










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Rare diseases are serious and uncommon conditions which are defined in the European Union as life-threatening or chronically debilitating conditions with a prevalence of no more than 5 in 10,000 people and with no or limited choice of therapeutic options, and consequently present with an important level of unmet need1. It is estimated that there are more than 6,000 rare diseases affecting around 30 million Europeans2. Orphan Drugs (ODs) are those intended to diagnose, prevent or treat rare diseases3. Some ODs are intended to treat an even smaller part of the population, these are defined as ultra-orphan drugs, which affect < 1/50,000 people4. ODs have been identified as a priority area at European level with the implementation of the European Union regulation EC 141/2000 which introduced regulatory and economic incentives to ODs developers5.
The increasing number of designated ODs has resulted in a growing debate on the complex dynamics of several conflicting factors: promoting timely and equitable access for patients, cost containment strategies to sustain public health services, and rewarding innovation. Public participation, further exploitation of early dialogs and innovative reimbursement approaches, adaptive agreements, multiple criteria to support analysis for price and reimbursement (P&R) decisions and, in general, greater process transparency are among the suggested strategies6.
While orphan designation and marketing authorisation occurs at European level, access to ODs remains a member state responsibility6. This results in differences between countries regarding evidence requirements, drug evaluation, public reimbursement and even in conditions of use and indication restrictions7, and therefore, patient access to orphan drugs varies largely across Europe8,9.
ODs face added challenges when subjected to Health Technology Assessment country appraisals10, as the limited outcomes knowledge and heterogeneity of the diseases make it difficult to demonstrate added clinical benefit, often struggling to recruit a sufficient number of patients for clinical trials or having difficulties in setting up studies comparing the OD with a relevant treatment alternative11, therefore, reducing the level of confidence on the resulting evidence12.
Rare Diseases are also a public health issue in Spain, with about 3 million of patients3 on a population of about 46 million. The relevant number of subjects needing therapies raises the importance of P&R decisions of ODs. Even though reimbursement criteria are defined in the Spanish legislation13, their application in practice is not followed and evaluations and decisions are neither transparent nor explicit, making it difficult to assess P&R outcomes.
This paper aims to shed some light on understanding which disease and outcomes-based P&R criteria were considered by health authorities to approve ODs in Spain between January 2012 and June 2018.
Methods
Price and reimbursement process in Spain
Following European Commission (EC) approval, national marketing authorisation is granted by the Spanish Medicines Agency (AEMPS). Since May 201314, the P&R process in Spain starts with the generation of the Therapeutic Positioning Report (TPR)15, issued by the AEMPS, to establish a recommendation of clinical and value positioning to the General Pharmacy Directorate within the Ministry of Health. The General Pharmacy Directorate releases a proposal to the Interministerial Pricing Commission16, which decides the P&R of the new drug.
Spanish reimbursement evaluation criteria of ODs are the same as for any other innovative drug and are defined by law in the Royal Decree 1/2015 of 24 July17: severity of the disease, unmet needs of specific populations, therapeutic and social drug value, incremental clinical benefit considering cost-effectiveness, budget impact, existence of alternative treatment options for the indication and degree of innovation. The P&R decision must be taken in a time between 180 to 270 days18.
Identification of European Commission approved orphan drugs between January 2012 and June 2018
Drugs approved during the study period were extracted from European Medicines Agency’s website19 through their online medicine finder engine, with the following search filters: human medicines, orphan medicines, only authorised medicines and a time filter from year 2012 to June 2018. Found ODs were grouped according to their EC authorisation year. Extracted information was checked with the EC register of orphan medicines20. Only ODs that had been authorised by the AEMPS to be marketed in Spain, and were therefore able to request P&R, were included in this study. Marketing authorisation status was searched in the AEMPS website21.
Identification of the orphan drugs price and reimbursement situation in Spain
ODs were classified according to their P&R status in Spain using the following definitions: (i) P&R approval (ODs that have received P&R approval); (ii) under P&R decision process (ODs for which P&R has been requested but are still undergoing P&R negotiations), and (iii) P&R rejected (ODs that have seen their P&R request rejected in Spain).
As there is no official information source to know P&R status of medicines in Spain, the following decision tree was created to classify ODs (Figure 1).
The EC approval, the Spanish marketing authorisation and the P&R approval dates were searched for all studied ODs in July 2018 and used to analyse the time from EC approval to Spanish marketing authorisation and the time from Spanish marketing authorisation to P&R approval. EC approval dates were searched in the European Medicines Agency’s website19, the Spanish marketing authorisation dates were searched in the Spanish Online Medicines Information Centre webpage21 and the Spanish P&R approval date was searched in Botplus, a Spanish online payment platform created by the General Council of Official Pharmacy Colleges22. When the date was not available, the OD inclusion date in the list of medicines affected by the economic deductions was used as a proxy of the reimbursement approval date, found in the Spanish Ministry of Health website23. The inclusion date of ODs in the list of medicines affected by the economic deductions was only available if the OD had been approved in the last year, as only documents from the last 12 months are available online. All regulatory time-lines were calculated in months.

Figure 1. Categorisation of studied orphan drugs according to hypotheses used to relate key drivers and price and reimbursement status in Spain.*We assume that all ODs with a published TPR or a TPR in process had finished or were undergoing the reimbursement process.**The TPR publication started in May 2013, so some of the studied ODs could have been reimbursed prior May 2013 without the publication of a TPR.***It was not possible to know if an OD had its P&R request rejected before May 2013 (the year that the TPR publication in Spain started), so the ODs with no published TPR and not included in the list of economic deductions published in the Spanish Ministry of Health webpage were classified as undergoing the reimbursement process.****It is assumed that all reimbursed ODs are commercialised in Spain. MoH: Ministry of Health; ODs: Orphan Drugs; P&R: Price and Reimbursement; TPR: Therapeutic Positioning Report.
Identification, description and stratification of outcome variables for orphan drugs
Thanks to the personal experience of authors (Xavier Badia and Alicia Gil) in P&R negotiations, official published criteria were operationalized to formulate a possible set of outcome variables driving P&R decisions in current practice in Spain.
Studied variables that could drive P&R decisions in Spain are shown in Table 1.
Table 1. Identified outcome variables hypothetically driving price and reimbursement of studied orphan drugs in Spain
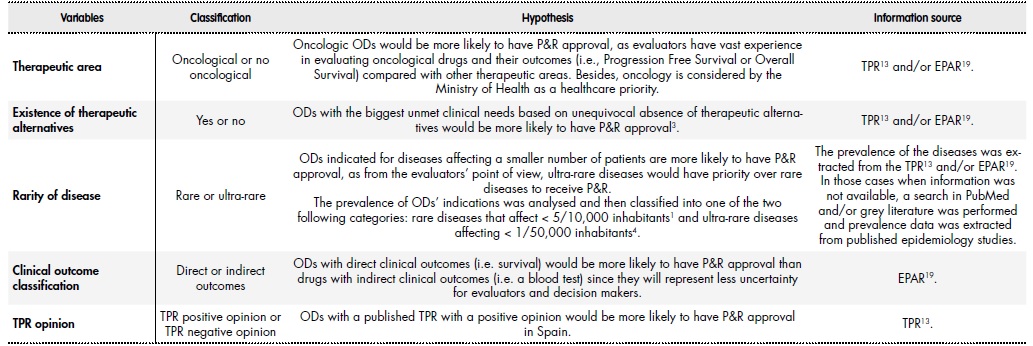
EPAR: European Public Assessment ReportODs: Orphan DrugsP&R: Price and ReimbursementTPR: Therapeutic Positioning Report.
Selected variables were linked to official P&R criteria established by Royal Decree Law 1/2015 of 24 July13 in the following manner: disease severity was related to an oncologic versus non oncologic indication and to the availability of direct clinical trial outcomes, as drugs indicated for severe diseases would be more likely to have P&R approval if they had direct clinical outcomes (e.g.: overall survival); unmet needs of certain collectives was related to being indicated for ultra-orphan diseases; existence of alternative therapies was related to ODs without a therapeutic alternative for the approved indication and degree of innovation was related to ODs with a published TPR with a positive opinion, meaning that the drug offers an added therapeutic value.
Analysis of the impact of outcome variables on price and reimbursement approval
A descriptive and statistical analysis of the outcome variables was conducted to test the validity of the proposed hypothesis shown in Table 2 and to identify potential variables that may positively influence P&R approval of ODs in Spain. Stata software was used.
First, a univariate probit regression was used to analyse the relationship between P&R and each of the outcome variables used. After this, a multivariate probit regression analysis was performed to predict the impact of the studied variables on P&R decision. The probability of P&R approval was considered as the dependent variable. ODs that had undergoing P&R process were excluded from the analysis. Therefore, only final decisions “P&R approval” and “P&R rejection” were considered. The variables considered for the regression analysis were TPR opinion, rarity of the disease, clinical outcome classification, therapeutic area and existence of therapeutic alternatives.
Table 2. Identified outcome variables used in the multivariate regression analysis for each orphan drug approved by the European Commission, with Spanish marketing authorisation and stratified by price and reimbursement status (period 2012-2018)

P&R: Price and Reimbursement; TPR: Therapeutic Positioning Report.
Results
Identification of European Commission approved orphan drugs and price and reimbursement status between January 2012 and June 2018
A total of 78 ODs were found to be approved by the EC between January 2012 and June 2018, of which 64 (82%) had been authorised in Spain. Only ODs for which Spanish marketing authorisation had been approved were selected for the study.
The mean time from EC approval to reimbursement approval for ODs in Spain was 22.5 ± 14.7 months, and the mean time from Spanish marketing authorisation to reimbursement approval was 12.1 ± 5.1 months, with a minimum of 5 months (for two ODs: Darzalex® and Imnovid®) and a maximum of 24 months (Kalydeco®).
Regulatory timelines for P&R approval of ODs have decreased over the last six years and a half: time from EC approval to Spanish marketing authorisation decreased clearly from 2012 to 2018 (20.6 ± 17.3 months vs 1.25 ± 0.5 months, respectively), and time from Spanish marketing authorisation to P&R approval decreased from 2012 (20.5 ± 0.7 months) to recent years: 12,8 ± 5.5 months in 2016 and 11.6 ± 2.8 months in 2017, indicating that the reimbursement process in Spain has shortened up, on average, in 8.9 months since 2012 to 2017.
Identification and description of outcome variables for orphan drugs price and reimbursement
From the 64 studied ODs, 28 (43.8%) had received P&R approval in Spain, 23 (35.9%) were undergoing the P&R decision process and 13 (20.3%) had seen their P&R request rejected.
Out of the 64 ODs, 26 (46%) were oncologic, of which 13 (50%) had P&R approval and 4 (15%) had P&R rejected. From the 23 ODs without an existing therapeutic alternative, 9 (39.1%) had P&R approval and 6 (26%) had their P&R request rejected. From the 27 (42.1%) ODs indicated for ultra-rare diseases, 11 (41%) had P&R approval and 4 (15%) had their P&R request rejected; and from the 33 ODs with direct clinical outcomes, 17 (51.5%) had P&R approval and 5 (15.1%) had their P&R request rejected. Results showed that there were 13 ODs with an ultra-rare indication and direct clinical trial outcomes and of which 6 had P&R approval and 2 had the P&R rejected.
There were 30 ODs with published TPRs with positive opinions, of which 23 (76.6%) had P&R approval. In contrast, all 4 (100%) ODs with a negative TPR had P&R rejected.
A total of 23 observations were excluded from the regression analysis because P&R negotiations were still undergoing, thus no final decision on P&R was available. The final dataset was formed by a total of 41 ODs. TPR opinion (introduced as “tpr_op” in the regression analysis), rarity of the disease (introduced as “rarity”), clinical outcome classification (introduced as “outcome”), therapeutic area (introduced as “therapeutic” in the regression) and the existence of a therapeutic alternative (introduced as “alternative”) were the variables considered in the regression analysis.
P&R variables used in the regression analysis, stratified by P&R status are described in Table 2.
When the univariate probit regression analysis was run, TPR opinion was found to be related with P&R approval and rejection. All the variables that had TPR positive opinion (n = 23) had P&R approval (except for two ODs which had P&R rejection) and all the variables that had TPR negative opinion (n = 4) had P&R rejected. Rarity of the disease, clinical outcome classification, therapeutic area and the existence of a therapeutic alternative were not statistically significant at 95% significance level.
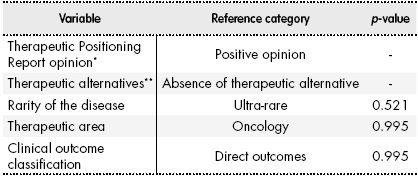
When the multivariate probit regression analysis was run, TPR opinion and existence of therapeutic alternatives were found to be related with P&R approval (n = 19). A positive TPR opinion and the existence of no therapeutic alternatives were related with a P&R approval. Rarity of the disease, clinical outcome classification and therapeutic area variables were not statistically significant at 95% significance level. Results are shown in Table 3.
Discussion
A total of 64 ODs were approved by the EC between January 2012 and June 2018 and with marketing authorisation in Spain. Mean time from EC approval to P&R approval for ODs in Spain was 22.5 ± 14.7 months; mean time from Spanish marketing authorisation to P&R approval was 13.7
± 5.1 months.
Based on the results of the report, having the EC and Spanish marketing authorisation approval does not guarantee access within the Spanish market, as from the 64 studied ODs, only 28 (44.4%) were reimbursed in Spain at the moment of the study, and the rest of ODs were either undergoing a long decision process or rejected, which prevents patients affected by rare diseases equitable and timely access to these drugs.
The shortness in the ODs regulatory timelines in recent years suggest that Marketing Authorisation Holder could be requesting reimbursement in Spain earlier than in the past and a considerable speed-up of the institutions in the Spanish administrative process. These results are in line with the growing concern about the need to have better and timely access to ODs across Europe and Spain, but P&R approval timelines are very large, considering that the official P&R decision process timeline in Spain is 180-270 days18.
In 2013, TPR was introduced in the P&R process14, however, it was not until 2016 it became a regular practice, so the TPR analysis could not be performed on all ODs approved during the study period. Data shows that ODs with positive TPR opinion were more likely to have P&R approval, while those who had obtained a negative opinion had P&R rejected.
In Europe, there is a lack of transparency and availability of information with regards to which criteria are used in real practice for P&R of ODs6. In recent years, actions have been made to try to reduce uncertainty surrounding the appraisal of ODs and to increase the process’ transparency, like the creation of specific frameworks to assess ODs24 or the publication of recommendations on principles to help improve the consistency of ODs P&R assessment in Europe25. A recent publication from Paulden et al.24 identified decision criteria that could influence P&R of ODs in published literature, some of which were found to be important in various papers, such as the availability of therapeutic alternatives, the evidence of clinical efficacy, the severity of the disease or the impact of treatment on life expectancy and quality of life. Another highlighted point by Paulden et al. is the diversity of views around P&R decision criteria, therefore it would be important to incorporate preferences of several stakeholders when making P&R decisions. The recent creation of specific frameworks for OD appraisal26 using the multi-criteria decision analysis methodology27, would provide more systematic and transparent evaluation process for ODs P&R.
This study has several limitations. The main one comes from the lack of or limited access to public information available for regulatory and P&R processes in Spain. From June 2012 to November 2017 there was no public information in Spain regarding dates for P&R approval, so to be able to analyse the time that an OD needs for P&R approval in Spain, the commercialisation date was used as a surrogate of approval date. Although this could have resulted in a slightly overestimation of time to market access, we do not expect this to be significant as when a drug’s P&R is approved in Spain, based on our experience, there can be a maximum delay of two months for it to be commercialised.
The results obtained when comparing regulatory timelines of ODs between years could be slightly modified by including longer follow-up periods, including ODs that were classified as “undergoing P&R decision process” at the moment of the study when obtaining a P&R final decision. Updates on regulatory approval timelines will be addressed in future updates of this study.
Explicit information about P&R rejection is not available in Spain, so indirect sources were used to know if an OD had had its P&R rejected, and therefore, some of the ODs that have been categorised as “under P&R decision process” might have seen their P&R rejected in Spain when no TPR was available. The reasons behind the lack of commercialisation of a given product remain unclear and impossible to evaluate with the present study.
On the statistical side, the regression analysis did not consider all the variables that might affect the P&R decision. For example, drug price or budget impact were not considered due to the lack of valid information in Spain. Although most companies include an economic evaluation (budget impact and cost-effectiveness analysis) in their P&R submission requests, it is not mandatory by law and this criterion is not used in practice for P&R in Spain. Finally, sample size used in the regression was small. This might decrease the statistical power of the analysis. The authors are currently working on gathering new valid data for the dataset. A further analysis might be done adding new variables that could influence P&R decisions.
The study showed that mean time of ODs P&R approval has shortened during the past years because of the effort made by the Spanish institutions involved in the process. It remains challenging to establish what driving criteria are used in the P&R process of ODs in Spain even though it was found that a positive TPR opinion and no therapeutic alternatives might be related with P&R approval. Although it is important to measure delays in patient access resulting from lengthy reimbursement processes, we highly recommend that efforts should be directed towards improving transparency in evaluation and multi-criteria decision-making, which should, in turn, lead to more effective processes and contribute to timely access of ODs to Spanish patients.
Contribution to scientific literature
The study adds new information about which orphan drugs have had pricing and reimbursement in recent years to the current literature of orphan drugs in Spain. To the knowledge of the authors, this is the first study that analyses the criteria that might determine pricing and reimbursement decision in Spain after the European Commission approval.
Results might help to understand why some orphan drugs receive positive pricing and reimbursement and others don’t, which might help to improve the approval timings as well as to improve accessibility for patients.

