










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Anxiety is an emotion or a negative mood defined by some authors as apprehension and anticipation of the future. In Brazil, 9.3 % of the population suffers from some kind of anxiety disorder. This is three times as much as the world average of 3.6 % (1). On distinct levels, the feelings and symptoms caused by anxiety include increased heart rate, excessive sweating, shaking, impatience, frustration, irritability, lack of concentration, hypervigilance, cognitive distortions, fear, agitation, and difficulty speaking (2-4). When experienced at a moderate level, anxiety can impact learning as well as physical and intellectual performance (5). An anxiety state is categorized as a passing emotional state of the human body characterized by unpleasant feelings of tension and consciously perceived apprehension (6).
In terms of behavior, anxiety is related to a sense of aversion and an urge to run away, avoiding both affection and negative experiences (7). Because of this, many people develop harmful habits such as overeating or illegal drug use for mood regulation. This contributes to the development of addictions (8) that, in addition to decreasing serotonin (the neurotransmitter responsible for good mood), can reduce internal and external stimuli, and induce excessive and inappropriate increases in food intake. That, in turn, changes the composition of the body, which consists of fat and lean mass, as well as water (9,10).
In practice, fat body mass is measured primarily using anthropometric methods with specific equipment and calculations. Body mass index (BMI), waist circumference (WC), waist-to-height ratio (WHR), and body fat percentage (%BF) are the most common indicators used for identifying overweight individuals and high body fat distribution. As an isolated measure, BMI cannot distinguish fat from lean body mass, and does not take into account the amount of water, muscle, and bone mass. Bioimpedance tests can be used to estimate those components by applying electric currents to body compartments (11). In order to diagnose an individual as overweight or as having another disorder, a combination of both indirect methods (anthropometrics and bioimpedance) is recommended due to their practicality, speed, and wide population reach.
In a recent literature review about mood and obesity, anxiety has been considered a risk factor for overweight, regardless of the occurrence of depression. Extreme examples cited include binge eating disorder, with episodes of unusually high food intake over short periods of time observed under elevated levels of anxiety and negative emotional states. In fact, eating disorders had been found in 30 % of obese individuals, according to the study. In another review based on a meta-analysis, an association between anxiety and obesity was found in 16 cross-sectional studies, with an odds ratio of 1.4 (CI: 1.2-1.6), suggesting opportunities for further research on specific obesity severity levels (9,12,13).
While the association between anxiety states and anthropometric indicators does not specifically denote a causal relationship in either direction, the present study aims to verify such association in university students using anxiety as the exposure of interest.
MATERIALS AND METHODS
The target population of the Longitudinal Study on the Nutrition and Health of University Students (NUTSAU) were students attending the second semester of each of the seven undergraduate programmes - Biology, Nursing, Engineering, Pharmacy, Nutrition, Medicine, and Chemistry - on offer at the Federal University of Rio de Janeiro (UFRJ), Macaé Campus. Our focus on second-semester students was based on the fact that the students at this point had had time to become more used to the campus and their study and dietary routines for at least six months (14).
The data were collected during the second semester of 2015 in classrooms and at the laboratory of the Research Centre on Health and Society (NUPESS/UFRJ-Macaé), with the assistance of lecturers and undergraduate research scholars of NUTSAU.
The sample for the study was calculated considering a prevalence of 12 %, a margin of error of 5 %, and a confidence level of 95 %. A sample of 147 students was assessed as part of the project.
The students were trained to assist with questionnaire administration, and the measurements from the anthropometric assessments were standardized to ensure intra- and inter-rater reliability (15). Classrooms were visited three times on average for different modules within each programme in an effort to include as many eligible students as possible.
The questionnaire was designed based on current scientific literature in adult public health (16-19). A draft version was pre-tested on nutrition students, and any terms or words not fully understood were replaced. The final version included questions related to gender, age, housing situation regarding house share, economic class, physical exercise, sedentary lifestyles, smoking habits, drinking habits, and anxiety symptoms.
INCLUSION AND EXCLUSION CRITERIA
Inclusion criteria: second-semester students aged between 17 and 25 years, determined based on habits and routines observed at least six months into their undergraduate studies (14).
Exclusion criteria: pregnant and nursing women, as well as individuals with physical limitations for whom an anthropometric assessment would be impracticable.
Exposure: anxiety symptoms
Anxiety symptoms were assessed using the State-Trait Anxiety Inventory (STAI) scale (6), a self-reported instrument consisting of 20 items in which respondents used one of four ratings (1 = almost never; 2 = sometimes; 3 = often; 4 = almost always) to describe how they felt generally (6,19). Each of these items comprised two parallel scales, one for assessing trait anxiety (STAI-T) and another for state-anxiety (STAI-S). A score of 1-4 was assigned to each answer for quantification and interpretation purposes. For positive questions, the answers were marked in reverse scale ("almost always" scored 1 and "almost never" scored 4). For STAI-S, questions 1, 2, 5, 8, 10, 11, 15, 16, 19 and 20 were positive (6,19).
The scores for each completed questionnaire ranged between 20 and 80. Anxiety values were interpreted dichotomically based on the median value of the scores returned by the analysis of the student-filled questionnaires, as suggested by the relevant literature for use with the STAI anxiety assessment instrument (20-22). As the median was 43 points for both state anxiety and trait anxiety, any anxiety scores equal or greater than 43 points were considered high for both anxiety types in the present study.
OUTCOME: ANTHROPOMETRIC INDICATORS
Body mass (kg) was measured according to Lohman & Martorell (15), using a 50 g precision Tanita Inner Scan® digital scale with a maximum capacity of 150 kg. Each subject dressed in light clothing stood barefoot on the scale's platform. Height was also measured according to Lohman & Martorell (15) using a 1-cm precision Alturaexata® portable stadiometer. The subjects stood upright with their bare feet together, head facing forward in the Frankfurt plane, knees straight, and heels touching the base of the stadiometer. The BMI values were obtained from a calculation of the body mass divided by the height squared (kg/m²), categorized into the ranges used by the World Health Organization for teenagers (< 20 years) and adults (≥ 20 years) (23,24), and classified as either adequate (< 25 kg/m²) or excessive (25 kg/m²).
Waist circumference (WC) was measured with a stretch-resistant tape at the midpoint between the last palpable rib and the anterior superior iliac crest on exhalation, as described by Lohman and Martorell (15). The values obtained were considered adequate measures if < 94 cm or risk factors if ≥ 94 cm for men. The cut-off point for women was 80 cm (21).
Body fat percentage (%BF) was measured for the lower limbs using a Tanita Inner Scan® device with bioelectric impedance analysis (BIA) capabilities. A protocol, which included fasting, no-caffeine, no-alcohol, hydration, and exercise policies, was adopted as preparation for the physical assessment (25). Body fat percentages were categorized using the Lohman and Martorell procedures (15) for statistical analysis, with values < 15 % in the ‘adequate' range, and ≥ 15 % in the ‘high' range for males. For females, body fat values < 23 % were considered adequate, and values ≥ 23 % were considered high.
The impedance and anthropometric assessments were conducted in the morning, and the questionnaires were administered in the afternoon.
DATA PROCESSING AND ANALYSIS
The statistical analysis was run on SPSS v. 21 software, and Epi-Info with double data entry was used for processing. Frequency and prevalence data were presented for categorical variables, and a comparison was run between groups using chi-squared tests.
The association between exposure (state anxiety), via the median, and the outcome (anthropometric indicators), whether at adequate or inadequate levels, was determined with a logistic binary regression analysis to estimate crude and adjusted odds ratios (OR) for each indicator.
The state anxiety variable was dichotomized and characterized as < median (43 points) and median (43 points). This value refers to the group median according to the authors who use the instrument and follow this premise (23-25) based on the fact that the STAI instrument cannot diagnose the level of anxiety, but it can identify it. The anthropometric indicators were dichotomized as follows: BMI and %BF were considered either adequate or excessive; WC and WHR were considered either adequate or increased risk. Adequate BMI, WC, %BF, and WHR were used as the reference category for the indicators.
The adjusted model for BMI was composed of the following variables: gender, walking time per day, and alcohol consumption, the confounders that influence the association under study the most. For the remaining indicators, WC, %BF, and WHR were adjusted by age, walking time/day, energy, and alcohol consumption. The significance level used for the test was ≤ 0.05.
ETHICAL ASPECTS
The NUTSAU project was authorized by the campus general director of the Federal University of Rio de Janeiro at Macaé, and meets the criteria outlined in resolution 466 of December 12th, 2012 by the National Health Council, submitted and approved by the Research Ethics Committee of the Federal University of Rio de Janeiro, Macaé Campus (CAAE 51104115.4.0000.5699). All of the students were informed of the purposes of the study as appropriate, and asked to sign a free informed consent form.
RESULTS
A profile analysis of the 147 university students found that 63.3 % of the subjects were female and approximately two-thirds of the total of these undergraduates were studying health-related programs. Self-reported responses established that 53 % of the students self-identified as white, and 91.8 % were not recipients of student financial help or bursaries of any kind (housing, undergraduate research grants, community extension and outreach services, or mentoring scholarships). Screen usage time indicators also showed that 89 % of the students used screens for more than two hours a day, and significantly more women (94.6 %) engaged in high levels of usage than men (74.6 %) (p = 0.01) (Table I).
Table I. Student distribution according to socioeconomic, demographic, and anxiety state characteristics. Rio de Janeiro, 2020
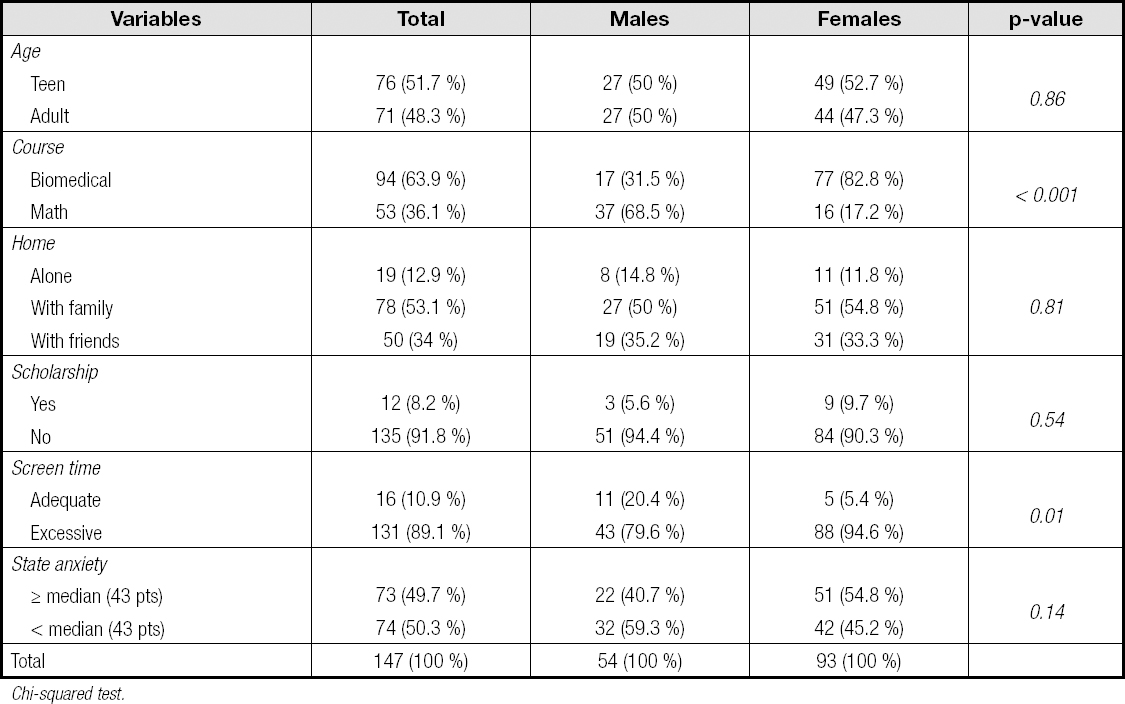
Chi-squared test.
Anthropometric assessments placed nearly one fourth (23.8 %) of the students in weight categories that put them at increased health risk based on their BMI, with 16.3 % of overweight and 7.5 % of obese students. The results for WC measurements showed high and very high risk in 8.2 % of the subjects, with women accounting for a larger portion of this risk group (p = 0.06). Increased risk levels of WHR were also found in 10.9 % of the students, and 22.4 % of the %BF content measures found were either bad or critical (Table II).
Table II. Student distribution according to anthropometric variations and gender. Rio de Janeiro, 2020

Chi-squared test.
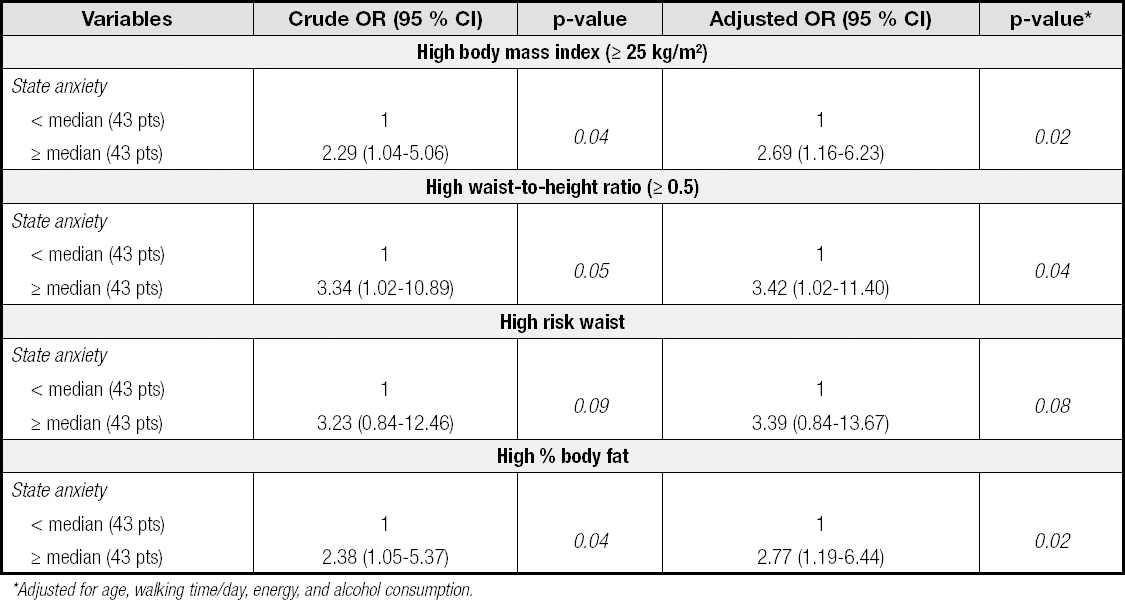
Among the students with anxiety states above average, the adjusted analysis models found a 2.69 OR for overweight (p = 0.02) and 2.77 OR for bad or critical %BF (p = 0.02) (Table III).
DISCUSSION
This study was developed with university students who faced numerous challenges and responsibilities after starting their degree programmes. They suffered from the expectations placed on them by their families and society at large, and had to deal with dramatic changes in their daily lives due to exhaustively long hours of lectures and studies. All of these factors, which were directly or indirectly linked to the analyzed individuals, may increase the risk of developing or worsening anxiety symptoms, which has reflections on anthropometric indicators in the short term, and poses a potential risk for chronic non-communicable diseases in the long term.
The sample of students was predominantly made up of female subjects, and a majority attended health-related programs. Scholarly literature has shown that such full-time programs with heavier workloads, compounded by internal and external pressures, affect health, which means these students are more prone to showing signs and symptoms related to anxiety (26).
Approximately half of the students did not live with their families - they either shared accommodation with friends or lived alone. Additionally, the fact that only 8.2 % received some kind of financial support in the form of bursaries or scholarships suggests that 91.8 % of these undergraduates were financially dependent or had to work for a living, which may have significantly impacted their quality of life during their education period (27).
One of the lifestyle indicators assessed in the students was the use of electronic devices, specified as screen time. Prolonged use of screen devices was the prevailing trend in the sample, with a predominance of female students exhibiting this behaviour (p = 0.01). Following controls for potential confounding data (gender, income, body mass, and a variety of behaviours related to diets and physical exercise), two studies (28,29) found that such factors can contribute to a deterioration of anxiety symptoms and, as a result, may adversely affect anthropometric indicators.
A large proportion of the students assessed in the present study were found to be in the overweight category according to BMI indicators. Such findings were in line with the data obtained by the Surveillance System of Risk and Protective Factors for Chronic Diseases by Telephone (VIGITEL) survey, which revealed that one third of the young adult population are overweight (15). International studies have suggested that the increasingly high BMI values found in young adults could be a consequence of their lifestyles (30).
However, as much as the BMI analysis provides an important assessment tool, it cannot alone distinguish between lean and fat mass, nor can it provide insight regarding their distribution (11). For this reason, BMI assessment was used in combination with other important indexes for fat estimation, such as WC and WHR, due to their ability to provide a simple and valid diagnosis of abdominal adiposity, and major indicators of risk factors for heart diseases, for example (31). The use of WC measurements enabled us to identify that 8.2 % of the sample was at a high or very high health risk, and most of these individuals were female. Campagnoli (32) reports a similar trend, pointing out an association between gender and greater proneness to obesity due to a number of factors including the presence of estrogen (a hormone that predisposes an individual to the formation of fat tissue in the body), a low calorie burn rate, and a greater tendency to consume more palatable food. A high WHR was found in 10.9 % of the students, which is associated with the high values found for WC, and suggests that young adults have unhealthy lifestyle and dietary habits.
The %BF results provided useful insight into fat and lean mass discrepancies, and were fairly simple to determine using a variety of approaches (33). Our study found worrying numbers related to this metric, with 22.4 % of the subjects in the bad or critical range of %BF. Considering that 24.7 % of the women involved were in this range (compared to 18,5 % of the men), the findings seem to confirm that men and women have different body compositions, possibly due to hormonal and physiological differences (32).
Most importantly, our study found a significant association between the highest levels of anxiety and anthropometric indicators for BMI and %BF. Such findings contribute to the results of the systematic reviews followed by meta-analyses (34), and corroborate a recent review (9) that linked the mechanisms of anxiety and obesity with the secretion of hormones such as serotonin. Additionally, individuals with higher levels of anxiety frequently avoided situations that could abruptly change their physiological responses, such as increased heart rate and blood pressure, contributing to a reduction in physical exercise (35). The combination of hormonal and physiological factors can lead to greater consumption of palatable food due to the neuronal stimulation and dependence it can induce. High-fat and high-sugar diets can cause inflammatory and cognitive changes (due to inflammation of the hippocampus, a critical region responsible for memory), leading to obesity (36).
In relation to the present study, it is important to highlight the particularities of the data collection location, which, when compared to other educational institutions, imposes limits on the sample size. The Macaé campus of the Federal University of Rio de Janeiro (UFRJ-Macaé) was inaugurated in July 2008, based on the recognition and evolution of the academic community, with the objective of creating courses, projects, and research in Macaé, a municipality in the state of Rio de Janeiro. In 2011, the campus offered eleven different courses within two different areas: exact sciences (chemistry, engineering, and pharmacy) and biological sciences (nutrition, chemistry, nursing, medicine, and biology). In 2015 the data collection of the NUTSAU group took place on this campus, covering all courses and the whole universe of university students present there.
One of the limitations related to the study, in addition to the number of individuals enrolled, is its cross-sectional design, which defined the scope of the inference. In addition, these characteristics also limit the analysis options with more stratification ranges. Because of this, it was then decided to work with the median, aiming at more homogeneous and comparable groups, in addition to careful work with the use of OR for anxiety symptoms and avoidance of closed diagnoses.
As the main potential for contribution by our study, our findings could be used to inform professional healthcare practice by providing evidence on the importance of intervention models that combine both the psychological and nutritional perspectives in order to promote innovative strategies in the prevention and treatment of anxiety and obesity.
CONCLUSION
Self-reported anxiety information in association with anthropometric assessments has allowed us to identify anthropometric risk for individuals with above-median anxiety states, showing an association between higher anxiety levels and anthropometric indicators for overweight or obesity, and high or very high body fat percentages.

