










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The human taste system can recognize five basic tastes: sweet, sour, bitter, salty and umami. Gustatory function affects nutrition, food choice, pleasure and sensory aspects of food, metabolic efficiency, and even quality of life. According to the National Health and Nutrition Examination Survey, the estimated prevalence of taste impairment was 17.3 % (1). Patients who complain of dysgeusia may actually have olfactory dysfunction. In the previous study 8.7 % of patients reported taste loss, but less than 5 % of patients actually had taste dysfunction according to taste testing. Self-reported gustatory function was not reliably related to psychophysical test results (2). Therefore, it is necessary to carry out a quantitative and qualitative assessment of the gustatory function.
In Asia, Japan was the first country to use the whole-mouth gustatory test to study the gustatory function of Japanese subjects, followed by China, South Korea, and Taiwan (3-6). Hwang CS et al. (4) tested five basic tastes, including sour, sweet, salty, umami, and bitter in 2018, and obtained the normal range for a Korean population. Umami, one of the five basic tastes, was widely present in food. Umami can reduce the use of salt in food processing and increase the flavor of food, which plays a very important role in maintaining health (7,8). In order to fully evaluate the taste function, it is necessary to conduct a functional evaluation of the five basic tastes including umami. In 2010, Yang et al. (6) studied the gustatory function of Chinese subjects with the three-drop method, but the sample size of the study was small and they considered only four basic tastes (bitter, sweet, salty, and sour), without umami. Therefore, the aim of the study was to develop a convenient, fast and reliable tool to assess the taste function with the five basic tastes in healthy Chinese adults.
MATERIALS AND METHODS
STUDY SUBJECTS
Healthy subjects were recruited for physical examination at the health examination center of our hospital from January, 2021 to April, 2021. All subjects had signed a written informed consent. This study had been approved by the Ethics Committee of our hospital (No.: 2021074X). Inclusion criteria were healthy adults aged 18 to 65 years with normal self-rated smell function and gustatory function. Exclusion criteria were subjects with olfactory dysfunction, gustatory dysfunction, acute oral infections, acute otitis media, coma after head trauma, mental illness, neurodegenerative diseases, or previous middle ear surgery, nasal surgery, radiotherapy or chemotherapy. Detailed data about each person's current health status, past history, and chemosensory function were obtained through a questionnaire. Otolaryngological examination excluded subjects with acute otitis media and/or acute pharyngitis.
PROCEDURE
In the assessment of gustatory function with the whole-mouth taste test, five liquid taste solutions were used. Five basic tastant solutions (sour, sweet, salty, umami, and bitter) were respectively prepared with citric acid, sucrose, sodium chloride, monosodium glutamate, and quinine hydrochloride in distilled water. Successive test concentrations were determined based on the study by Hwang CS et al. (4) and preliminary experiments. In order to ensure that the lowest concentration of each taste test was suitable for the Chinese population, we reduced a concentration gradient based on the testing by Hwang CS. Through preliminary experiments, the concentration was adjusted appropriately and finally 7 concentrations (No. 1 to No. 7) were prepared for each solution. The No. 1 dilution concentration was the lowest concentration and the No. 7 dilution concentration was the highest concentration (Table I). Taste solutions were prepared once a week.
Table I. Concentrations of taste stimuli used in g/mL (solvent: distilled water)
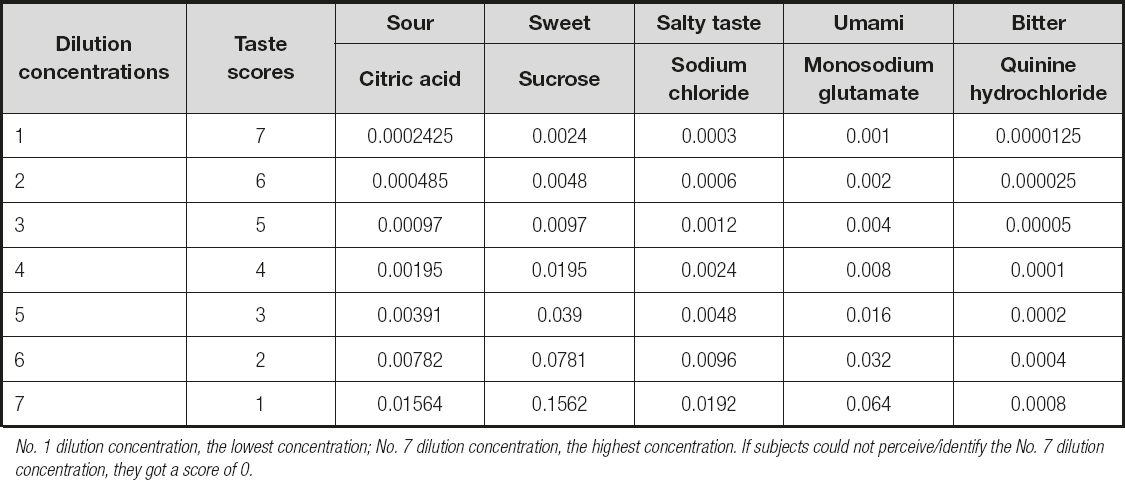
No. 1 dilution concentration, the lowest concentration; No. 7 dilution concentration, the highest concentration. If subjects could not perceive/identify the No. 7 dilution concentration, they got a score of 0.
Tastant solutions were administered via a disposable plastic dropper with a standard scale. A drop (0.1 mL) of each tastant solution was dripped in the middle of the anterior third of the extended tongue of each subject. Then subjects swished the drop in their closed mouth. After administration of each solution, subjects were asked to rinse their mouths with tap water. Administration was started with the lowest concentration until the individual tastant was detected. We then re-tested the concentrations that were one level lower and higher in order to confirm the exact threshold concentration. The lowest concentration at which the subject perceived a sensation of taste was defined as the detection threshold. In the course of determining the taste recognition threshold, the subjects were asked to choose one of five tastes to describe the administered taste (salty, sweet, sour, bitter, and umami). The administration concentration gradually increased until the correct recognition of the respective tastant concentration occurred twice. The lowest concentration of the identified tastant solution was defined as the recognition threshold. The administration was carried out in a pseudo-randomized order. Five basic tastes were respectively tested and the bitter was tested at last. The recognition score was obtained based on the recognition threshold. According to the concentration corresponding to the identified taste, the subject got a score between 0 and 7 for each administration. If subjects did not identify the taste at the No. 7 dilution concentration, they received a score of 0. The higher the threshold was, the lower the score was. In order to obtain an overall evaluation of gustatory function, recognition scores of all the five tastants were summed as total scores ranging from 0 to 35. The complete procedure for the five tastes was completed within almost 20 min. The inspection was conducted in the morning (8:30-11:30 am). Subjects were instructed not to eat or drink anything except water, brush their teeth or smoke at least one hour before the test.
TEST RELIABILITY
To verify test-retest reliability, the taste test was repeated in 50 subjects (24 men and 26 women with a mean age of 40 years and an age range of 20 to 63 years) 2 weeks later.
STATISTICAL ANALYSIS
The statistical analysis was performed in SPSS 22.0 (SPSS Inc., Chicago, IL, USA). Student's t-test or analysis of variance for repeated measures (rm-ANOVA) was performed to assess the statistical significance of the differences between subgroup scores. Bonferroni tests were performed for post-hoc comparison. Pearson's correlation coefficient was used to assess the correlation. The intraclass correlation coefficient was used to assess reproducibility and internal consistency. A χ2 test was used to assess composition ratio. A p-value ≤ 0.05 was considered to be significant.
RESULTS
A total of 464 participants underwent the taste test (227 females and 237 males, age range 19-65 years). Descriptive statistics are provided in table II. Normative values are presented according to different age groups and sex in table III. To assess gustatory function, the perception and recognition thresholds of sour, sweet, salty, umami, and bitter taste were analyzed separately. The total taste scores of recognition showed a significantly negative correlation with age (r = -0.279, p < 0.001). The perception threshold and recognition threshold of the individual five tastants except the salty taste also demonstrated a significant correlation with age (-0.356 < r < -0.110, p < 0.05). Total scores decreased with increasing age and showed significant differences (p < 0.001) between the three age groups (younger group: 19-35 years, middle aged group: 36-50 years, and older group: 51-65 years). Older subjects (51-65 years) had the lowest scores. Individual tastants' perception threshold and recognition threshold showed no significant differences between the younger-age group and middle-age group (p > 0.05). For the sour, sweet, umami, and bitter tastes, the perception scores of the older group were significantly lower than those of the younger group and middle-aged group. For the sour, umami, and bitter tastes, the recognition scores of the elder group were significantly lower than those of the younger group and middle-aged group.
Table II. Descriptive statistics of taste scores for all subjects
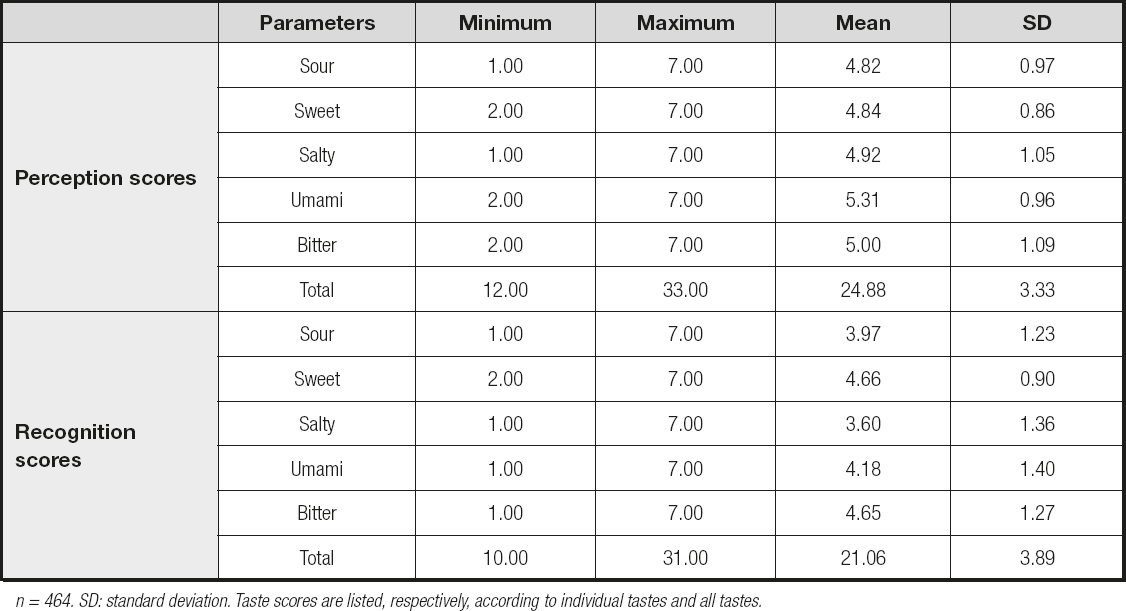
n = 464. SD: standard deviation. Taste scores are listed, respectively, according to individual tastes and all tastes.
Table III. Recognition scores from taste testing in the various participant groups of sex and age
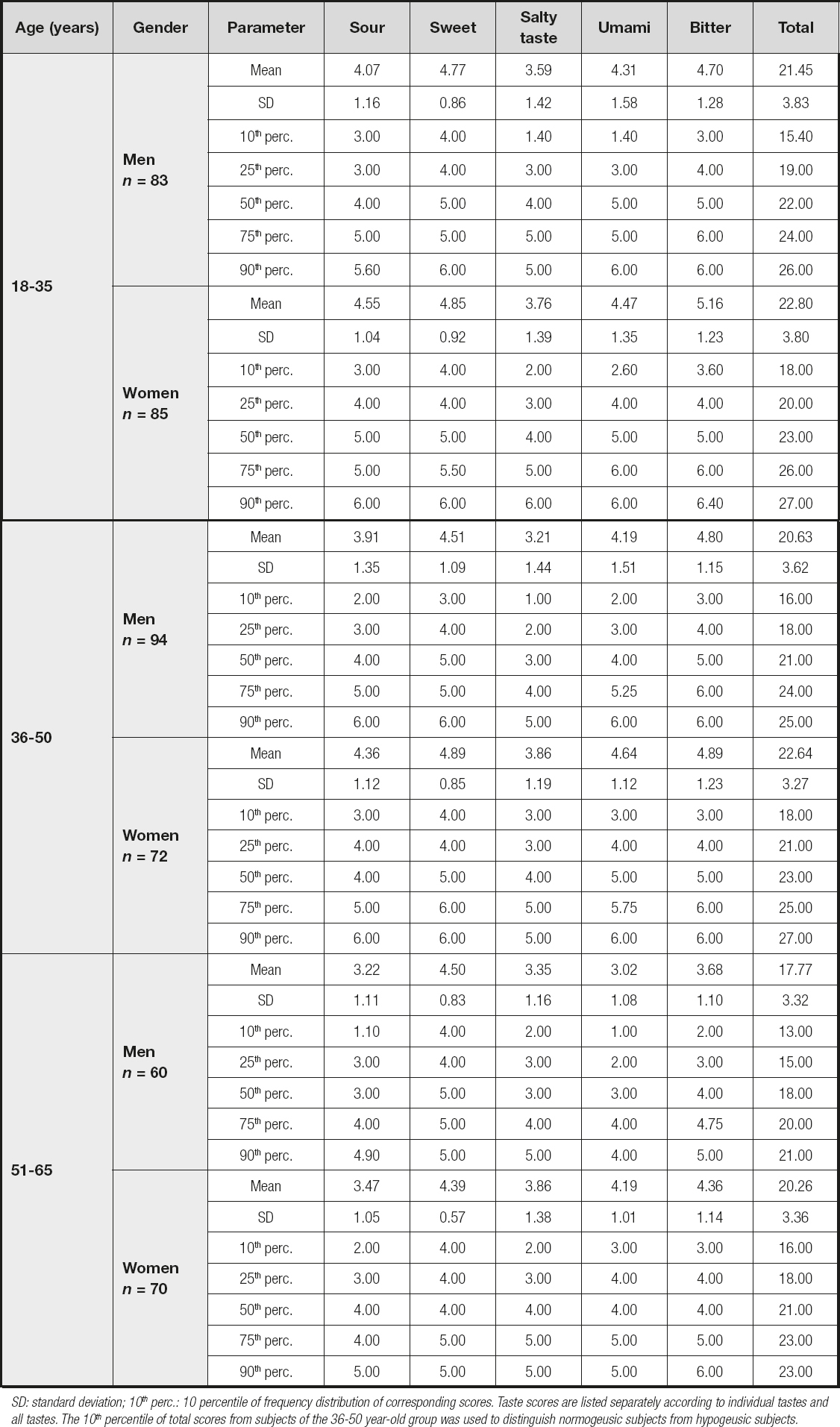
SD: standard deviation; 10th perc.: 10 percentile of frequency distribution of corresponding scores. Taste scores are listed separately according to individual tastes and all tastes. The 10th percentile of total scores from subjects of the 36-50 year-old group was used to distinguish normogeusic subjects from hypogeusic subjects.
Total score of recognition for women were higher than those for men (p < 0.001). In a further exploratory analysis of perception scores, the effect of gender was most significant for sour (p = 0.024), salty (p = 0.044), umami (p = 0.046) and bitter (p < 0.001), but it was not significant for the sweet taste (p = 0.804). The same results were found in the taste recognition thresholds between men and women (sour, p = 0.001; salty, p < 0.001; umami, p < 0.001; bitter, p < 0.001; sweet, p = 0.154).
Based on the definition of hypogeusia, the 10th percentile for subjects aged 36-50 was used to differentiate normogeusic subjects from hypogeusic subjects (4,9). Therefore, the subjects with total score of recognition lower than 16 for males and 18 for females were considered hypogeusic subjects in this study.
Subjects were divided into a non-smoking group (giving up smoking or smoking < 100 cigarettes) and a smoking group. The total taste score of recognition for non-smokers was significantly higher than that for smokers (21.23 ± 3.91 vs. 19.90 ± 3.52, p = 0.014). In a further exploratory analysis of recognition thresholds, the effect of smoking on salty was the most significant (p = 0.013), but the effect of smoking was not significant on sour (p = 0.082), sweet (p = 0.459), umami (p = 0.444), and bitter (p = 0.056). Individual tastants' perception threshold showed no statistically significant differences between smokers and non-smokers (p > 0.05). The proportion of smokers showed no signficant difference among the three age groups (45 smokers and 123 non-smokers in the younger group; 34 smokers and 132 non-smokers in the middle-aged group; 32 smokers and 98 non-smokers in the older group; χ2 test, p = 0.392). Smokers were mostly males (smokers included 57 males and 2 females; non-smokers included 180 males and 225 females; χ2 test, p < 0.001).
The intraclass correlation coefficients of taste perception scores and taste recognition scores for the five tastants were 0.774 to 0.833. The study method showed a relatively high reliability.
DISCUSSION
In this study, the gustatory function of Chinese people was tested with the whole-mouth taste method to obtain normative data for the sour, sweet, salty, umami, and bitter tastes.
At present, subjective gustatory function tests mainly include chemical threshold tests and electrical threshold tests. The subjective gustatory function test is a psychophysical test and can quantify the subject's conscious perception of taste stimuli (10). Chemical threshold tests mainly include the whole-mouth taste test and regional taste test (4,10). A cotton swab or filter paper dipped in the tastant solution can be used to evaluate the regional taste function. The regional taste test can be used to determine whether a given taste nerve is dysfunctional (11). The whole-mouth taste test can be performed in cups or small containers, or with droppers of different sizes (9). The whole-mouth test is usually employed to explore the overall gustatory function. Because of its economy, fast speed, and convenience the whole-mouth taste test is the dominant subjective taste test at present. The liquid-drop method and the three-drop method are the most commonly used whole-mouth taste tests. An adequate evaluation of taste function is essential in the diagnosis of chemosensory dysfunction.
Umami has been shown to be the fifth basic taste, and is the reason why human beings can enjoy delicious foods. Japanese scholar Kikunae Ikeda isolated glutamate from kelp for the first time in 1908. It was only in the 1980s that umami was recognized as a basic taste, mainly the taste of sodium glutamate (MSG) (12). Umami can produce a "salty" feeling (7). Adding MSG to foods can reduce the use of salt during food processing, improve the quality of life of the elderly, and partially replace the use of salt in patients with anorexia. The evaluation of the taste sensitivity for umami before adding MSG to foods can also improve the compliance of patients with anorexia (13). In the study, we found that the recognition score of umami gradually decreased with age. According to the study of Satoh-Kuriwada, some patients, especially the elderly, complained that the subjective sensation of umami was continuously impaired, even though the other four basic taste sensations were still normal (8). This unknown impact on umami will be explored in the future.
In the process of clinical testing, many factors affect the subjective taste threshold, including water temperature, saliva volume (14), number of taste buds (15), time interval for each taste stimulation, volume of taste solvent, and duration of stimulation (16). Therefore, in order to control the influencing factors that affect the subjective taste function as much as possible, during the whole test process, the taste solution was placed at room temperature before the actual test. The test was performed by the same examiner in the morning. The taste solution was dripped in the middle of the anterior third of the tongue using a dropper with a standard scale. In order to evaluate the credibility of the whole-mouth test, we analyzed the test-retest reliability of the taste perception scores and recognition scores of sour, sweet, salty, umami, and bitter tastes. In previous studies (4,17,18), the test-retest reliability of the whole-mouth method was analyzed and the ICC value was 0.61 to 0.78. In our study, the taste test showed a high test-retest reliability with an ICC value of 0.774 to 0.833. Therefore, we believed that the taste test was a reliable subjective taste test for Chinese people.
Tastes function are affected by many factors. Aging appears to be the most significant determinant of taste change (19). In epidemiological surveys (20), the incidence of self-reported taste disorders was 19 %, increased gradually with age, and peaked in the elderly aged 80 and older. The incidence of severe gustatory dysfunction was found to be 14.8 % in the adults aged 57 to 85 (21). Clinical studies on taste also confirmed the decline of taste function in the elderly (19,22). In this study, we found that the total taste score of recognition was significantly negatively correlated with age. The taste perception threshold or recognition threshold showed no statistical differences between the younger group and the middle aged group, indicating that the taste function was relatively stable in younger and middle-aged Chinese. However, taste scores declined in those aged above 50, as manifested by a decline in taste perception and recognition ability for sweet, umami, sour, and bitter. According to the result, the 10th percentile of subjects aged 36 to 50 was used to distinguish normogeusic subjects from hypogeusic subjects. Taste disorders in older adults are thought to be related to aging, disease status (especially Alzheimer's disease), medication, surgical interventions, and environmental exposures (23,24). However, the underlying mechanism is not clear. It is speculated that the reduction of gustatory function with aging may be ascribed to a degradation of gustatory peripheral tissues and related to various neural signatures in the central nervous system. The five basic tastes have different receptor cells, so the decline in overall gustatory function might be non-homogeneous (25).
It is generally believed that women's taste sensitivity is better than men's (22,25,26). Our study found that the recognition scores of sour, salty, umami, and bitter, except sweet, in females are higher than those of males. Yamauchi et al. (27) and Yoshinaka et al. (26) reported the same results. According to the study by Heft (28), women were less sensitive to the sour taste than men, but there was no gender difference for the salty taste. A large number of studies suggested that sex differences in taste recognition might be related to differences in sex hormones (29,30). Our study found that smoking led to a decline in taste recognition and mainly affected the recognition of salty. Male smokers were much more numerous than female smokers. It was speculated that the gustatory difference between men and women might be related to living habits, such as smoking (31). In addition, females had more fungiform papillae and taste buds than males, and their gustatory function was superior to that of males (32).
However, in the study we only studied the gustatory function of adults aged 19 to 65, and only considered the influences of age, gender and smoking on taste. In the future, we will add elderly people over 65 years of age and analyze other possible influencing factors on gustatory function.
CONCLUSION
This whole-mouth method is simple and time-saving, and can be easily adjusted to obtain reliable data. The taste function was negatively related to age. In the elderly above 50 years old, taste function was significantly reduced. Taste function was more sensitive in female and non-smokers. Most importantly, this study provided the normative data for the gustatory function of the Chinese.

