










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Vitamin D gained prominence when it was discovered that its deficiency was associated with the pathogenesis of rickets in children and osteomalacia in adults (1). Subsequent investigations revealed that 25-hydroxyvitamin D also had biological action not only in bone diseases, but also in autoimmune diseases, inflammatory bowel disease, infections, immunodeficiencies, cancer, neurocognitive disorders, cardiovascular diseases and type 2 diabetes mellitus (DM2), as reviewed by Grober, Reichrath and Holick (2).
Evidence shows that vitamin D influences 1α-hydroxylase enzyme expression of β-pancreatic cells through interaction with a nuclear vitamin D receptor (VDR) (3). VDR is a member of the nuclear receptor superfamily (4) and exists in several tissues, which explains the biological role of vitamin D in some clinical conditions, such as type 2 diabetes mellitus (DM2) (5).
Different polymorphisms present in the VDR gene may interfere in the concentration and, especially, in the action of vitamin D (6). To the present, rs1544410 (BsmI), rs2228570 (FokI), rs7975232 (ApaI) and rs731236 (TaqI) are the VDR gene polymorphisms that have been extensively investigated under various clinical conditions, including glycemic behavior. In this sense, we have already found association of polymorphisms in the VDR gene with higher glycemic averages, insulin resistance and DM2 in different ethnic populations (7).
Fei et al. (8), however, warn that there are limitations in studies demonstrating this association of VDR polymorphisms with glycemia. Among these limitations, they refer to the statistical power of the studies, diverse clinical conditions and age, besides the great ethnic diversity. This may warrant literature reviews to show association of VDR with glycaemia; however, there are a variety of other studies where this association has not been demonstrated.
Brazil has continental dimensions and a history of different ethnic exploitation between regions. With the Brazilian population, for example, and in case of healthy adolescents, only two studies were performed: one by Santos et al. (9), with young girls between the ages of seven and 18, investigating the relationship between VDR gene polymorphisms with 25-hydroxyvitamin D levels; and another by Cobayashi, Lourenço and Cardoso (10), in children under ten years of age in the Amazon, with VDR gene polymorphisms and biochemical parameters such as 25-hydroxyvitamin D and glycemia. In the northeast region of Brazil, there are no studies evaluating the relationship of VDR gene polymorphisms with a glycemic profile in healthy adolescents.
Therefore, the objective of this study was to verify the association of serum concentrations of 25-hydroxyvitamin D and glycemic levels with the genetic variants rs1544410 and rs2228570 of the VDR gene in adolescents from the Northeast region of Brazil.
MATERIALS AND METHODS
SAMPLE
This was a cross-sectional study involving a random sample of 208 adolescents of both sexes, aged 15 to 19 years of public schools in the city of João Pessoa-PB, Northeast Brazil. The sample calculation considered 60 % (P) of prevalence of vitamin D deficiency/deficiency (9), with a margin of error of 10 % (D) and a level of significance of 5 % (z = 1.96), making up a minimum required total of 194 adolescents. In order to correct any losses, an increase of 10 % (100/[100-10]) was made, resulting in 216 sample units. From the universe of public schools in the city of João Pessoa, which met inclusion and exclusion criteria, the sample was selected using a random number table.
The inclusion criteria of the research were: adolescents between 15 and 19 years of age with preserved cognitive status, non-pregnant or lactating adolescents, nutritional status of thinness, non-users of vitamin D supplements and anticonvulsant drugs or for HIV/AIDS treatment, and who did not present diabetes, renal and hepatic disease or any other chronic consumptive disease. The protocol of this study was approved by the Ethics and Research Committee of the Health Sciences Center of the Federal University of Paraíba (CCS / UFPB) under protocol 0139/15, in compliance with Resolution 466/12 of the National Health Council.
Adolescents with 25-hydroxyvitamin D deficiency/deficiency were referred to the nutritional care service for dietary guidance and/or supplementation.
BIOCHEMICAL ANALYSES
Blood collection was performed in schools. The adolescents were advised about the day and time of the examination, as well as the need for a 12-hour fast. Subsequently, 25-hydroxyvitamin D, parathyroid hormone (PTH) and calcium (Ca) analyses were sent to the laboratory of the Physical Training Studies Applied to Development and Health at the Federal University of Paraíba.
Serum analysis of 25-hydroxyvitamin D and PTH were determined using the chemiluminescent immunoassay (UniCel® DxI 800 - Beckman Coulter), and the classification of vitamin D status was based on the reference values used by the Endocrine Society, which considers levels as deficient when 25-hydroxyvitamin D < 20 ng/ml; insufficient when 25-hydroxyvitamin D > 20 and < 30 ng/ml; and sufficient when 25-hydroxyvitamin D > 30 and < 100 ng/ml (11). Concentrations of Ca and fasting glucose were performed on a Labmax 240 Premium® automatic analyzer (Lagoa Santa, MG, Brazil), using commercial kits from the Labtest brand (Minas Gerais, Brazil), following the recommendations of the manufacturer.
GENOTYPE ANALYSIS
VDR polymorphisms
Genotypes were determined by polymerase chain reaction-restriction size polymorphism (PCR-RFLP). For the variant rs1544410 the primers: 5’-CAACCAAGACTACAAGTACCGCGTCAGTGA-3 ‘(sense) and 5’-AACCAGCGGGAA GTCAAGGG-3’ (antisense) (13). Amplification occurred under the following conditions: initial denaturation at 94 °C (ten minutes), 30 cycles of denaturation (one minute at 94 °C), annealing (one minute at 58 °C) and extension (three minutes at 72 °C), with an extra stage of final extension of ten minutes. The 825 bp product was digested with BsmI, which recognizes and cleaves polymorphic allele b generating two fragments (650 bp and another of 175 bp) while the ancestral allele B remains at 825 bp.
For the variant rs2228570, primers: 5’-AGCTGGCCCTGGCACTGACTCTGCTCT-3’ (sense) and 5’-ATGGAAACACCTTGCTTCTTCTCCCTC-3’ (antisense) (14). Amplification occurred under the following conditions: initial denaturation at 94 °C (five minutes), 35 cycles of denaturation (30 seconds at 94 °C), annealing (30 seconds at 60 °C) and extension (30 seconds at 72 °C), with an extra stage of final extension of ten minutes. The 265 bp product was digested with FokI, which recognizes and cleaves the polymorphic allele f generating two fragments (196 bp and the other 69 bp), while the ancestral allele F remains at 265 bp. The genotypes were analyzed by electrophoresis in 10 % polyacrylamide gel and 0.5 % silver nitrate staining.
STATISTICAL ANALYSIS
Continuous variables were tested for normality by the Kolmogorov-Smirnov test. The variables that presented non-Gausean distribution were transformed into natural logarithm and retested. Data were presented as mean and standard deviation (SD). Differences between genotype groups were tested using the non-parametric Kruskal-Wallis test, with Dunn’s post-test. For the association between the genotyping patterns and the biochemical parameters, the logistic regression model was used. A level of significance was adopted when p-value < 0.05. Statistical analysis was developed using STATA 14 Software (StataCorp; USA).
RESULTS
Data on the demographic and biochemical characteristics of adolescents are presented in table I. The total sample consisted predominantly of female adolescents, with an overall mean age of 17.7 (± 1.14) years, with boys 17.9 (± 1.22) years and girls 17.95 (± 1.06) years. Regarding the biochemical parameters, half of the sample was adequate and the other half insufficient/deficient of 25-hydroxyvitamin D. Considering the cutoff points for adolescents of Ca, PTH and glycemia, the means of these biochemical analyses were found normal. The median values of 25-hydroxyvitamin D = 28.0 (28.4-30.7) ng/ml; for sufficient of vitamin = 33.0 (35.1-38.3) ng/ml and insufficient/deficient = 25.0 (23.9-25.1) ng/ml; Ca = 10.1 (10.0-10.2) mg/dl; PTH = 27.0 (27.1-31.3) pg/ml; and glycemia 83.0 (83.5-86.0) mg/dl.
Table I. Demographic and biochemical characteristics in adolescents from Northeast Brazil

Data are expressed as mean and standard deviation (SD).
The distribution of the genotypes of both VDR gene polymorphisms studied as well as allelic frequency are presented in table II. For genotype rs1544410, bb was the most frequent and BB was the least frequent, resulting in more prevalent allelic distribution of b. The distribution of the rs2228570 polymorphism follows the higher frequency of the Ff genotype and lower frequency of ff, with the F allele being the most frequent of the sample. The haplotypes frequencies Bf, Bf, bF, bf for BsmI and FokI polymorphisms were respectively 0.27, 0.17, 0.34 and 0.22 (D’ = 0), meaning that the two loci are in linkage equilibrium.
Table II. Distribution of genotypes and allelic frequency of polymorphism rs1544410 and rs2228570 in adolescents from Northeast Brazil

Data are expressed as number of adolescents (n) and percentage (%).
Table III shows the values of the biochemical variables studied as a function of the distribution of the rs1544410 polymorph genotypes. A significant relationship between rs1544410 genotypes and glycemia values was observed (p = 0.049). Significance was observed in the relationships between the genotypes BBxbb (p = 0.012) and Bbxbb (p = 0.037). Adolescents who presented bb genotype appear to be more protected with glycemia. Table IV shows that there is no significant relationship between biochemical variables and polymorphism genotypes rs2228570.
Table III. Mean values of the biochemical variables as a function of the distribution of polymorphism genotypes rs1544410 in adolescents from Northeast Brazil

Ca: calcium; PTH: parathyroid hormone. Data are expressed as mean and standard deviation (SD).
*Different letters mean statistically significant differences by Dunn’s post test.
†Different letters mean statistically significant differences by Dunn’s post test.
‡p < 0.05 for Kruskal-Wallis.
Table IV. Mean values of the biochemical variables as a function of the distribution of genotypes of polymorphism rs2228570 in adolescents from Northeast Brazil

Ca: calcium; PTH: parathyroid hormone. Data are expressed as mean and standard deviation (SD).
The stratification of the sample into two groups of sufficient and insufficient/deficient 25-hydrixivitamin D was performed, however, no differences were found in the biochemical variables studied as a function of the distribution of the polymorph genotypes (data not shown in the table).
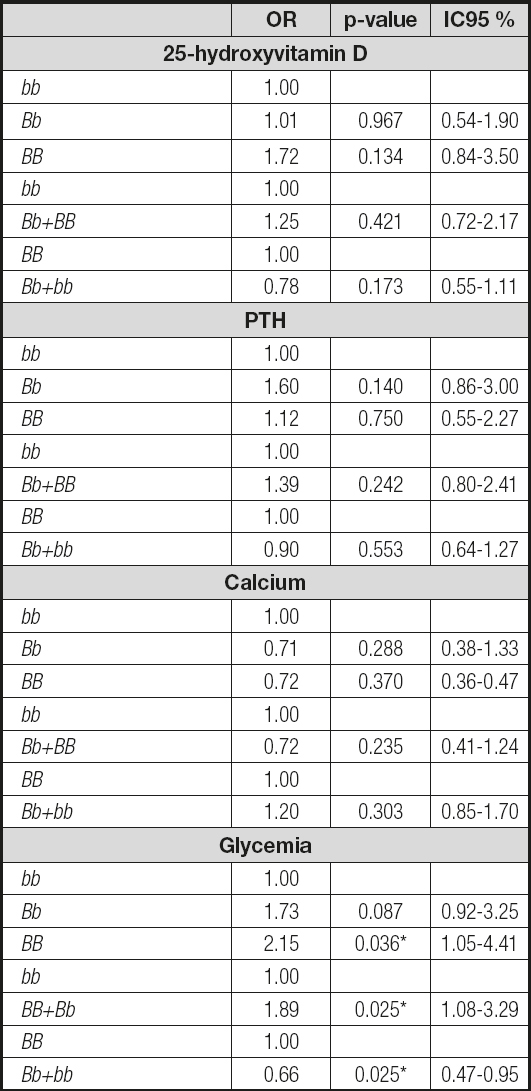
In the analysis of the logistic regression model, the concentrations of 25-hydroxyvitamin D, PTH, Ca and glycemia were related to the distribution of genotypes of rs1544410 polymorphism, and glycemia showed a significant relationship. Adolescents with BB genotype (OR = 2.15, 95 %; CI = 1.05-4.41) and group BB+Bb (OR = 1.89, 95 %; CI = 1.08-3.29) when compared to bb presented higher risk of glycemia above the median. On the other hand, when Bb+bb (OR = 0.65, 95 %; CI = 0.46-0.93) was analyzed in relation to BB, adolescents had a higher chance of having below-median glycemia (Table IV).
DISCUSSION
This study aimed to investigate the relationship between 25-hydroxyvitamin D and glycemia with the genotypic variants of polymorphisms rs1544410 and rs2228570. The glycemia was related to the distribution of rs1544410 genotypes.
In the literature, there are differences regarding the results of studies with variants of the VDR gene and concentrations of 25-hydroxyvitamin D (10). Santos et al. (9) studied Brazilian girls from the southern region, aged 7-18 years, and observed that variants of rs1544410 of the VDR gene were associated with low levels of 25-hydroxyvitamin D (p < 0.001), presenting significance in the Bb+bb genotypes (p = 0.014) in vitamin deficient subjects. Cobayashi et al. (10) found a significant association between the rs1544410 polymorphism variants with 25-hydroxyvitamin D, but did not find the rs2228570 variants in a study with children from the northern region of Brazil, younger than ten years. On the other hand, our findings corroborate a previous study conducted by researchers in our group (15), who did not find this association of polymorphimoses rs1544410 with serum 25-hydroxyvitamin D in a population of elderly people with the same ethnic patterns and conditions of latitude and climate. Similarly, Valtueña et al. (16), who studied European adolescents, also found no association between rs1544410 genetic polymorphism and serum 25-hydroxyvitamin D levels. In the light of the foregoing, it appears that ethnic diversity results in different behaviors for this phenotype related to the VDR gene, as previously suggested by Fei et al. (8).
Some factors may influence the low concentrations of 25-hydroxyvitamin D, such as age, race, socioeconomic status, seasons of the year, exposure to sunlight and eating habits (17,18). On the concentration ratio of the vitamin verses polymorphisms of the VDR gene, Jollife et al. (19) published a summary of all genes involved in vitamin D metabolism and demonstrated that the VDR gene is already present in cell signaling when it binds to the active form of the vitamin. Under these conditions, it can be hypothesized that polymorphism of this receptor gene would not influence the concentrations of 25-hydroxyvitamin D, but rather the cellular response.
As for the distribution of genotypes of the rs1544410 polymorphism found in this study, the results differ from those performed with Brazilian adolescents. In this respect, Santos et al. (9) found a higher frequency in BB (47.0 %) and B allele (68 %) in the southern region and Cobayashi et al. (10) found a higher frequency of Bb genotype (63 %) and B allele (59 %) in the northern region. However, a study carried out in the same geographic space but with an elderly population corroborates our findings, with a higher frequency of the bb (38 %) and allele b (55 %) genotype (15). These data point to genotypic differences depending on the regions of Brazil. For the polymorphism rs2228570, the results of the present study corroborate the findings of Cobayshi et al. (10), with a higher prevalence of the F allele.
Vitamin D appears to improve the function of pancreatic β cells, protect them from attack by the immune system, raise insulin receptor sensitivity and, consequently, decrease insulin resistance (3,20). For these functions, the active form of vitamin D must bind to its receptor, so that the expression of the gene could be involved in the pathogenesis of hyperglycemia, hyperinsulinemia and progression of DM2 (8).
In this sense, fasting glycemia values in the present study were shown to be significantly associated with the rs1544410 polymorphism, where the BB genotype presented higher glycemic mean (p = 0.049). Results from a subsample of healthy children studied by Cobayashi et al. (10), reexamined two years later, also showed the influence of rs1544410 polymorphism on fasting glucose concentrations. Luo et al. (21) have shown that individuals with the b allele have a higher VDR expression rate than individuals with the presence of the B allele, indicating that the effect observed in our series may be a consequence of higher expression in adolescents with Bb or bb genotypes (p = 0.01) and Bbxbb (p = 0.03). However, in the BBxBb ratio (p = 0.26), the effect of b is null.
Studies conducted by Shuch et al. (22) carried out in São Paulo, Brazil, in adults with and without metabolic syndrome, associations of rs1544410 polymorphism with insulin resistance and fasting glycemia were not observed. The heterogeneity among the populations studied may explain the divergence of the results regarding genotype and risk allele in this context (23).
In the logistic regression model, glycemia remained related to rs1544410 (p < 0.05) genotypes. It was observed that the adolescents studied who had BB genotype had a 115 % risk of presenting above-median glycemia, and when the genotypes were analyzed together BB+Bb, the risk was 89 %, demonstrating that possibly the presence of the B allele increases the chance of adolescents having higher glycemia. Our data corroborate meta-analyses recently published by Fei et al. (8) with Chinese and Caucasian adults with type 2 diabetes and other diseases such as cardiovascular diseases, and Wang et al. (7) healthy as control subjects and with type 1 and 2 diabetes. In both meta-analyses, the association between VDR and risk of type 2 diabetes mellitus was found for the B allele and BB genotype of the rs1544410 polymorphism. Although robust, these meta-analyses did not include studies with Brazilian populations. Therefore, the present study extends the already established results for this population of the Western South hemisphere.
On the other hand, Bb+bb was protective, with a 34 % lower risk of having glycemia above the median (p = 0.025). Despite the findings described, Oh and Barrett-Connor (24) presented divergent results. These authors evaluated healthy non-diabetic Caucasians and found that carriers of the bs genotype of rs1544410 polymorphism, relative to BB and Bb, had significantly higher levels in insulin resistance markers. It is noteworthy that these markers use fasting glucose as a variable.
Polymorphisms were also analyzed separately for vitamin D status as sufficient and insufficient/deficient, and there was no significant association of rs1544410 genotypes with fasting glycemia and the other biochemical parameters investigated. Issa et al. (15) evaluated variants of the rs1544410 polymorphism, separating by vitamin D status into sufficient and insufficient/deficient groups, and also did not observe association of fasting glycemia between groups.
Although the BB genotype presented higher glycemia, these values do not appear to be of concern because they are still within the normoglycemic limits. However, there is evidence indicating that higher values of several clinical variables in adolescents are already a predisposing factor for the development of a pathological clinical condition in adulthood. An example of these clinical variables is childhood abdominal obesity, which is already reportedly associated as a risk factor for insulin resistance and DM2 in adulthood, as recently emphasized in a study by Alías-Hernández et al. (25). Our results contribute to a better knowledge in this research literature, reinforcing the genetic aspect also as an early marker, as reported by Li et al. (26), who state that the presence of these polymorphisms even in healthy individuals can lead to an increased risk for DM2.
Despite the relationship of rs1544410 polymorphism with glycemia, in the present study, the same did not occur for polymorphism rs2228570. In a meta-analysis, Fei et al. (8) report that the rs2228570 polymorphism is close to the promoter region of the gene and does not only affect vitamin D function, but also disrupts insulin functioning, interfering with plasma glucose levels and leading to DM2. Other meta-analyses indicated that this polymorphism was significantly associated with increased glycemia and risk of DM2, and the f allele and homozygous variant ff may be risk factors for DM2 (7,26). Although studies indicate this association, Yu et al. (27) found no significant relationship between rs2228570 and DM2 in Chinese diabetic and non-diabetic individuals of different ages, sex, and subgroups. These results are similar to those found in the study by Malecki et al. (28), with diabetics and non-diabetics in Poland, where the results did not provide evidence of the relationship between polymorphism rs2228570 and variables related to the glycemic profile. Likewise, Jia et al. (29), in Chinese, and Wehr (30), in women diagnosed with polycystic ovary, also found no association of rs2228570 polymorphisms with endocrine or metabolic patterns. Recently, Bertoccini et al. (31) also found no evidence of the relationship of this polymorphism with glycemic profile.
It was not possible to perform the analyses of other biochemical markers related to the carbohydrates metabolism such as fasting insulin and HOMA for predisposition to insulin resistance. This is the first study in healthy adolescents in northeastern Brazil. The relevance of this study is in the amplification of the VDR gene polymorphisms already found in European and Caucasian populations for the Western hemisphere region. Our data confirmed the relationship of rs1544410, but not of rs2228570, demonstrating that regions and ethnicities seem to be a factor influencing the genotype, particularly for the case of glycemia in adolescents.

