SOURCES
We searched MEDLINE, EMBASE, SCOPUS and the Cochrane Central Register of Controlled Trials (CENTRAL) (up to May 2015). We used the acronym PICO (Participant, Interventions, Comparisons, and Outcomes) to formulate the clinical question (13). Thus, the Medical Subject Headings (MeSH) terms and their entry terms were for population critical care; and for intervention and comparisons, enteral nutrition ("underfeeding" [intervention] and "full-feeding" [control]). For outcome, we decided not to restrict the search in order to find all available outcomes analyzed in the studies. We also included entry terms for RCT identification (available at http://www.sign.ac.uk/methodology/filters.html#random). The complete strategy for MEDLINE search is available at Supplemental Content. The studies were identified by database searching, scanning reference lists of articles and consultation with experts in the field. We checked the Annual Congresses of the following societies: American Society for Parenteral and Enteral Nutrition, European Society for Clinical Nutrition and Metabolism, Society of Critical Care Medicine and European Society of Intensive Care Medicine. A hand search was conducted for original papers published in relevant journals in the nutrition field.
DATA COLLECTION PROCESS
Titles, abstracts and full texts were reviewed by two independent reviewers (O.S.F and A.D.v.F). Disagreements regarding study inclusion were settled by a third investigator (S.H.L). Data were extracted independently by two reviewers using a piloted form.
The data extracted included the studies' methods and quality information (authors, publication year and journal, number of participants, study design, trial duration, randomization mode, allocation concealment, blinding, loss of follow-up and selective reporting), patients' demographic and baseline clinical characteristics (age, gender, BMI, admission category, prevalence of sepsis, use of vasopressor agents, APACHE II or APACHE III score or SAPS II and PaO2/FiO2 ratio). Nutrition strategy characteristics included intervention period, energy intake target, achieved energy intake, initial dose, increasing feeding rate and GRV. Data regarding outcomes included: ICU and overall mortality (hospital mortality or 60-day mortality), ICU and hospital LOS, duration of MV, infectious complications and gastrointestinal intolerance (diarrhea, constipation, abdominal distention, vomiting, aspiration, regurgitation, elevated GRV and use of prokinetic agents).
ASSESSMENT OF METHODOLOGICAL QUALITY
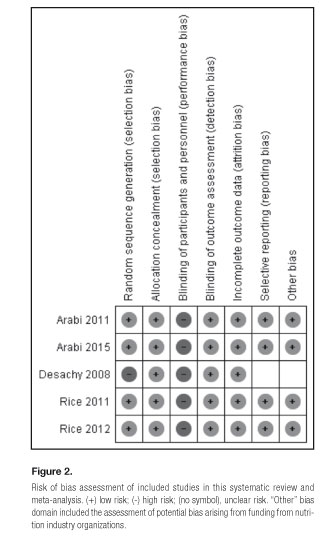
The methodological quality and risk of bias of the studies included were independently assessed by two reviewers (O.S.F and A.D.v.F). Biases were classified into six domains: Selection bias, Performance bias, Detection bias, Attrition bias, Reporting bias and other. The "other" domain included the assessment of potential bias arising from funding from nutrition industry organizations. Each domain was classified as high, low or unclear (13). Regarding risk of bias from funding, it was classified as "low" if the author described the funding/support sources or "unclear" if the information was not reported.
STATISTICAL ANALYSIS
ICU and overall mortality and infectious complications were analyzed through Mantel-Haenszel method (15,16) and summarized as risk ratios (RR). ICU and hospital LOS and duration of MV through inverse variance method (13) and the effect measure as mean difference (MD). Diarrhea, constipation, distention, vomiting, aspiration, regurgitation, GRV and use of prokinetic agents were analyzed through inverse variance method (13) and summarized as RR after logarithmic transformation. For both RR and MD, their corresponding 95% confidence intervals (CIs) were estimated. Heterogeneity between studies was assessed using Cochran's x test (Q test) (statistically significant at p for trend ≤ 0.10). The I2 test was also performed to evaluate the magnitude of heterogeneity and was considered high if I2 ≥ 50.0%. Considering the conservative characteristic of the random-effects model (17), this approach was used to summarize RR and MD estimates. To detect publication bias, we performed Begg's and Egger's tests (18,19). We conducted a subgroup analysis wherein the underfeeding group was assigned according to achieved energy intake (trophic nutrition [16-25% of target] and moderate feeding ([46-72% of target]). Meta-analyses were performed using RevMan v 5.3 analysis software from the Cochrane Collaboration (20).
Results
LITERATURE SEARCH AND STUDY SELECTION
The flow diagram for the selection of eligible studies is presented in figure. 1. Through database searching, we identified 901 studies, and through other sources three more studies were added. For full text examination we selected 25 studies (see data collection process) and after exclusions, five studies were included in the final qualitative and quantitative analysis (21-25). The characteristics of the studies included are presented in table I, while those related to nutritional strategy are shown in table II.



Studies included 100 to 1,000 patients of both genders and with mean age of 54 ± 4.3 years. Mean BMI was not different between underfeeding and full-feeding groups for all studies, ranging from 25.0 to 30.4 kg/m². Four studies reported the admission category, with samples mainly composed of medical patients (average of 72%) (21,22,24,25). Although studies have used different scores to assess severity, there were no differences between underfeeding and full-feeding groups for all studies. Among five trials included in this meta-analysis, three (21,23,24) used as inclusion criteria the expectation to require MV for ≥ 72 hours, so all patients were on MV. Despite MV having not been considered as an inclusion criteria in two studies, 99% and 97% of patients were on MV respectively (22,25).
Four studies presented data on baseline sepsis diagnosis, use of vasopressor agents and PaO2: FiO2 ratio (22-25). Despite no difference within studies, baseline sepsis diagnosis and use of vasopressor agents were higher in two studies (22,25) and baseline PaO2:FiO2 ratio was lower in another study (24).
As far as nutritional strategies are concerned, the intervention period was similar in four studies (4.7 days (21) to 7 days (22)). In one study the intervention period was longer (9.4 days) (25). The calculated caloric requirement of full-feeding groups ranged from 1,608 to 1,842 kcal/d and that of underfeeding groups from 1,570 to 1,833 kcal/d (Table II). The energy intake achieved in full-feeding groups ranged from 71 to 93% of the estimated energy goal between the five studies; on the other hand, it varied widely in the underfeeding groups, reaching 16-25% in two studies (trophic nutrition) (23,24) and 46-72% in the other three (moderate feeding) (21,22,25). The initial dose in full-feeding groups was similar in three studies (22-24) while, in a single study, EN was started at optimal flow rate (21). In the five studies, the initial dose in underfeeding groups ranged from 10 to 30 mL/h. The increasing feeding rate in full-feeding groups was also similar in four studies (22-25), ranging from 10 to 30 mL/h, guided by protocols that considered GRV as a sign of EN tolerance. In the underfeeding groups, two studies did not increase the feeding rate during the intervention period, keeping the initial dose (23,24), one study increased the feeding rate of 25 mL/h every 24 h (21), and two studies increased the feeding rate of 10 mL every 4 or 12 h according to EN tolerance until reaching the energy goal (22,25). GRV used in the feeding protocols ranged from 150 to 400 mL in the five studies. One multicentric study reported the feeding protocol used in one center while the other centers were free to use their own standard feeding protocols (25).
RISK OF BIAS IN THE INCLUDED STUDIES
Risk of bias assessment of the studies included in this systematic review and meta-analysis is summarized in figure 2. The risk of bias for random sequence generation was low in four studies (22-25). In one study (21) it was high due to more patients having been admitted after surgery in the underfeeding group and more patients having been admitted for trauma in the full-feeding group. Risk of bias from allocation concealment was low in all studies. Risk of bias from performance was high for all studies considering that in none of them the researchers were blinded due to the need of adjustments of the feeding rates according to the protocols. Risk of bias from detection was low in all studies, taking into account that outcome measurements were not likely to be influenced by lack of blinding. Attrition bias was low in all studies in view of the fact that outcome data were complete and the rate of discontinued intervention was low. Risk of bias from reporting was low in four studies (22-25) but in one study (21) the risk was unclear due to the absence of separate reporting of some gastrointestinal outcomes according to the groups. Regarding funding bias, it was low in four studies (22-25) that showed information about funding/support sources, none having received funding from nutrition industry organization. In one study it was unclear due to the absence of data (21).
Concerning publication bias, neither Begg's (p = 0.46) nor Egger's (p = 0.43) tests achieved significance, providing evidence of absence of publication bias.
EFFECTS ON CLINICAL OUTCOMES
Figure 3 presents a meta-analysis of overall and ICU mortality between underfeeding and full-feeding. All included studies evaluated the effects of underfeeding versus full-feeding on overall mortality. Pooled data from these five studies did not find differences between underfeeding and full-feeding strategies in the risk of overall mortality (RR, 0.91; 95% CI, 0.78-1.06; I2 13%, p = 0.33 for heterogeneity). The achieved energy intake varied widely in the underfeeding group even with low heterogeneity (I2 13% p = 0.33). Therefore, a secondary analysis was performed wherein underfeeding was divided into trophic feeding (16-25% of target) and moderate underfeeding (46-72% of target) according to the level of energy intake achieved (test for subgroup differences: I2 70.7%, p = 0.06). Mortality was lower with underfeeding in the three studieswhere the underfed group received moderate feeding (at a level that overlapped with the full-feeding level in some studies) (RR, 0.82; 95% CI, 0.68-0.98; I2 0%, p = 0.59 for heterogeneity).

Among the five selected studies, two were excluded from the ICU mortality analysis due to the absence of data (23,24). There was no difference in ICU mortality between the two strategies (RR, 0.86; 95% CI, 0.67-1.09; I2 0%, p = 0.66 for heterogeneity).
Forest plots of the effects of underfeeding versus full-feeding on ICU and hospital LOS and duration of MV are shown in figure 4. Three studies (21,22,25) reported the effects of nutritional strategies on ICU and hospital LOS. Regarding ICU LOS, two studies (21,25) reported the same period of hospitalization for both groups while the other (22) showed longer LOS in the full-feeding group. In the meta-analysis, no significant differences were found (MD, -0.61; 95% CI, -2.25-1.03; I2 26%, p = 0.26 for heterogeneity). As far as hospital LOS is concerned, no differences were found (MD, -1.94; 95% CI, -6.13-2.25; I2 0%, p = 0.91 for heterogeneity).

The duration of MV was evaluated by four studies (22,25) and did not significantly differ between groups (MD, -0.67; 95% CI, -1.52-0.19; I2 13%, p = 0.33 for heterogeneity).
Infectious complications were reported in four studies (22-25) and did not significantly differ between groups (RR, 1.00; 95% CI, 0.88-1.12; I2 0%, p = 0.54 for heterogeneity) (Fig. 5).

Effects of underfeeding versus full-feeding on gastrointestinal signs and symptoms are shown in figure 6. Among the five selected studies, three (21,23,24) reported data for vomiting, regurgitation and high GRV. Vomiting was 21% lower (RR, 0.79; 95% CI, 0.63-1.00; I2 0%, p = 0.87 for heterogeneity) and regurgitation 44% lower in the underfeeding group (RR, 0.56; 95% CI, 0.39-0.80; I2 0%, p = 0.73 for heterogeneity) as well as elevated GRV occurrence (RR, 0.39; 95%, CI, 0.25-0.61; I2 0%, p = 0.72 for heterogeneity). The use of prokinetic agents was reported by four studies and was less common in the underfeeding group (RR, 0.85; 95% CI, 0.73-1.00; I2 0%, p = 0.41 for heterogeneity) (21,23-25). Two studies (23,24) analyzed the effects of underfeeding versus full-feeding on constipation, aspiration and distention. Constipation was 33% less frequent in the underfeeding group when considering the feeding days (RR, 0.67; 95% CI, 0.54-0.85; I2 0%, p = 0.92 for heterogeneity). Aspiration and abdominal distention did not differ between groups (RR, 0.69; 95% CI, 0.44-1.08; I2 0%, p = 0.35 for heterogeneity and RR, 0.86;95% CI, 0.70-1.06; I2 0%, p = 0.32 for heterogeneity respectively, forest plots not shown). Diarrhea was evaluated by three studies and its occurrence was 15% lower in the underfeeding group (RR, 0.85; 95% CI, 0.75-0.96; I2 0%, p = 0.78 for heterogeneity) (23-25).

Discussion
This systematic review and meta-analysis of RCTs enabled us to assess the effects of two different feeding strategies on clinical outcomes and gastrointestinal tolerability in critically ill patients. Studies analyzed were not associated with differences in overall mortality (21-25). Subgroup analysis showed different effects according to the achieved energy intake. In the moderate feeding subgroup that reached 46-72% of the energy requirement (21,22,25), overall mortality was significantly lower in the underfeeding group than in the full-feeding one. This adequacy fits the proposed minimum cutoff value suggested by ASPEN (6) for the first week of ICU and is similar to the average adequacy found in international multicenter studies (26,27). No differences were found in the trophic feeding subgroup (23,24) that reached 16-25% of requirements. The two strategies evaluated in this study were not associated with differences in ICU mortality, ICU and hospital LOS, duration of MV and infectious complications.
Early EN is considered a therapeutic strategy associated with decreased disease severity and complications, as well as reduced ICU LOS (6,28,29). Among the reasons for offering early EN, maintaining the gut integrity and systemic immune response system should to be considered. However, despite the recommendation of early EN by current clinical practice guidelines, it remains unclear how much energy critically ill patients should consume considering the conflicting evidence in support of both initial underfeeding and full-feeding strategies (7,11,22-25,30,21).
Concerning gastrointestinal signs and symptoms, this study found some interesting data. Unlike the study by Choi et al. (32), which pooled data on the incidence of serious gastrointestinal intolerance (vomiting, regurgitation and diarrhea) and found no differences between feeding strategies, we decided to observe gastrointestinal signs and symptoms separately to better understand the effects of the strategies evaluated in the results. Underfeeding was associated with low occurrence of all upper digestive intolerance signs and symptoms and the protective effect ranged from 21% for vomiting to 61% for elevated GRV occurrence. Upper digestive intolerance signs and symptoms are associated with a higher incidence of nosocomial pneumonia, longer ICU stays and higher ICU mortality (33). Data show that symptoms occur early, and are more frequent in patients using sedation or catecholamines (33). For lower gastrointestinal tract symptoms, underfeeding showed the same trend, lowering the occurrence by 15% for diarrhea and 33% for constipation. Abdominal distention was not different between the groups. Diarrhea, which is the gastrointestinal symptom most commonly experienced by critically ill patients, and the respective contribution of feeding, were explored by Thibault et al. (34). They reported that the median day of diarrhea onset was the sixth day and that most patients had ≤ 4 diarrhea days. As an important result, enteral covering of > 60% of the energy target was associated with 75% more occurrences of diarrhea. These findings are consistent with our observations that diarrhea was less frequent in the underfeeding group. Constipation, a prevalent symptom in critically ill patients (35,36), is associated with delays in weaning from MV that can be explained by distention, discomfort and restlessness experienced by patients and by the inability of the ventilator muscle to cope with increased workload caused by distention (35). Early defecation is associated with a shorter duration of MV and ICU length of stay (37,38). Even after multivariate analysis, observational data showed lower incidence of constipation when early EN was implemented (36). Our results are consistent with these findings, since underfeeding was associated with the symptom occurring 33% less. The above may suggest that the benefit could center on the introduction of nutrients in the gastrointestinal tract rather than in the achievement of energy targets. No difference was found for aspiration, a symptom that occurred rarely (one study (23) reported one episode in the underfeeding group and other (24) reported the occurrence of 0.2-0.3% of feeding days).
Although the literature search was conducted in multiple databases and no restrictions concerning language, publication date or publication status were imposed, this meta-analysis has some limitations. First, the small numbers of studies retrieved did not allow us to perform meta-regression. We were able to perform subgroup analysis which allowed us to better understand the differences between full-feeding and underfeeding strategies (trophic and moderate feeding). However, the analysis was conducted using only two studies and three studies, respectively, so these findings should be interpreted cautiously. Second, none of the study design used a double-blind format. Third, studies did not report data of all outcomes evaluated in this meta-analysis, so some analyses included two or three studies.
Concerning the methodology of the studies included, none of them performed indirect calorimetry to measure resting energy expenditure and thus accurately assess energy requirements (6,39,40). The absence of a gold standard method to quantify requirements is an important limitation of all the studies included, since the prevalence of underprescription or overprescription of energy needs in critically ill mechanically ventilated patients is high when predictive equations or weight-based fixed prescriptions are compared to estimates of indirect calorimetry values (38% and 12%, respectively) (41). Thus, the standard caloric requirements and the goals of caloric intake set by the strategies evaluated (full-feeding versus underfeeding) probably fail to match the actual energy needs. Futhermore, studies used different methods to calculate caloric requirements (kcal/kg, kcal/kg of nonprotein calories, Harris-Benedict equations adjusted for stress factors), thus comparisons among studies are challenging because some patients in one study may have received more calories than other patient in other study regardless of the intervention group.
It is important to consider that full-feeding strategies did not achieve their energy targets, ranging from 71-93% of requirements, and none of the studies actually achieved their endpoints. Thus, groups were energy deprived and the studies compared underfeeding versus severe underfeeding, common situation in prospective nutrition studies in critical care setting (42). The lower limit achieved in the full-feeding strategy (71% of goal) was actually lower than the upper limit achieved in the underfeeding strategy (moderate feeding - 72% of goal). This overlap of the adequacy between the groups addresses a serious problem in the interpretation of results.
None of the studies analyzed body composition, so the nutritional status is represented only by BMI, which has limitations for critically ill patients. The mean BMI ranged from 25.0 (21) to 30.4 kg/m2 (23). Although the standard deviation has been considered, undernourished patients are not well represented, thus preventing generalization of the conclusions to this extreme end of the population. Studies did not show hypoglycemia or worse indicators of malnutrition in the population submitted to moderate nutrition (22,25). Patients with prior malnutrition were not specifically contemplated. Alberda et al. found association between energy supply and clinical outcomes between different BMI (43). In this study, patients with BMI < 20 kg/m2 showed reduction in mortality with full energy supply strategy. This is a key-point on treatment and possibly a limitation for intentional underfeeding in patients with previous malnutrition. Decrease in weight prior to admission would be a better tool to evaluate degree of malnutrition. Another strategy for better assessment would be the use of a specific tool to assess nutritional risk (such as NUTRIC - Nutrition Risk in Critically Ill - score) (44), which would allow the identification of those who may benefit from aggressive nutritional therapy.
Recently, three RCTs compared underfeeding with full-feeding nutritional support in critically ill patients (45-47). They were excluded from our analysis due to the use of supplementary parenteral nutrition. One study found more nosocomial infections in the underfeeding group while there was no significant effect on ICU and hospital mortality and duration of MV (45). Another found no differences regarding infections, ICU and hospital LOS and mortality (47). The last study found no differences in length of MV, hospital or ICU stay and infection but was prematurely interrupted at the first interim analysis with the observation of a statistically significant increase in mortality in the full-feeding group. These findings should be interpreted cautiously considering that a post hoc analysis is needed to determine which aspects of the intervention resulted in higher mortality (46).
Conclusion
This meta-analysis found no differences in ICU and overall mortality ICU and hospital LOS, duration of MV, and infectious complications when underfeeding and full -feeding were compared. In the subgroup analysis, moderate feeding (46-72% of energy intake) was associated with lower overall mortality (21,22,25) compared with the full-feeding group. These results are in accordance with the minimum cutoff value proposed for the first week in the ICU (6) and the average adequacy found worldwide in multicenter studies (26,27). Underfeeding was associated with fewer occurrences of gastrointestinal signs and symptoms evaluated. The results should be cautiously interpreted due to the small number of studies analyzed and their methodology. Large multi-center RCT that measure resting energy expenditure as a guide for nutritional therapy and achieve both caloric goals will likely allow for a more definitive evaluation of feeding strategies for critically ill patients.
References
1. Hoffer LJ, Bistrian BR. Why critically ill patients are protein deprived. JPEN J Parenter Enteral Nutr 2013;37:300-9. DOI: 10.1177/014860711.3478192. [ Links ]
2. Pasquini TA, Neder HD, Araujo-Junqueira L, et al. Clinical outcome of protein-energy malnourished patients in a Brazilian university hospital. Braz J Med Biol Res 2012;45:1301-7. DOI: 10.1590/1414-431X20122586. [ Links ]
3. Elke G, Wang M, Weiler N, et al. Close to recommended caloric and protein intake by enteral nutrition is associated with better clinical outcome of critically ill septic patients: secondary analysis of a large international nutrition database. Crit Care 2014;18:R29. DOI: 10.1186/cc13720. [ Links ]
4. Dhaliwal R, Cahill N, Lemieux M, Heyland DK. The Canadian critical care nutrition guidelines in 2013: an update on current recommendations and implementation strategies. Nutr Clin Pract 2014;29:29-43. DOI: 10. 1177/0884533613510948. [ Links ]
5. Nunes ALB, Koterba E, Alves VGF, et al. Terapia Nutricional no Paciente Grave.2011. http://diretrizes.amb.org.br/_BibliotecaAntiga/terapia_nutricional_no_paciente_grave.pdf. [ Links ]
6. McClave SA, Martindale RG, Vanek VW, et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2009;33:277-316. DOI: 10.1177/0148607109335234. [ Links ]
7. Villet S, Chiolero RL, Bollmann MD, Revelly JP, Cayeux RNM, Delarue J, et al. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin Nutr 2005;24:502-9. DOI: 10.1016/j.clnu.2005.03.006. [ Links ]
8. Doig GS, Simpson F, Finfer S, et al. Effect of evidence-based feeding guidelines on mortality of critically ill adults: a cluster randomized controlled trial. JAMA 2008;300:2731-41. DOI: 10.1001/jama.2008.826. [ Links ]
9. Casaer MP, Mesotten D, Hermans G, et al. Early versus late parenteral nutrition in critically ill adults. N Engl J Med 2011;365:506-17. DOI: 10.1056/NEJMoa1102662. [ Links ]
10. Heilbronn LK, de Jonge L, Frisard MI, et al. Effect of 6-month calorie restriction on biomarkers of longevity, metabolic adaptation, and oxidative stress in overweight individuals: a randomized controlled trial. JAMA 2006;295:1539-48. DOI: 10.1001/jama.295.13.1539. [ Links ]
11. Krishnan JA, Parce PB, Martinez A, et al. Caloric intake in medical ICU patients: consistency of care with guidelines and relationship to clinical outcomes. Chest 2003;124:297-305. [ Links ]
12. Dickerson RN, Boschert KJ, Kudsk KA, et al. Hypocaloric enteral tube feeding in critically ill obese patients. Nutrition 2002;18:241-6. [ Links ]
13. Higgins G. Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration. 2011. www.cochrane-handbook.org. [ Links ]
14. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol 2009;62:e1-34. DOI: 10.1016/j.jclinepi.2009.06.006. [ Links ]
15. Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 1959;22:719-48. [ Links ]
16. Greenland S, Robins JM. Estimation of a common effect parameter from sparse follow-up data. Biometrics 1985;41:55-68. [ Links ]
17. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177-88. [ Links ]
18. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50:1088-101. [ Links ]
19. Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629-34. [ Links ]
20. TNC C. Review Manager. The Cochrane Collaboration, Copenhagen, 2014. [ Links ]
21. Desachy A, Clavel M, Vuagnat A, et al. Initial efficacy and tolerability of early enteral nutrition with immediate or gradual introduction in intubated patients. Intensive Care Med 2008;34:1054-9. DOI: 10.1007/s00134-007-0983-6. [ Links ]
22. Arabi YM, Tamim HM, Dhar GS, et al. Permissive underfeeding and intensive insulin therapy in critically ill patients: a randomized controlled trial. Am J Clin Nutr 2011;93:569-77. DOI: 10.3945/ajcn.110.005074. [ Links ]
23. Rice TW, Mogan S, Hays MA, et al. Randomized trial of initial trophic versus full-energy enteral nutrition in mechanically ventilated patients with acute respiratory failure. Crit Care Med 2011;39:967-74. [ Links ]
24. Rice TW, Wheeler AP, Thompson BT, et al. Initial trophic vs full enteral feeding in patients with acute lung injury: the EDEN randomized trial. JAMA 2012;307:795-803.DOI: 10.1001/jama.2012.137. [ Links ]
25. Arabi YM, Aldawood AS, Haddad SH, et al. Permissive Underfeeding or Standard Enteral Feeding in Critically Ill Adults. N Engl J Med 2015;372:2398-408. DOI: 10.1056/NEJMoa1502826. [ Links ]
26. Heyland DK, Dhaliwal R, Wang M, et al. The prevalence of iatrogenic underfeeding in the nutritionally 'at-risk' critically ill patient: Results of an international, multicenter, prospective study. Clin Nutr 2015;34:659-66. DOI: 10.1016/j.clnu.2014.07.008. [ Links ]
27. Cahill NE, Dhaliwal R, Day AG, et al. Nutrition therapy in the critical care setting: what is "best achievable" practice? An international multicenter observational study. Crit Care Med 2010;38:395-401. DOI: 10.1097/CCM.0b013e3181c0263d. [ Links ]
28. DOIg GS, Heighes PT, Simpson F, et al. Early enteral nutrition, provided within 24 h of injury or intensive care unit admission, significantly reduces mortality in critically ill patients: A meta-analysis of randomised controlled trials. Intensive Care Med 2009;35:2018-27. DOI: 10.1007/s00134-009-1664-4. [ Links ]
29. Doig GS, Heighes PT, Simpson F, et al. Early enteral nutrition reduces mortality in trauma patients requiring intensive care: A meta-analysis of randomised controlled trials. Injury 2011;42:50-6. DOI: 10.1016/j.injury.2010.06.008. [ Links ]
30. Faisy C, Lerolle N, Dachraoui F, Savard JF, Abboud I, Tadie JM, et al. Impact of energy deficit calculated by a predictive method on outcome in medical patients requiring prolonged acute mechanical ventilation. Br J Nutr 2009;101:1079-87. DOI: 10.1017/S0007114508055669. [ Links ]
31. Singer P, Anbar R, Cohen J, et al. The tight calorie control study (TICACOS): a prospective, randomized, controlled pilot study of nutritional support in critically ill patients. Intensive Care Med 2011;37(4):601-9. DOI: 10.1007/s00134-011-2146-z. [ Links ]
32. Choi EY, Park DA, Park J. Calorie intake of enteral nutrition and clinical outcomes in acutely critically ill patients: a meta-analysis of randomized controlled trials. JPEN J Parenter Enteral Nutr 2015;39:291-300. DOI: 10. 1177/0148607114544322. [ Links ]
33. Mentec H, Dupont H, Bocchetti M, Cani P, Ponche F, Bleichner G. Upper digestive intolerance during enteral nutrition in critically ill patients: frequency, risk factors, and complications. Crit Care Med 2001;29:1955-61. [ Links ]
34. Thibault R, Graf S, Clerc A, et al. Diarrhoea in the ICU: respective contribution of feeding and antibiotics. Crit Care 2013;17:R153. DOI: 10.1186/cc12832. [ Links ]
35. Mostafa SM, Bhandari S, Ritchie G, et al. Constipation and its implications in the critically ill patient. Br J Anaesth 2003;91:815-9. [ Links ]
36. Nassar AP Jr, da Silva FM, de Cleva R. Constipation in intensive care unit: incidence and risk factors. J Crit Care 2009;24:630.e9-12. DOI: 10.1016/j.jcrc.2009.03.007. [ Links ]
37. Van der Spoel JI, Schultz MJ, van der Voort PH, et al. Influence of severity of illness, medication and selective decontamination on defecation. Intensive Care Med 2006;32:875-80. DOI: 10.1007/s00134-006-0175-9. [ Links ]
38. Van der Spoel JI, Oudemans-van Straaten HM, Kuiper MA, et al. Laxation of critically ill patients with lactulose or polyethylene glycol: a two-center randomized, double-blind, placebo-controlled trial. Crit Care Med 2007;35:2726-31. DOI: 10.1097/01.CCM.0000287526.08794.29. [ Links ]
39. Bursztein S, Elwyn D, Askanazi J, et al. Energy metabolism, indirect calorimetry and nutrition. En: Wilkins W editor. Energy metabolism, indirect calorimetry and nutrition. Baltimore, Maryland, USA; 1989; p. 27-83. [ Links ]
40. Singer P, Berger MM, Van den Berghe G, et al. ESPEN Guidelines on Parenteral Nutrition: intensive care. Clin Nutr 2009;28:387-400. DOI: 10.1016/j.clnu.2009.04.024. [ Links ]
41. Tatucu-Babet OA, Ridley EJ, Tierney AC. The prevalence of underprescription or overprescription of energy needs in critically ill mechanically ventilated adults as determined by indirect calorimetry: A systematic literature review. J Parenter Enteral Nutr 2016;40:212-25. DOI: 10.1177/0148607114567898. [ Links ]
42. Singer P, Cohen J. Please sir, may I have some more? The case against underfeeding. Ann Transl Med 2015;3:173. DOI: 10.3978/j.issn.2305-5839.2015.07.19. [ Links ]
43. Alberda C, Gramlich L, Jones N, et al. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med 2009;35:1728-37. DOI: 10.1007/s00134-009-1567-4. [ Links ]
44. Heyland DK, Dhaliwal R, Jiang X, Day AG. Identifying critically ill patients who benefit the most from nutrition therapy: the development and initial validation of a novel risk assessment tool. Crit Care 2011;15:R268. DOI: 10.1186/cc10546. [ Links ]
45. Petros S, Horbach M, Seidel F, et al. Hypocaloric vs Normocaloric Nutrition in Critically Ill Patients: A Prospective Randomized Pilot Trial. JPEN J Parenter Enteral Nutr 2016;40:242-9. DOI: 10.1177/0148607114528980. [ Links ]
46. Braunschweig CA, Sheean PM, Peterson SJ, et al. Intensive nutrition in acute lung injury: a clinical trial (INTACT). JPEN J Parenter Enteral Nutr 2015;39:13-20. DOI: 10.1177/0148607114528541. [ Links ]
47. Charles EJ, Petroze RT, Metzger R, et al. Hypocaloric compared with eucaloric nutritional support and its effect on infection rates in a surgical intensive care unit: a randomized controlled trial. Am J Clin Nutr 2014;100:1337-43. DOI: 10.3945/ajcn.114.088609. [ Links ]
![]() Correspondence:
Correspondence:
Oellen Stuani Franzosi.
Hospital de Clínicas de Porto Alegre.
Rua Ramiro Barcelos.
90035-003. Porto Alegre.
RS - Brazil
e-mail: oellen.franzosi@gmail.com
Received: 04/08/2016
Accepted: 10/12/2016
