










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkBACKGROUND
All over the world and most strikingly in developed countries, population is aging. In 2010, world elderly population (above 65 years old) should represent about 8% of total world population, which corresponds to more than 500 million people 1. In 2050, it is expected that this elderly population reach about 1.500 million, 16% of total world population. The increase number of older citizens is creating new social and clinical problems. Neurologic disorders increase with age. Also, most cancers, including head and neck cancer, are more frequent in elderly patients. Neurologic disorders and head and neck cancer share an important clinical feature: they both cause dysphagia and long standing dysphagia is the major clinical indication for percutaneous endoscopic gastrostomy (PEG) 2. This aging population in developed countries is creating an increasing number of PEG fed patients.
Endoscopic gastrostomy is generally considered a safe procedure with very low mortality and unusual severe morbidity 3. Some complications may eventually occur and becoming more and more frequent due to the high number of patients usually fed through the gastrostomy for months and years 3. Migration of the PEG tube is considered a rare complication of long term enteral feeding. Indeed, standard PEG tubes have external bumpers that prevent migration into the stomach and duodenum. Most of the rare cases of migration into the duodenum were reported with Foley-type tubes that, unlike standard PEG tubes, do not have external bumpers. Nevertheless, Foley tubes are still used because they are cheaper than standard PEG tubes and widely available in nursing homes and other health facilities.
CASE REPORT
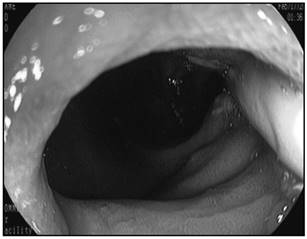
A 73 years old woman was admitted in the emergence room with a two days history of vomiting. She suffered a stroke two years before and she was fed using an endoscopic gastrostomy. Since the discharge after the stoke, the patient was followed in the Artificial Nutrition Outpatient Consultation of our Hospital. Gastrostomy tubes were regularly changed each 4-6 months. One week before the vomiting episode, the patient accidentally pulled out her PEG tube. A Foley catheter was passed in order to replace the PEG tube and the patient was fed through this catheter for a few days. Two days before hospital admission she started vomiting after each meal. At the same time, the Foley catheter was pulled into the stomach leaving just the proximal tip in the PEG gastrocutaneous tract (Fig. 1). An upper GI endoscopy was performed showing the catheter pulled into the duodenum (Fig. 2) where the balloon caused obstruction. The balloon was deflated and removed. A 24Fr PEG tube was passed and the patient resumed gastrostomy feeding immediately without any problem.

DISCUSSION
Inadvertent removal of PEG tube occurs in 1.6% to 4.4% of patients 3. In order to maintain the feeding access and prevent spontaneous closure of the gastrocutaneous tract, the tube must be replaced as soon as possible. A large percentage of PEG fed patients is bedridden or has major motility impairment, living in nursing homes or other institutions.
These patients are difficult to move to a hospital where experience enteral feeding teams can provide adequate tube replacement. In many occasions, replacing the PEG tube by a Foley catheter is appealing. Furthermore, some articles support this option. In a 1994 study, 46 patients were randomized for replacement with standard PEG tubes or Foley catheters. They used both tubes during several weeks and neither the Foley catheter nor the standard replacement gastrostomy tube migrated into duodenum 4. To the best of our knowledge, there was no other prospective study evaluating the replacement of PEG tubes with Foley-type catheters but some teams kept advocating this procedure 5. That is not the experience of our enteral feeding team as over the years we had several cases of tube migration with duodenal obstruction, like the one described above, and others previously reported in literature 6,7,8. This is not only our experience since over the years a large number of migrations were also reported, including in children 9 and occasionally causing pancreatitis 10. Most of these duodenal migrations are caused by Foley-type catheters 3. Each hospital or institution should have an optimal protocol for PEG tube replacement 11. Replacement of PEG tubes using Foley catheters in institutions without experienced teams and established protocols increases the risks of severe complications.
CONCLUSION
Replacement of PEG tubes should be performed by experienced teams in institutions with comprehensive protocols and always using standard PEG tubes. According with our experience, the use of Foley-type catheters that may migrate into the duodenum and cause obstruction is occasionally performed in institutions with little experience, nevertheless this strategy is dangerous and should be banned.

