










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The visceral fat component is the adipose tissue compartment most strongly associated with cardiometabolic complications 1,2,3, but its precise quantification requires high cost imaging studies, making its use in population studies and clinical practice unfeasible. For this reason, there is an increasing search for a simple, inexpensive, and easy-to-apply tool to assess visceral adiposity.
Because excess visceral fat is an independent risk factor for the development of cardiovascular diseases and is related to associated with dyslipidemia, systemic arterial hypertension, insulin resistance, and subclinical inflammation 4,5, the formulation of an indicator that can be routinely applicable is of importance to evaluate this fat as it would allow its wide use.
Recently, the visceral adiposity index (VAI) has been proposed as an indicator of fat distribution and function 6 and considered as a predictor of cardiometabolic risk 7. VAI is gender-specific and takes up simple anthropometric parameters such as waist circumference (WC) and body mass index (BMI), as well as the metabolic parameters triglyceride (TG) and high-density lipoprotein (HDL-c). VAI showed a high correlation with the visceral fat measured by magnetic resonance 6, in addition to association with cardiometabolic risk 8, metabolic syndrome 9, diabetes 10, and hypertension 11.
Population-based studies have not yet been conducted to determine which factors are associated with VAI in the Brazilian adult population and how this occurs, with his gap remaining unexplained. Therefore, the objective of this study was to analyze the association of socioeconomic, demographic, anthropometric, body composition, behavioral and biochemical factors with VAI in Brazilian adults.
MATERIALS AND METHODS
STUDY DESIGN AND SAMPLE CALCULATION
The current research was conducted as a cross-sectional, population-based study from 2012 to 2014. Data were obtained from a research that aimed to evaluate the health conditions of the adult population of Viçosa, Minas Gerais, Brazil. The study was approved by the Ethics Committee in Research of the Federal University of Viçosa (Regulation 02/2013 / CEP / 07.12.13) and its procedures are described in Segheto et al. 12.
Study sample consisted of adult individuals aged 20 to 59 years, of both sexes and living in the urban area of the municipality. For the sample calculation of this outcome, 43,431 individuals were considered as reference population 13, confidence level of 95.0%, expected prevalence of 50%, predicted sample error of 4.5 percentage points, and a design effect of 1.5. The obtained value was added with 10% of losses and refusals and 10% more to control confounding factors, requiring a minimum sample of 844 individuals. As this study is part of a survey that aims to evaluate different outcomes, 854 individuals were included who had the complete data for the calculation of VAI and TG ≤ 279 mg/dL and BMI ≤ 40 kg/m2 (14. The sampling process was probabilistic, without replacement, and used a two-stage conglomerate sampling (census and domicile).
DATA COLLECTION
Data collection was carried out in two stages: the first stage was conducted in the domiciles, by applying a structured questionnaire, while the second stage was carried out in the university's premises, using the anthropometric evaluations body composition and biochemical parameters. Initially, a total of 30 census tracts were selected among the 99 existing in the urban area of the municipality, then, the blocks and the starting corner of the data collection were randomly chosen. After identification of the households, all the adults residing in them were invited to participate in the study, considering as criteria for non-inclusion the pregnant women, individuals who were bedridden or unable to undergo anthropometric measurements and those unable to answer the questionnaires.
STUDY VARIABLES
VAI was considered the dependent variable and was calculated from the equations described below 6 and analyzed in tertile.

The socioeconomic, demographic, behavioral, anthropometric, body composition and biochemical characteristics were investigated as independent variables.
The socioeconomic and demographic variables included sex, age group in years, skin color categorized as white and non-white; schooling categorized into 0-4 years, 5-8 years, 9-11 years and ≥ 12 years, marital status categorized as with and without partner, and socioeconomic status grouped into higher (A + B), intermediate (C) and lower (D + E).
The variables related to the behavior were leisure-time physical activity (LTPA) and sedentary behavior. LTPA was evaluated by the International Physical Activity Questionnaire (IPAQ), long form, using the fourth domain. The LTPA was calculated by adding the time spent with moderate physical activities plus twice the time with vigorous activities, within the categories insufficiently active (< 150 minutes of activities in the week) or physically active (≥ 150 minutes of activities) 15. The sedentary behavior was evaluated by the sitting time (ST) calculated by the average of time (minutes) spent sitting on weekdays. TS was categorized into ≤ 300 minutes and > 300 minutes per day.
The anthropometric variables measured were BMI, WC and neck circumference (NC), all in triplicate, using the average. The criteria proposed by the World Health Organization (WHO) 16 were used for BMI. Normal-weight individuals were grouped into the normal weight category. WC and NC were measured respectively at the midpoint between the last rib and the iliac crest and below the laryngeal prominence.
The female body composition was estimated by the triceps, abdominal, and thigh skinfolds, and male body composition by triceps, pectoral and subscapular skinfolds. Skinfold data were used in sex-specific equation to calculate body density 17,18, then the fat percentage was estimated by the Siri equation 19. The skinfolds were measured using a Lange caliper (Cambridge Scientific Industries, Inc., Cambridge, MD), 1 mm precision.
The biochemical variables measured were HDL-c, TG, uric acid (UA) and ultra-sensitive C-reactive protein (us-CRP). Blood samples were collected for dosages after a 12-hour fast by venipuncture using a vacutainer system (Becton Dikinson, UK). HDL-c was measured by the enzymatic colorimetric method, TG and UA with commercial kits and us-CRP by the immunoturbidimetric assay.
STATISTICAL ANALYSIS
Data analysis was conducted using the statistical program Stata (Version 13.1, StataCorp, College Station, Texas). Considering the complex nature of the sample, the command set "svy" was used, with sample weights assigned to the variables sex, age and schooling 13.
A descriptive analysis was carried out and association was found between the VAI and the independent variables by the ordinal logistic regression. After analyzing the independent variables in the multiple regression model, the variables that were associated with the outcome with p < 0.05 were maintained in the final model.
RESULTS
We evaluated 854 individuals, 392 males and 462 females. Regardless of sex, most individuals evaluated were not white (men 57.81% CI 95% 48.01-67.03 and women 60.60% CI 95% 51.83-68.73), had 12 or more years of schooling (men 55.20% CI 95% 40.11-69.38% and women 45.60% CI 95% 33.98-57.70), and were defined as intermediate socioeconomic status (men 63.42% CI95% 56.35-69.95 and women 68.44% CI95% 61.69-74.48) (Table I).
Table I Demographic and socioeconomic characteristics of adults assessed by sex, Viçosa, MG, Brazil, 2012-2014 (n = 854)
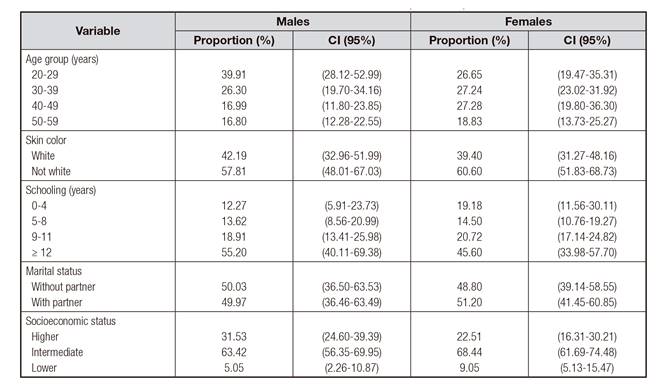
CI: confidence interval; ≥ greater than or equal to.
Except for LTPA in the female sex and ST in both sexes, all other parameters evaluated showed a significant difference between the third and the first VAI tertiles (Table II).
Table II Distribution (mean ± SE and 95% confidence interval) of the anthropometric variables, body composition, biochemical and behavioral variables, according to VAI tertiles in adults. Viçosa, MG, Brazil, 2012/2014 (n = 854)

SE: standard error; VAI: visceral adiposity index - VAI Tertile of men (tertile 1: 0.211-0.889; tertile 2: 0.891-1.667; tertile 3: 1.676-7.840) - VAI Tertile of women (tertile 1: 0.309-1.049; tertile 2: 1.059-1.667; 1.059-1.667; tertile 3: 1673-1750); NC: neck circumference; %: Percentage; UA: uric acid; us-CRP: ultra-sensitive c-reactive protein; LTPA: leisure-time physical activity; ST: sitting time. Bold numbers and different letters indicate statistical difference.
The percentage of fat, uric acid and C-reactive protein concentration in the blood were positively and independently associated with VAI in the male sex, while the leisure-time physical activity level was independent and negatively associated with VAI. A positive and independent association was found in females for increase in age, neck circumference, sitting time over 300 minutes, increased uric acid concentration and C-reactive protein in blood (Table III).
Table III Final model of the ordinal logistic regression for factors associated with the visceral adiposity index in adults. Viçosa, MG, Brazil, 2012-2014 (n = 854)

OR: odds ratio; CI: confidence interval; %: Percentage; NC: neck circumference; LTPA: leisure-time physical activity; ST: sitting time; UA: uric acid; us-CRP: ultra-sensitive C-reactive protein.
DISCUSSION
This is the first study evaluating the association of socioeconomic, demographic, anthropometric, body composition, behavioral and biochemical factors with VAI in Brazilian adults and may serve as a basis for conducting longitudinal studies aimed to assess the risk of increase in VAI and its association with comorbidities.
We found a positive and independent association between VAI and increase in age for women (OR 1.04 CI 95% 1.01-1.07), with a significant increase in age between the third (41.85 ± 1.361 CI 95% 39.06-44.64) and the first terciles (34.16 ± 1.135 95% CI 31.84-36.49) of VAI in both sexes.
Previous studies 20,21 have shown that advancing age leads to an increase in visceral adiposity, reinforcing the need to evaluate this adiposity in different age groups. Possible explanations for this association in women are changes in lifestyle that promote decreased levels of physical activity and consequently change in basal metabolism, as well as changes in hormone levels in particular after menopause 21.
The increase in the percentage of total fat was positively associated in men (OR 1.14 95% CI 1.09-1.18), indicating that an increase in overall adiposity in this group also leads to an increase in visceral adiposity, which may compromise health 22,23.
We found that increase in NC was also positively associated with VAI independently in women (OR 1.28 95% CI 1.15-1.44). NC is a simple marker of upper body adiposity, and a synergistic effect between this measure and visceral adipose tissue with cardiometabolic risk factors was observed in the Framingham Heart Study 24. It is worth noting that fat located in the upper part of the body can cause metabolic abnormalities, increasing circulating free fatty acids, which can lead to insulin resistance 25,26.
In our study, we found that being active contributed to a 46% reduction in the chance of increased visceral adiposity among men (OR: 0.54 95% CI 0.35-0.83), constituting a protective factor. LTPA was statistically lower in men who had higher VAIs (82.71 ± 19.73 CI 95% 42.29-123.13) than in those with lower VAI (194.90 ± 30.29 CI 95% 132.85-256.96). Inverse association between LTPA and obesity has previously been demonstrated 27, reinforcing the benefits of an active life in body composition.
Our results also showed that sedentary behavior time > 300 minutes in women was independently and positively associated with VAI (OR 2.10 95% CI 1.11-3.97). Previous studies have shown association between greater time spent in sedentary behavior and greater waist circumference (1.89 95% CI 0.94-2.83 cm) 28, as well as higher risk of overweight and obesity (OR 1.38 95% CI 1.26-1.52) 29. The physiological effect of sedentary behavior promoting unhealthiness may result from the absence of muscle contraction that leads to an increase in triglycerides, plasma glucose and a reduction in lipoprotein lipase activity, which is an enzyme related to the regulation of triglyceride absorption and the production of HDL-c in skeletal muscles 30.
Identifying differences between the sexes in the association of LTPA and sedentary behavior with VAI is important for proposing specific intervention strategies for this adult population. This study suggests that physical activity should be encouraged for men to reduce the chance of increasing VAI, while for women the greatest encouragement should be to decrease sitting time as this more than doubles the chance of increasing VAI.
We observed that in both sexes the increase in UA concentration was positively associated (OR: 1.42 CI 95% 1.14-1.78 in men; OR: 1.50 CI 95% 1.14-1.98 in women). The association between high concentration of UA with factors such as obesity, hypertriglyceridemia, hypertension, diabetes and consequently metabolic syndrome has been demonstrated in the Brazilian adult population 31, as well as a correlation between VAI and UA 9 in adult Chinese, suggesting the possibility of using VAI to predict inflammation. Recently, an association between increased UA and visceral and subcutaneous adipose tissue was described, but the association was lost when the effect of visceral adipose tissue was controlled 32.
Increase in us-CRP concentration was also positively associated in both sexes (OR: 1.19 95% CI 1.05-1.35 in men; OR: 1.19 CI 95% 1.06-1.33 in women). As us-CRP is a marker for low-grade inflammation, its association with IAV suggests that it may also indicate inflammation. Recent research on the impact of the number of risk factors for metabolic syndrome on the serum concentration of us-CRP in women and men has shown that even in absence of evident disease and pharmacological treatment, individuals with risk factors for metabolic syndrome already have an increased concentration of us-CRP 33. Correlation between VAI and us-CRP in women (0.19 p < 0.005) has been previously demonstrated 34, corroborating with our study, as well as the increase observed in us-CRP as the tertile value of VAI increases both in pre-diabetes (OR 2,17 CI 95% 1,40-3,37) and type 2 diabetes (OR 1,17 95% CI 1,16-2,71) 35.
Some limitations of this study are that the transversal design does not allow us to establish a temporal relation between the exposure and the outcome, but this was not the objective of our study. The proportion of selected individuals had no correspondence to data referring to the Viçosa population for sex, schooling, and age, which was corrected by weighing the sample means. Finally, a questionnaire was used to estimate LTPA and quantification of sitting time as an indicator of sedentary behavior was memory dependent. However, we believe that when we evaluated LTPA with a validated questionnaire and took only the last week for the sitting time we were able to minimize these limitations.
Considering the data from this study, we conclude that there is a positive and independent association in men between VAI and the increase in fat percentage, in the concentration of UA and us-CRP in the blood, whereas a negative association was observed with LTPA. In women, the increase in age and NC, sitting time greater than 300 minutes, increase in AU concentration and us-CRP were the independent factors and positively associated with VAI. With the exception of age, the other factors are modifiable, suggesting that the adoption of early intervention measures that lead to changes in habits may alter the risk of increased visceral adiposity and, consequently, the appearance of comorbidities. However, more research on this topic needs to be undertaken to investigate the factors associated with VAI in different populations.

