










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Peer victimization is a problem of growing social concern due to its prevalence and negative consequences for the psychosocial well-being of adolescent students (Söderberg & Björkqvist, 2020; Van Geel et al., 2018). The results of the meta-analysis of 80 studies carried out by Modecki et al. (2014) showed that 36% of the adolescents studied felt victimized by their peers, with a percentage of severe victims ranging between 3% and 10%. Moreover, some authors have related victimization with peer aggression (Estévez et al., 2020; Walters, 2020), as well as with depressive symptoms (González-Cabrera et al., 2021; Hellfeldt et al., 2018).
Firstly, victims of peer aggression are the target of physical, verbal, relational, or psychological aggression carried out by some of their classmates with the aim of causing them harm (Graham, 2006; Martínez-Ferrer et al., 2018). Victimization has been associated in the scie.jpgic literature with a greater expression of peer aggression (Falla et al., 2020; León-Moreno et al., 2019). For example, in a recent meta-analysis conducted by Walters (2020) it was concluded that peer victimization and peer aggression are moderately correlated and that their longitudinal cross-relationships move in both directions, namely that it is as likely that perpetration will lead to future victimization as it is that victimization will result in future perpetration. Sentse et al. (2015) observed moderate to weak correlations between previous and later peer victimization and previous and later peer aggression (studied separately) for early and late adolescents followed up for 1 year. Other longitudinal studies have reported a positive correlation between peer victimization and peer aggression (Barker et al., 2008; Haltigan & Vaillancourt, 2014).
Secondly, according to Beck's (1963) cognitive theory, depression is mainly characterized by long periods of sadness that trigger distorted thought schemes, which in turn contribute to the negative way individuals perceive, encode, and interpret information about themselves, the world, and their future (Beck, 1963). Certain symptoms such as feelings of guilt and worthlessness, loss of appetite, helplessness and despair, sleep problems, and concentration problems are among the most common (Liu et al., 2021; Radloff, 1977).
Peer victimization has attracted the attention of researchers in recent years due to its negative influence on the mental health of victims. Longitudinal research has found that students victimized by their peers are more likely to display depressive symptoms over time (Kwong et al., 2019; Xiao-Wei et al., 2019). In their study, Li et al. (2019) found that students who had experienced peer victimization showed a propensity to present greater depressive symptoms one year later. Likewise, Takizawa et al. (2014) found that peer victimization between the ages of 7 and 11 years was associated with a higher prevalence of depressive symptoms at ages 23 and 50 years. In fact, long-term effects of victimization on mental health have been found even as late as 36 years after (Ttofi et al. 2011). These studies using longitudinal designs have allowed researchers to ide.jpgy the long-term effects that early victimization experiences can have on the mental health of victims.
Despite the available empirical evidence suggesting that peer victimization is related to aggressive behaviors and that it has negative effects on mental health, both in the short and long term, these relationships have rarely been analyzed jointly. Moreover, empirical evidence on the relationships over time between victimization, aggression, and mental health is largely lacking. Most studies conducted to date are correlational in nature and, therefore, have not analyzed in depth the trajectories of peer victimization, peer aggression, and depressive symptoms in adolescents. The advantage of studying trajectories over time is that it allows authors to analyze the way relationships between variables evolve. It also enables the ide.jpgication of markers (e.g., sociodemographic variables) that can explain differences in these trajectories. For instance, empirical research has found that victimization, aggression, and depressive symptoms are not equally distributed across genders (Lahav-Kadmiel & Brunstein-Klomek, 2018; Nuñez-Fadda et al., 2020). These studies have found, in this respect, that girls are more vulnerable than boys to the negative consequences (psychological and emotional problems) of peer victimization (Feijóo et al., 2021; Kim et al., 2018), probably due to their greater desire for acceptance and inclusion in the peer group (Baldry et al., 2017; Zhang et al., 2020). According to Morabito et al. (2021), when faced with these interpersonal stressors, girls tend to focus on their inner world and ruminate over the possible causes and consequences of their troubled relationships, while boys choose to defend themselves or even drop out of school (Sittichai & Smith, 2018). While these relationships have been reported in correlational studies, research on the influence of gender in the evolution of peer victimization, peer aggression, and depressive symptoms has been largely neglected.
The Present Study
Most empirical research on the relationship between peer victimization, aggression, and mental health has been conducted with correlational designs. Much of this research has also focused primarily on linking peer victimization with either the potential aggressive behaviors of victims or a deterioration in their mental health (Strohacker et al., 2021; Zhang et al., 2019). Joint studies of victimization, aggression, and mental health are less frequent (Zych et al., 2020), despite the compelling theoretical reasons for undertaking such research.
Peer victimization experiences result from the aggression of other peers. However, this does not exclude the fact that adolescents experience victimization because of their involvement in aggressive peer relations: sometimes they will perpetrate aggression and sometimes they will be the object of such aggressions. To differentiate between these two situations, which are quite distinct, it is necessary to assess not only victimization, but also potential aggressive behaviors directed towards others. Given that the analysis of victimization has been characterized by the study of its effects on mental health, it is important to differentiate any differences in the association of victimization and aggression with mental health. These research strategies are also conditional on obtaining quality data to explore the relationships studied. For this reason, it is essential to incorporate longitudinal designs that can be used to ide.jpgy trajectories in victimization, aggression, and mental health (Laith & Vaillancourt, 2022), as well as the different interrelationships between them over time.
This type of longitudinal design would allow researchers to answer questions such as “how do peer victimization and aggression evolve over time?”, “is this evolution related to the evolution of mental health?”, or “does gender play an important role in understanding the evolution of these variables?”. These questions guided this research and allowed us to ide.jpgy its two main objectives: a) to analyze the relationship over time between peer victimization, peer aggression, and depressive symptoms and b) to study whether these relationships are influenced by gender.
Method
Participants
The study participants were recruited from primary schools. The study began with the evaluation (T1) of participants in 5th grade of primary education when they were between 10-11 years old. A longitudinal study was conducted over a 36-month period, with measurements in three time periods: time 1 (T1, March 2019), time 2 (T2, March 2020), and time 3 (T3, March 2021). Students follow-up was as exhaustive as possible to minimize the possibility of them dropping out of the study. Two hundred and nineteen students were assessed at T1, 215 at T2, and 194 at T3. Ultimately, 194 students (49.2% male, 50.8% female; age in years, M = 10.88, SD = 0.84) completed the follow-up on the study variables. Twenty-five students dropped out of the study. Most of the students (90.9%) lived with both parents, 4.9% in a single-parent family (with only their mother), 0.2% in a single-parent family (with only their father), and 4% in a family of separated parents with joint custody.
Measurements
Peer Victimization
The adapted version into Spanish (Martínez-Ferrer et al., 2018) of the School Victimization Scale (Mynard & Joseph, 2000) was used. This Likert-type scale consists of 22 items that refer to peer victimization situations, with a response range from 1 (never) to 4 (always). The scale has three dimensions: relational victimization (e.g., “When a classmate has been angry with me, they have separated me from my group of friends so that I could not play or participate in a specific activity”), verbal overt victimization (e.g., “A classmate has shouted at me”), and physical overt victimization (e.g., “A peer struck or hit me to really harm me”). Previous studies have highlighted the adequate psychometric properties of the instrument in samples of adolescents (Martínez-Ferrer et al., 2021; Ye et al., 2022). In this study we used an overall score for the scale assessing the general victimization experienced by the student, adding the average scores of each subscale (range 3 to 12). The peer victimization average global scores for the three periods were respectively T1 (5.28), T2 (4.31), and T3 (3.97). Cronbach's alphas for the three dimensions were above .78. Confirmatory factor analysis (CFA) showed a good fit of the model to the data (SBχ2 = 313.56, df = 17, p = .001, CFI = .94, RMSEA = .04 [.036, .050]), thus ensuring that an overall peer victimization score adequately reflected the structure of the scale.
Peer Aggression
An adapted version into Spanish (Martínez-Ferrer et al., 2018) of the Aggressive Behavior Scale (Little et al., 2003), was used. This Likert-type scale consists of 25 items that measure participation in aggressive behavior toward peer groups, with a response range from 1 (never) to 4 (always). The scale has six dimensions: pure overt aggression (e.g., “I am a person who hits, kicks, and punches others”), reactive overt aggression (e.g., “When someone harms or hurts me, I hit them”), proactive overt aggression (e.g., “I threaten others to get what I want”), pure relational aggression (e.g., “I am a person who tells their friends not to hang around or go out with others”), reactive relational aggression (e.g., “If someone hurts or harms me, I don't let that person be part of my group of friends”), and proactive relational aggression (e.g., “To get what I want, I tell my friends not to hang around or go out with others”). Previous studies have highlighted the adequate psychometric properties of the scale in samples of adolescents (Jiménez et al., 2021; Romero-Abrio, 2019). For this study, an overall aggression score was used by adding the scores on the different subscales (range from 5 to 20). The average global peer aggression scores for the three time-periods were respectively T1 (8.01), T2 (7.21), and T3 (6.48). Cronbach's alphas for the six dimensions were above .81. CFA showed a good fit of the model to the data (SBχ2 = 527.54, df = 24, p = .001, CFI = .93, RMSEA = .03 [.023, .030]), thus ensuring that an overall peer victimization score adequately reflected the structure of the scale.
Depressive Symptoms
A 7-item Spanish version of the Center for Epidemiological Studies Depression Scale (Radloff, 1977) was used, as proposed by Herrero & Meneses (2006). This Likert-type scale consists of 7 items that measure aspects related to depression symptoms, with a response range from 1 (never) to 4 (always), (e.g., “In the last month, I felt as if I could not shake off the sadness, even with the help of my family or friends”). Previous studies have highlighted the adequate psychometric properties of the instrument across ages (Crockett et al., 2005; Herrero & Gracia, 2007; Juarros-Basterretxea et al., 2021). In this study we used an overall score for the scale to assess the general depressive symptoms experienced by students, adding the scores (reverse items were recoded), ranging from 7 to 28, and then dividing by the number of items (7) to obtain a final range from 1 to 4. The average global depressive symptoms score for the three periods were respectively T1 (1.84), T2 (1.62), and T3 (1.46). Cronbach's alphas were above .87. CFA showed a good fit of the model to the data (SBχ2 = 15.3403, df = 9, p = .082, CFI = .99, RMSEA = .03 ([.000, .069]), thus guaranteeing that an overall depression score adequately reflected the structure of the scale.
Procedure
All primary schools in a town of 9,436 inhabitants in southern Spain – 4 in total – were contacted and invited to participate in the study. All the schools expressed their interest in participating, so meetings were organized with the school principals and representatives of the families to explain the objectives of the research. For this purpose, the research team carried out an informative seminar with the school staff and the families to explain the objectives, the scope of the study and the procedure to be followed during the three academic years of the longitudinal study. At this step, the necessary permissions were requested from both the educational centers and the families to participate in the study. The battery of instruments was administered voluntarily and anonymously and supervised in two different sessions of approximately 45 minutes during school hours.
This study followed the guidelines established in the Declaration of Helsinki (1964): informed consent and right to information, protection of personal data and guarantee of confidentiality, non-discrimination, free of charge, and the possibility of abandoning the study in any phase. It was also required to comply with Organic Law 3/2018, of 5 December, on the Protection of Personal Data and Guarantee of Digital Rights in Spain. The collected data were: (1) treated confidentially (using a coding procedure that prevented the ide.jpgication of participants), (2) with use restricted to researchers only, (3) safeguarded at all times by investigators, and (4) used solely for the strict purposes of this research.
Analytical Strategy
To analyze the relationships between victimization, aggression and depressive symptoms, we conducted a study of their co-evolution over time. MPLUS 8.2 software (Muthén & Muthén, 2018) was used to estimate this set of relationships using the Latent Growth Modeling (LGM) technique. The main aim was to explain the between-subject variability in the parameters describing the growth curves.
As highlighted in scie.jpgic literature (Herrero et al., 2019), LGM uses two parameters to describe the growth trajectory: a factor of the initial level at the beginning of the study (intercept) and a growth factor (slope) (see Figure 1) (Duncan, et al., 2013). A statistically significant negative slope suggests that the mean levels of the sample decrease over time. A statistically significant positive slope indicates that the mean levels of the sample increase over time. A zero mean slope implies that there is no significant mean growth in the sample (neither an increase nor a decrease over time).

Figure 1. Latent Growth Model for Victimization, Aggression, and Depressive Symptoms. VIC1-VIC3 represent victimization from T1 to T3; AGR1-AGR3 represent aggression from T1 to T3; DS1-DS3 represent depressive symptoms from T1 to T3; intercepts are IVIC (intercept factor for victimization), IAGR (intercept factor for aggression), and IDS (intercept factor for depressive symptoms); slopes are SVIC (slope factor for victimization), SAGR, (slope factor for aggression), and SDS (slope factor for depressive symptoms); covariations among intercepts and slopes were freely estimated by the model.
To ide.jpgy the between-subject variability in their trajectories (i.e., that individual levels increase or decrease at different rates), slope variance was examined. A statistically significant variance of the slope suggests that not all participants in the sample grow or decline at the same rate. A non-significant variance of the slope suggests that the estimated trajectory does not vary across participants and is therefore a valid description for the entire sample (i.e., that all participants grow or decline at the same rate). For the factor of initial levels (intercept), its variability indicates whether all participants started the study at the same levels or whether these were heterogeneous (as is more common in this type of study with community samples).
For the estimation of model fit, we used χ2 and its associated likelihood for n degrees of freedom, the comparative fit index (CFI), and the root mean squared error of approximation (RMSEA) and its corresponding 90% confidence interval (CI). A CFI greater than .95 and an RMSEA less than .05 indicate a good model fit (Cangur & Ercan, 2015).
Results
An initial model was evaluated that considered the growth trajectories of victimization, aggression, and depressive symptoms to be related over time. This model included gender as a time-invariant covariate to estimate its effect on the initial levels of victimization, aggression, and depressive symptoms and in their evolution over time. An additional model with a second covariate (age) did not provide additional relevant information since age was not statistically related to the variables of the model. To preserve as much as possible a higher ratio between the number of participants and the number of variables in the model, we chose not to retain this additional model. The analyses were therefore based on the initial model with gender as a time-invariant covariate. Model fit was excellent (χ2 = 28.42, df = 20, p = .10; CFI = .98; RMSEA = .04, 90% CI [0.00, 0.09]), suggesting that the proposed model did not differ significantly from the true model and thus adequately represented the observed sample variability in victimization, aggression, and depressive symptoms over time.
The unstandardized parameters estimated by the model showed that the initial levels of victimization (M = 5.28, p < .001), aggression (M = 8.01, p < .001), and depressive symptoms (M = 1.84, p < .001), differed significantly from zero at the beginning of the study (T1) (see Table 1). With regard to their evolution over time, the average levels of growth in victimization (M = -0.64, p < .001), aggression (M = -0.75, p < .01), and depressive symptoms (M = -0.20, p < .04) estimated by the model indicated that throughout the follow-up period their average levels decreased for the entire sample.
Table 1. Unstandardized Parameter Estimates of Latent Growth Analysis.
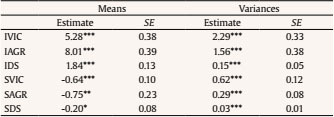
Note.IVIC = initial level of victimization; IAGR = initial level of aggression; IDS = initial level of depressive symptoms; SVIC = growth factor of victimization; SAGR = growth factor of aggression; SDS = growth factor of depressive symptoms; SE are standard errors.
*p < .05,
**p < .01,
***p < .001.
The between-subject variability of the study variables (see Table 1) showed that the initial levels of victimization (estimate = 2.29, p < .001), aggression (estimate = 1.56, p < .001), and depressive symptoms (estimate = 0.15, p < .001) were not the same for all the participants. Similarly, the study participants also showed different rates of growth in victimization (estimate = 0.62, p < .001), aggression (estimate = 0.29, p < .001), and depressive symptoms (estimate = 0.03, p < .001) over time.
While the estimated trajectories revealed a decrease in victimization, aggression, and depression over time, the model also provided information on relationship between these trajectories. Since the trajectories are defined from the initial level (intercept) and slope, the relationships between slopes provide information on the relationship between trajectories. The relationships between the intercepts provide information on the relationships of the variables at the beginning of the study.
The analysis of the relationship between victimization, aggression, and depressive symptoms (Table 2) showed that: a) higher levels of victimization at T1 were positively and significantly associated with higher levels of aggression at T1 (estimate = 1.24, p < .001) and T1 depressive symptoms (estimate = 0.43, p < .001); b) the levels of aggression and depressive symptoms at T1 were also positively and significantly related (estimate = 0.33, p < .001); c) the evolution of victimization and aggression showed a statistically significant relationship (estimate = 0.27, p < .01); d) the evolution of victimization and depressive symptoms showed a statistically significant relationship (estimate = 0.08, p < .01); e) and, finally, variations in depressive symptoms over time were statistically unrelated to variations in aggression (estimate = 0.04, p = .16). The fact that two negative slopes are positively correlated indicates that the greater the decline in one variable, the greater the decline in the other variable. Taken together, these results suggested that a smaller decrease in victimization over time was associated with a smaller decrease in aggression and depressive symptoms. Moreover, the evolution of aggression did not seem to be directly related to the evolution of depressive symptoms.
Table 2. Latent Growth Model Results: Covariances of Model Variables.
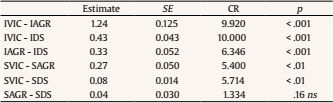
Note.IVIC = initial level of victimization; IAGR = initial level of aggression; IDS = initial level of depressive symptoms; SVIC = growth factor of victimization; SAGR = growth factor of aggression; SDS = growth factor of depressive symptoms; ns = non significant; SE are standard errors, CR are critical ratios.
Since the tendency of the participants was towards an unequal variation of victimization, aggression, and depressive symptoms over time, we analyzed the extent to which gender allowed us to ide.jpgy different trajectories in the participants of the study (see Table 3). Firstly, gender was statistically related to initial levels of victimization (b = - 0.87, p < .001), aggression (b = - 1.69, p < .001), and depressive symptoms (b = - 0.23, p < .01). This suggested that girls scored lower on victimization, aggression, and depressive symptoms at baseline. Secondly, the model did not ide.jpgy a significant effect of gender on the evolution of victimization over time (b = 0.18 p = .18) but did detect a significant effect of gender on the evolution of aggression (b = 0.48, p < .001), and depressive symptoms (b = 0.14, p < .01) over time.
Table 3. Unstandardized Parameter Estimates of Latent Growth Model Results: Effect of Gender on Study Variables.
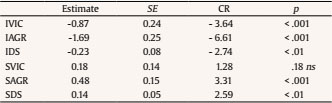
Note.IVIC = initial level of victimization; IAGR = initial level of aggression; IDS = initial level of depressive symptoms; SVIC = growth factor of victimization; SAGR = growth factor of aggression; SDS = growth factor of depressive symptoms; ns = non significant; SE are standard errors, C.R. are critical ratios.
Figure 2 presents a visual representation of the variations in victimization over the three time-periods for the overall sample and for boys and girls separately.

Figure 2. Estimation of Latent Growth for Peer Victimization for the Complete Sample, Boys, and Girls.
As shown in Figure 2, boys started the study with higher rates of victimization compared to girls. For both, victimization decreased over the course of the study, although the rate of reduction seemed greater for boys than for girls. Figure 2 shows that the line for boys was slightly steeper than for girls, although this difference was not statistically significant.
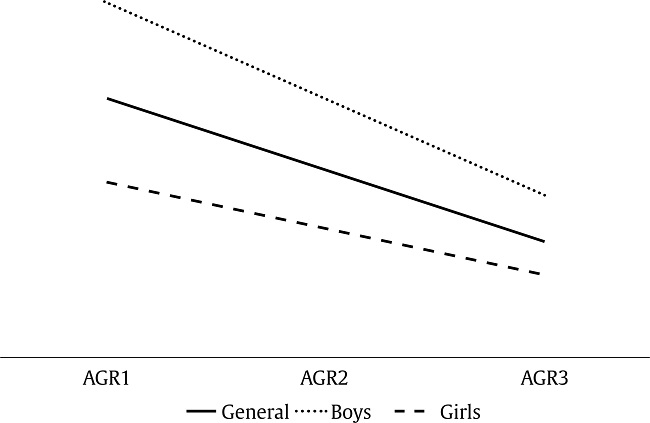
Figure 3. Estimation of Latent Growth for Peer Aggression for the Complete Sample for the Complete Sample, Boys, and Girls.
In the case of aggression, the same trend was also observed (see Figure 3). There was a trend for aggression in both boys and girls to decrease during the three time-periods, this decrease being more pronounced in boys than in girls. As presented above, the estimated decrease in aggression for boys was significantly greater than for girls.
Figure 4 shows the evolution of depressive symptoms over three-year time-periods, and the same trend appears: both boys and girls reported a reduction in their depression symptoms, but this reduction was significantly greater in boys than in girls.
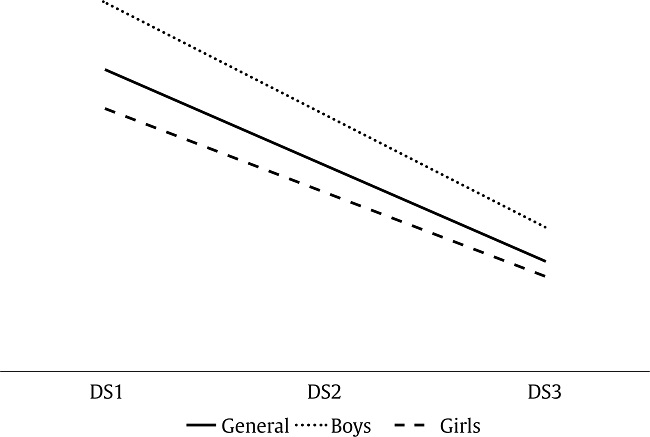
Figure 4. Estimation of Latent Growth for Depressive Symptoms for the Complete Sample, Boys, and Girls.
As compared to boys, girls experienced on average a smaller reduction in aggression and depressive symptoms over time. As noted above, the level of growth in aggression for an average participant was M = - 0.75. If the participants were girls, the reduction in aggression was significantly smaller (-0.75 + 0.48 = -0.27). In terms of depressive symptoms, the girls participating in the study showed a smaller reduction in depressive symptoms over time (-0.20 + 0.14 = -0.06) as compared to boys.
Overall, the results of the study showed that victimization, aggression, and depressive symptoms were not only related at their initial levels in the study, but also that changes over time in these variables were statistically related. A greater decrease in victimization was related to a greater reduction in aggression and depressive symptoms over time. However, variations in aggression did not seem to be related to changes in depressive symptoms. Since these relationships were partial regressions, once variations in victimization across different levels of aggression are taken into account, changes in aggression are not statistically related to changes in depressive symptoms.
Discussion
The study of peer victimization, aggression, and depressive symptoms has attracted the attention of researchers in recent decades due to its negative consequences for the psychosocial well-being of adolescents (Van Geel et al., 2018; Söderberg & Björkqvist, 2020). Most of these studies, however, have been conducted with correlational data and have focused on some, but not all, of these variables. This represents a potential limitation in this field of study that we aimed to address in our study.
This study had two overall objectives: a) to analyze the relationship over time of peer victimization, peer aggression, and depressive symptoms and b) to study whether these relationships are influenced by gender.
Firstly, the results from the estimated model suggested that the levels of these variables decreased over time among the study participants. This finding is consistent with those obtained in previous studies that suggest that violent behavior in the school population has a tendency to remit over time, which can be attributed to the maturity of the perpetrators of aggression (González-Cabrera et al., 2021; Xiao-Wei et al., 2019), as well as the victims' acquisition of coping skills and abilities to deal with victimization (Van Ouytsel et al., 2019; Zych et al., 2020). As a result, the depressive symptoms associated with these experiences of victimization would possibly also decrease (Kwong et al., 2019; Xiao-Wei et al., 2019), as our results also indicate.
Secondly, the results of the analyses of trajectories revealed that the more pronounced the reduction in victimization over time, the greater the reduction in depressive symptoms. These results confirmed those obtained in other studies which have reported that the experience of victimization increases the likelihood of greater depressive symptoms due to the fact that the peer group acquires a special relevance in adolescence (Nepon et al., 2021) and, consequently, it can have a negative impact on psychosocial adjustment and on the mental health of adolescents (Kwong et al., 2019; Xiao-Wei et al., 2019).
Thirdly, these results also seemed to be conditioned by gender. Not only did boys and girls show different levels of victimization, aggression, and depressive symptoms at the beginning of the study, but their trajectories also presented differences. In general, the decrease in aggression and depressive symptoms was significantly lower in girls as compared to boys. Although girls generally started with lower levels in the study variables, they self-reported a lower decrease over time as compared to boys. Particularly important was the clear slowdown in the reduction of victimization and depressive symptoms over time in girls. This result coincides with those obtained in other previous longitudinal studies (Bannink et al., 2014; Kim et al., 2018), which underline that victimization in adolescence may have a more negative effect on girls than on boys. This differential effect has been explained by the importance that girls attribute to their interpersonal relationships and also to the fact that girls think that they have been victimized due to their own actions (Morabito et al., 2021; Sittichai & Smith, 2018), thus increasing their tendency to ruminate on their possible causes and consequences. When faced with an initial situation of victimization, girls may experience more intense and prolonged stress as a result of these negative experiences (Xiao-Wei et al., 2019), which would also explain the slower reduction of their depressive symptomatology over time as compared to boys.
Overall, these results help advance our understanding of victimization, aggression, and mental health in adolescents. Firstly, the general trend pointed towards an overall improvement of the participants in the study: over the three time periods studied, peer victimization, aggression, and depression were in remission. However, this does not exclude the fact that some students presented significantly increased levels of victimization, aggression, and depression. The general trend, however, was towards a progressive decrease in the study variables. In addition, this general remission process evidenced mutual influences between the variables. Victimization and aggression evolved together and this had a clear influence on the mental health of students (Kochel et al., 2012).
The role of aggression in depression appears to be limited (Krygsman & Vaillancourt, 2019): although higher levels of aggression were associated with higher levels of depression at baseline, the trajectories of aggression and depression over time were shown to be statistically independent in the study participants. Other studies have longitudinally linked aggression with depression (Blain-Arcaro & Vaillancourt, 2017), although these studies do not include victimization and therefore cannot completely exclude a potential confounding effect.
Our research has important strong points and potential limitations. The longitudinal nature of the study is a strong point that allowed us to address certain limitations of previous studies in this area. Although the relationship between peer victimization, aggression, and depressive symptoms has been empirically proven in several cross-sectional studies (Strohacker et al., 2021; Zhang et al., 2019), the analysis of their evolution over time had been largely neglected, probably due to the greater research effort that longitudinal studies require as compared to cross-sectional studies. In addition, we used growth modeling to analyze trajectories which is a strength that allows to ide.jpgy the relationships between variables over time (Herrero et al., 2019; Herrero et al., 2022).
The results of the present study have certain limitations that should be highlighted. Firstly, although the sample was a strong point as it allowed us to access all the educational centers in the population, it also presented a potential limitation in terms of the generalizability of the results. However, due to the consistency of our results with the evidence available in scie.jpgic literature, we anticipate that this did not probably significantly affect the results of the study. A possible limitation related to the above was the ide.jpgication of a reduction in both victimization, aggression, and depressive symptoms. We cannot affirm that these processes tend to remit with age, since this may be due to the nature of the sample. Likewise, the observed decrease may also have been a collateral effect of the study design. It is possible that the adolescents were more aware of their situation due to the repeated administration of measurement instruments, which would translate into lower scores. Further research should focus on clarifying this point.
Also, our study found that aggression itself is not related to depressive symptoms. Previous cross-sectional studies have nevertheless shown a positive relationship between school aggression and depressive symptoms (e.g., Estévez et al., 2005; Estévez et al., 2018). This may have been due to our much smaller sample size and not sufficiently representative of the general population, which would explain why this relationship was not observed.
We believe that this study is very revealing and also very useful for the design of prevention programs to improve school coexistence and the mental health of victimized students, to the extent that it allowed us to study the co-evolution of victimization, aggression, and psychological distress. Our results indicate that experiences of victimization are not only related to aggression, but that the evolution of victimization is related to the evolution of depressive symptomatology, thus suggesting that prevention strategies emphasizing these variables should be considered. Likewise, the implementation of school interventions aimed at developing and improving mental health strategies can be beneficial, such as the promotion of emotional intelligence (Quintana-Orts et al., 2021), the enhancement of emotional control in students (Dray et al., 2017), the promotion of specific moral disconnection strategies (Romera et al., 2021), and favoring cohesion among students (Lucas-Molina et al., 2022) and collective school efficacy (Peraza-Balderrama et al., 2021). Also, interventions focused on transforming the implicit beliefs about the personality of adolescents (Incremental Theory of Personality Intervention), based on teaching that personality can change, have been shown to reduce the symptoms of anxiety and depression among adolescents and peer aggression (Calvete et al., 2021).
In summary, the results of the present study are interesting and complement existing information in previous literature regarding the importance of developing strategies focused on improving the mental health of adolescents as an effective way to prevent peer aggression.

