










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 no.3 Madrid may./jun. 2016
https://dx.doi.org/10.20960/nh.276
TRABAJO ORIGINAL / Epidemiología y dietética
Dietary patterns are associated with calcium and vitamin D intake in an adult Mexican population
Asociación entre los patrones dietarios y el consumo de calcio y vitamina D en población adulta mexicana
Edgar Denova-Gutiérrez1, Patricia Clark1,2, Paloma Muñoz-Aguirre3, Mario Flores4, Juan O. Talavera5, Laura Gabriela Chico-Barba6, Rodolfo Rivas5, Paula Ramírez3 and Jorge Salmerón3,7
1 Clinical Epidemiology Unit. Hospital Infantil de México Federico Gómez. Ciudad de Mexico, Mexico.
2 School of Medice. Universidad Nacional Autónoma de México. Ciudad de México. Mexico.
3 Unit of Epidemiologic Research and Health Services. Instituto Mexicano del Seguro Social. Cuernavaca, Morelos. Mexico.
4 Centro de Investigación en Nutrición y Salud. Instituto Nacional de Salud Pública. Cuernavaca, Morelos. Mexico.
5 Unit of Medical Research on Clinical Epidemiology. Centro Médico Nacional Siglo XXI. Instituto Mexicano del Seguro Social. Ciudad de México, Mexico.
6 Departament of Nutrition. Research on Community Intervention. Instituto Nacional de Perinatología. Ciudad de Mexico, Mexico.
7 Research Centre on Population Health. Instituto Nacional de Salud Pública. Cuernavaca, Morelos. Mexico
This study was financially supported by the Consejo Nacional de Ciencia y Tecnología (grant: 87783, and grant: 7876), Instituto Mexicano del Seguro Social, and Pfizer (unrestricted grant).
ABSTRACT
Introduction: Nutrition research has traditionally promoted a nutrient-based approach; however, to evaluate population compliance with dietary recommendations, researchers have increasingly used dietary pattern analysis.
Objective: To assess the relationship between dietary patterns and vitamin D and calcium intake in an adult Mexican population.
Methods: We characterized the dietary patterns of 8,456 men and women aged 20-80 years who were participating in the Health Workers Cohort Study. Information on participants' sociodemographic conditions and physical activity was collected via self-administered questionnaires. A food frequency questionnaire was used to assess diet. In a cross-sectional analysis, we examined dietary patterns in relation to vitamin D and calcium consumption.
Results: Factor analysis revealed 3 major dietary patterns. Pattern 1, labeled as "prudent pattern", was characterized by high positive loads for the consumption of fresh vegetables, fresh fruits, whole grains, oils, and legumes. The second dietary pattern, named as "dairy and fish pattern", was positively correlated with intake of dairy foods, fish and other seafood, milk and whole grains. Finally, dietary pattern 3 was associated with higher intake of red meat, soft drinks, fats, eggs, white meat and alcoholic beverages. Of these, the "dairy and fish pattern" was positively and significantly associated with vitamin D and calcium consumption (r = 0.42, p < 0.001; and r = 0.20, p < 0.001 respectively). Conversely, the third dietary pattern was negatively associated with vitamin D and calcium intake (r = -0.28, p < 0.001; and r = -0.41, p < 0.001, respectively).
Conclusions: In summary, our findings show that dietary patterns represented by high consumption of milk, dairy products, whole grains, fish are associated with higher consumption of vitamin D and calcium in Mexican adult population. Additionally, our results highlight the importance of following an appropriate dietary pattern to achieve adequate consumption of nutrients.
Key words: Dietary patterns. Factor analysis. Health workers cohort study. Calcium. Vitamin D.
RESUMEN
Introducción: tradicionalmente, la investigación en nutrición ha promovido un abordaje basado en el análisis de nutrimentos; sin embargo, más recientemente el análisis de patrones dietarios ha sido ampliamente utilizado para evaluar el apego de la población a las recomendaciones dietéticas.
Objetivo: evaluar la asociación entre los patrones dietarios y el consumo de calcio y vitamina D en población adulta mexicana.
Métodos: se derivaron patrones dietarios de 8.456 hombres y mujeres de 20-80 años de edad participantes de la Cohorte de Trabajadores de la Salud. La información sociodemográfica y de actividad física fue recolectada mediante cuestionarios autoadministrados. Para evaluar la información dietética, se utilizó un cuestionario de frecuencia de consumo de alimentos.
Resultados: mediante análisis factorial se derivaron tres patrones dietarios. El patrón 1, etiquetado como "patrón prudente", estuvo caracterizado por alto consumo de verduras frescas, frutas frescas, granos integrales, aceites y leguminosas. El segundo patrón, denominado "patrón de lácteos y pescado", fue positivamente correlacionado con ingesta de productos lácteos, pescado, leche y granos integrales. Finalmente, el tercer patrón dietario se asoció con alta ingesta de carnes rojas, bebidas azucaradas, grasas, huevos, pan blanco y bebidas alcohólicas. El patrón de lácteos y pescado se asoció positivamente con el consumo de vitamina D y calcio (r = 0,42, p < 0,001; r = 0,20, p < 0,001, respectivamente). Por último, el tercer patrón se asoció inversamente con el consumo de vitamina D y calcio (r = -0,28, p < 0,001; r = -0,41, p < 0,001 respectivamente).
Conclusión: nuestros hallazgos muestran que el patrón representado por un alto consumo de leche, productos lácteos, granos enteros y pescado está asociado con un mayor consumo de vitamina D y calcio en población adulta mexicana. Adicionalmente, nuestros resultados resaltan la importancia de seguir un patrón dietario apropiado para lograr un adecuado consumo de nutrientes.
Palabras clave: Patrones dietarios. Análisis factorial. Cohorte de trabajadores de la salud. Calcio. Vitamina D.
Introduction
Vitamin D and calcium are two important nutrients related primarily to bone health, but also with a variety of other diseases and health conditions (1). The main dietary sources of vitamin D and calcium are tuna, salmon, sardines, and dairy foods (2). Information regarding individual nutrients has been reported through the National Survey of Health and Nutrition 2006 (3,4). This survey shows that Mexican population has a suboptimal intake of calcium in all age groups. However, no information regarding vitamin D consumption is reported in the survey (3,4).
Traditionally, nutrition research has promoted a reductionist approach, focusing on intake of single nutrients as assessed with diet surveys (5,6). However, dietary pattern analyses have become more frequent in order to evaluate which populations are and are not complying with dietary recommendations (7). Dietary patterns are combinations of nutrients, foods and other dietary components which reflect a population's eating habits. Analyzing the intake of these patterns rather than single nutrients is useful because it more accurately accounts for the fact that humans eat complex meals and thus experience the interaction of multiple nutrients (8,9). This approach can also reveal relationships between diet and disease that are useful for the planning and execution of disease-prevention and healthy eating programs (10).
The relationships between dietary patterns and disease risks have been examined in many world regions, using statistical techniques such as factor analysis and cluster analysis to identify patterns (7,10,11). Prior research from Mexico has identified an association between specific dietary patterns and the presence of obesity (12,13), metabolic syndrome (9), insulin resistance (14), and gastric cancer (15). However, to date there are no reports on the relationship between dietary patterns and intake of specific nutrients, in Mexico or elsewhere. Therefore, the aim of this research is to examine the relationship between dietary patterns and vitamin D and calcium intake in an adult Mexican population.
Methods
PARTICIPANTS AND STUDY DESIGN
A cross-sectional analysis was carried out using data from participants in the baseline assessment of the Health Workers Cohort Study (HWCS). The details of the study design and methodology and baseline characteristics of the study population have been described previously (16). Briefly, the HWCS is a cohort study focusing on lifestyle and chronic diseases. It was initiated in 2004 with the enrollment of 10,769 employees and their relatives from 3 health and academic institutions in Morelos and Mexico states in Mexico. For the present analysis we excluded: a) participants < 20 or > 80 years (n = 1,557); b) participants with more than 10% blank items on their food intake information (n = 642); and c) participants with outlier daily energy intake values (outside the 600-7,000 kcal range) (n = 114) as assessed with the standard deviation method (17). A total of 8,456 participants (2,590 men and 5,866 women) were included in our final analysis.
This study was managed according to the Declaration of Helsinki guidelines. The ethics committees of all participating institutions (Comité de Ética e Investigación, Instituto Mexicano del Seguro Social, no. 12CEI0900614; Comité de Ética e Investigación, Instituto Nacional de Salud Pública, no. 13CEI1700736; Comité de Ética, Centro de Investigación en Ciencias Médicas, no. 1233008X0236) reviewed and approved the study protocol and informed consent forms.
DATA COLLECTION
After participants provided written informed consent, a self-administered questionnaire was used to collect information on participants' sociodemographic characteristics (e.g., age, sex and education), medical history and lifestyle, including diet and consumption of alcohol and tobacco.
Physical activity level was determined using a survey that was also used in similar follow-up studies (18). Participants reported the amount of time they spent each week on activities such as running and walking during a typical week in the previous year. Each activity was given a value in metabolic equivalent tasks (METs) and total METs/week was computed. Details of the measurement of physical activity are published elsewhere (19).
Body weight was measured with a previously calibrated electronic scale (model BC-533; Tanita, Tokyo, Japan), with participants wearing minimal clothing and no shoes. Height was measured using a conventional stadiometer (SECA brand), on barefoot subjects standing with their shoulders in a normal position; measurements were taken with the tape in a horizontal plane perpendicular to the vertical scale, touching the top of the head at the moment of inspiration. Body mass index (BMI) was computed as a ratio of weight in kilograms divided by height in meters squared. The definition for normal weight was BMI ≥ 18.5 and < 25.0, participants with BMI ≥ 25.0 - < 30.0 were classified as overweight, and those with BMI ≥ 30.0 were classified as obese.
VITAMIN D AND CALCIUM INTAKE
A semi-quantitative food frequency questionnaire (FFQ) was used to assess diet, energy and nutrient intake (20). The FFQ was validated by being administered twice, at a 1-year interval, to 134 women residing in Mexico City; the results were then compared with those from a set of 4 recall tests given at 3-month intervals. The questionnaire includes data describing the frequency of consumption of 116 foods during the previous year. The frequency of consumption reported for each food was converted to portions per day. In order to calculate the consumption of energy (kcal/day), the daily frequency of consumption (portions/day) of each food was multiplied by the food's energy content (obtained from a database of food contents) (21).
Vitamin D and calcium intakes were computed by multiplying the frequency of consumption of each food by the nutrient content of the specified portions. Composition values for dietary vitamin D and calcium were obtained using a database of food contents (21). Use of specific brands and types of multivitamins was determined by asking current users about weekly number of multivitamins taken. This information was included in the total vitamin D and calcium consumption calculation.
DIETARY PATTERN DERIVATION
Energy consumed from each food was converted into a proportion of the total consumption of energy per day and was subsequently standardized using Z scores (22,23). The foods and beverages on the questionnaire were categorized into 22 food groups that were used as the basis for the dietary pattern derivation. In short, the criteria for assigning a food to a particular food group were similarity of nutrient content (e.g., fats, proteins, carbohydrates) or proportion of dietary fiber. Other groups were classified based on their profile of fats (e.g., vegetable oils). Finally, some individual foods were considered to be groups in themselves because of their unique nutritional composition and/or because of the frequency with which they were consumed (e.g., corn tortillas and Mexican foods, potatoes, eggs, tomato juice) (Supplemental information; http://www.nutricionhospitalaria.org/nutricion-hospitalaria-vol-33-no-3-contenido-adicional/).
In order to derive the dietary patterns and to determine the factorial loads of each of the 22 groups, a factorial analysis of the main components was used (22,23). The factors were orthogonally rotated (varimax rotation) in order to keep them uncorrelated and to improve their interpretation. Factors with an eigenvalue above 1.5 were retained after the assessment of eigenvalues, graphic analysis and interpretability. Each factor was defined by a subset of at least 5 food groups with an absolute ≥ 0.2 load factor (considering that ≥ 0.2 load factors contributed significantly to the dietary pattern) as suggested in previous analyses (9,13-15,22). The factor scores for each dietary pattern were estimated by adding the consumption of the food groups weighted by their load factor, and each participant received a factorial score for each of the identified patterns.
STATISTICAL ANALYSIS
We performed a descriptive analysis of the principal characteristics (e.g., age, sex, BMI) of the study population across each of the dietary patterns grouped into tertiles. Continuous variables are presented as means and standard deviations and categorical variables as percentages and 95% confidence intervals. To investigate differences in participants' characteristics, we compared continuous variables using ANOVA tests. Finally, categorical variables were tested using Chi-square tests.
Correlations between dietary pattern scores and nutrient intake (vitamin D or calcium) were calculated with partial Pearson's correlations, including age (years), sex, total energy intake (kcal/day) and multivitamin use as covariates.
All the p values shown are two-tailed; a p value < 0.05 was considered to be statistically significant. All statistical analyses were carried out using the statistical software Stata, version 13.0 (StataCorp, College Station, TX, USA).
Results
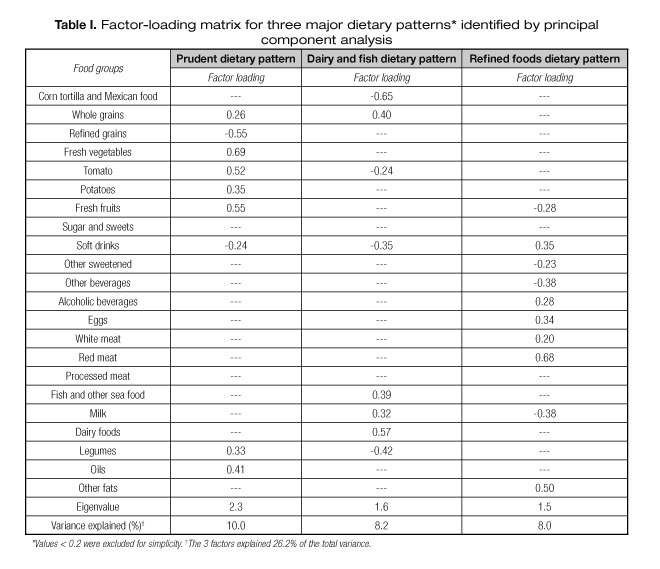
Factor loads for the dietary patterns identified by principal component analysis, which represents correlation coefficients between food groups and dietary patterns, are shown in table I. Factor analysis revealed three major dietary patterns. Pattern 1, labeled as "prudent pattern", was characterized by high positive loads for the consumption of fresh vegetables, fresh fruits, whole grains, oils, and legumes. The second dietary pattern, named as "dairy and fish pattern", was most strongly and positively correlated with intake of dairy foods, fish and other seafood, milk and whole grains, and negatively associated with consumption of legumes and soft drinks. Finally, dietary pattern 3, which we defined as "refined foods pattern", was associated with higher intake of red meat, soft drinks, fats, eggs, white meat and alcoholic beverages, and low intake of milk and fresh fruits. Together these patterns account for 26.2% of the total variance in food intake (10.0% by dietary pattern 1, 8.2% by pattern 2, and 8.0% by dietary pattern 3).
We found a total mean daily vitamin D intake of 241 UI in men and 251 UI in women. In the whole group, the total mean daily intake of calcium was 1,071 mg/day in women and a total mean daily calcium intake of 1,052 mg/day in men (data not shown).
Individuals with higher scores on the first dietary pattern tended to be older, smoke less, and consume less energy, vitamin D, and calcium. Furthermore, compared with participants in the lowest tertile, those in the highest tertile of the prudent pattern had a higher prevalence of obesity (p = 0.08) and multivitamin use (p < 0.001). In contrast, participants with high scores in the dairy and fish dietary pattern were significantly younger, smoked less, and consumed fewer multivitamins. Compared with those in the lowest tertile, participants in the upper tertile of dairy and fish pattern had higher intake of vitamin D (p < 0.001) and calcium (p < 0.001), and were more physically active and less likely to be obese. Lastly, those subjects in the highest tertile of the refined foods pattern were younger, had higher BMIs, and a higher prevalence of obesity compared with participants in the lowest tertile of the refined foods dietary pattern. They also had lower intakes of energy, vitamin D, and calcium (Table II).
In general, compared with those in the lowest tertile, participants in the upper tertile of the dairy and fish dietary pattern had higher intakes of skim milk, yogurt, dairy foods and fish. Participants with high scores in the prudent dietary pattern had lower consumption of whole milk, skim milk, cheese and yogurt than those in the lowest tertile of the prudent dietary pattern. Participants in the upper tertile of refined foods dietary pattern had lower intakes of different kinds of milk and dairy products (cheese and yogurt) than those in the lowest tertile of the refined foods dietary pattern (Table III).
Table IV presents Pearson's correlation coefficients between dietary patterns and vitamin D and calcium consumption. After adjusting for age (years), sex, total energy intake (kcal/day), and multivitamin use (yes or no), dairy and fish dietary pattern was positively and significantly associated with vitamin D consumption (r = 0.42, p <0.001) and calcium intake (r = 0.20, p < 0.001). Conversely, refined foods dietary pattern was negatively associated with vitamin D and calcium intake (r = -0.28, p < 0.001; and r = -0.41, p < 0.001 for vitamin D and calcium respectively).

Discussion
Using factor analysis, we found three major dietary patterns in this adult Mexican population. Of these, dairy and fish dietary pattern, characterized by high consumption of skim milk, dairy products, whole grains, fish and other seafood, and low consumption of soft drinks, was positively and significantly correlated with higher consumption of vitamin D and calcium. Conversely, refined foods dietary pattern, characterized by positive loads of soft drinks, alcoholic beverages, meats, eggs and fats and negative loads of milk and fresh fruits, was negatively correlated with calcium and vitamin D intake.
Interestingly, some characteristics of the dairy and fish pattern group might include them in a healthier style of life. They were in average significantly younger, with a lower percentage of smokers and a lower percentage of individuals taking multivitamins (we might infer that most of the nutrients were coming from the diet). Furthermore, in the highest tertile of this group, an association was found with less percentage of obese individuals and a higher level of physical activity. A recent study in Mexico reported that individuals younger than 45 years old had a higher perception risk of developing certain diseases, including osteoporosis, than older individuals. Younger people being more aware of disease might be one explanation for adopting a healthier lifestyle (24).
We found that our study population on average consumed less calcium and vitamin D than the recommended daily allowance (25). Thus, approximately 56% of men and women had inadequate consumption of calcium, and approximately 96% had inadequate intake of vitamin D. In addition, a recent study conducted in the central area of Mexico suggests that these findings are similar to those observed in another adult population from central Mexico, in which 43.5% of the population experienced vitamin D deficiency (< 50 nmol/L or < 20 ng/mL) (26), as well as throughout North America (27,28). For example, Bailey et al. (27) found that 95% of women and 96% of men in the US had inadequate consumption of vitamin D, while 44% of men and 70% of women aged 31-50 years had inadequate intake of calcium. The inadequate consumption of vitamin D in the diet is explained easily since vitamin D is found only in few foods, and in those it appears in low amounts.
Some limitations are inherent to the present study. Even though the food frequency questionnaire is a standard method for collecting information on dietary consumption, estimates originated from this instrument are not free from errors. However, in a recent study, Denova et al. found a reasonable comparability between the FFQ and 24-hour dietary recalls in typifying dietary patterns, supporting the utility of FFQs for assessing dietary patterns in adult Mexican populations (29). Principal component analysis, a form of exploratory factor analysis used to identify dietary patterns, has some weaknesses related to methodological variation including food grouping, number of food groups used in factor analysis, number of factors and the rotation employed, which could affect the interpretation of findings (30). In addition, dietary pattern analysis has been critiqued because, since factors are derived from the eating habits of the population under study, significant differences are observed between dietary patterns of individuals from different cultures, geographic locations and races which, in the other hand, might be as well an advantage since it reflects a particular population. In the present study, the participants in this cohort are adults from a specific segment of the Mexican population: working class, seemingly healthy individuals. While these adults cannot be considered to be representative of the Mexican adult population as a whole, they may be considered as representative of middle to low income adults from the mega polis of Mexico representing near one fourth of the Mexican population.
In conclusion, findings from this study show that the dairy and fish dietary pattern represented by high consumption of skim milk, dairy products (mainly cheese and yogurt), whole grains, fish and seafood (Table III) is associated with higher consumption of vitamin D and calcium in an adult Mexican population and with a healthier lifestyle pattern. Despite the fact that a diet high in dairy would also be high in saturated fats and thus contravene dietary recommendations (31), our data suggest that in a particular dietary pattern moderate consumption of skim milk and other dairy products could improve intake of calcium and vitamin D. Overall, our results highlight the importance of following an appropriate dietary pattern to achieve adequate consumption of nutrients. Nutrients should come primarily from foods; however, dietary supplements or fortified foods may be useful for increasing intake of a specific vitamin or mineral, and in this case vitamin D will be a desirable fortification in the light of the epidemics of vitamin D deficiency over the world. For this reason, the food industry could increase the levels of vitamin D and calcium added to certain foods, in order to improve the consumption of these nutrients in the Mexican population.
More observational dietary patterns research, such as studies of how close the population is to meeting key dietary guidelines, is needed. Such studies are important bases for dietary recommendations, government programs, and negotiations with industry that can help Mexican people to achieve certain dietary recommendations and healthy food choices. Such research could also lay the groundwork for large scale primary prevention trials focused on dietary patterns and healthy food choices that would allow us to evaluate which aspects of the population's diet are closest to their targets and which need improvement. In this regard, funding should be increased for intervention trials involving multiple dietary changes. Additionally, research is needed to increase understanding of the implications of dietary patterns identified in our population for bone health.
Acknowledgements
The authors are grateful to Emily Wentzell, Ph.D., for improving the manuscript with her editorial work.
References
1. Autier P, Boniol M, Pizot C, Mullie P. Vitamin D status and ill health: A systematic review. Lancet Diabetes Endocrinol 2014;2:76-89. [ Links ]
2. U.S. Department of Agriculture, Agricultural Research Service (2011): USDA National Nutrient Database for Standard Reference, Release 24. Nutrient Data Laboratory. In: http://www.ars.usda.gov/ba/bhnrc/ndl. [ Links ]
3. Flores M, Macias N, Rivera M, Barquera S, Hernández L, García-Guerra A, et al. Energy and nutrient intake among Mexican school-aged children, Mexican National Health and Nutrition Survey 2006. Salud Publica Mex 2009;51(Suppl. 4):S540-S550. [ Links ]
4. Baquera S, Hernández-Barrera L, Campos-Nonato I, Espinosa J, Flores M, J AB, et al. Energy and nutrient consumption in adults: Analysis of the Mexican National Health and Nutrition Survey 2006. Salud Publica Mex 2009;51(Suppl. 4):S562-S573. [ Links ]
5. Messina M, Lampe JW, Birt DF, Appel LJ, Pivonka E, Berry B, et al. Reductionism and the narrowing nutrition perspective: Time for reevaluation and emphasis on food synergy. J Am Diet Assoc 2001;101:1416-9. [ Links ]
6. Jacobs DR, Steffen LM. Nutrients, foods, and dietary patterns as exposure in research: A framework for food synergy. Am J Clin Nutr 2003;78(Suppl. 3):508S-513S. [ Links ]
7. Tucker KL. Dietary patterns, approaches, and multicultural perspective. Appl Physiol Nutr Metab 2010;35:211-8. [ Links ]
8. Hu FB. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr Opin Lipidol 2002;13:3-9. [ Links ]
9. Denova-Gutiérrez E, Castañón S, Talavera JO, Gallegos-Carrillo K, Flores M, Dosamantes-Carrasco D, et al. Dietary patterns are associated with metabolic syndrome in an urban Mexican population. J Nutr 2010;140:1855-63. [ Links ]
10. Jacques PF, Tucker KL. Are dietary patterns useful for understanding the role of diet and chronic disease? Am J Clin Nutr 2001;73:1-2. [ Links ]
11. Ciprián D, Navarrete-Muñoz EM, García de la Hera M, Giménez-Monzo D, González-Palacios S, Quiles J, Vioque J. Patrón de dieta mediterráneo y occidental en población adulta de un área mediterránea: Un análisis clúster. Nutr Hosp 2013;28(5):1741-9. [ Links ]
12. Flores M, Macías N, Rivera M, Lozada A, Barquera S, Rivera-Dommarco J, et al. Dietary patterns in Mexican adults are associated with risk of being overweight or obese. J Nutr 2010;140:1869-73. [ Links ]
13. Denova-Gutiérrez E, Castañón S, Talavera JO, Flores M, Macías N, Rodríguez-Ramírez S, et al. Dietary patterns are associated with different indexes of adiposity and obesity in an urban Mexican population. J Nutr 2011;141:921-7. [ Links ]
14. Romero-Polvo A, Denova-Gutiérrez E, Rivera-Paredez B, Castañón S, Gallegos-Carrillo K, Halley-Castillo E, et al. Association between dietary patterns and insulin resistance in Mexican children and adolescents. Ann Nutr Metab 2012;61:142-50. [ Links ]
15. Denova-Gutiérrez E, Hernández-Ramírez R, López-Carrillo L. Dietary patterns and gastric cancer risk in Mexico. Nutr Cancer 2014;66:366-76. [ Links ]
16. Denova-Gutiérrez E, Huitrón-Bravo G, Talavera JO, Castañón S, Gallegos-Carrillo K, Flores Y, et al. Dietary glycemic index, dietary glycemic load, blood lipids, and coronary heart disease. J Nutr Metab 2010;pii:170680. DOI:10.1155/2010/170680. [ Links ]
17. Rosner B. Percentage points for a generalized ESD many-outlier procedure. Technometrics 1983;25:165-72. [ Links ]
18. Martínez-González MA, López-Fontana C, Varo JJ, Sánchez-Villegas A, Martínez JA. Validation of the Spanish version of the physical activity questionnaire used in the Nurses' Health Study and the Health Professionals' Follow-up Study. Public Health Nutr 2005;8:920-7. [ Links ]
19. Méndez-Hernández P, Flores Y, Siani C, Lamure M, Dosamantes-Carrasco LD, Halley-Castillo E, et al. Physical activity and risk of metabolic syndrome in an urban Mexican cohort. BMC Public Health 2009;9:276. [ Links ]
20. Hernández-Ávila M, Romieu I, Parra S, Hernández-Ávila J, Madrigal H, Willett W. Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico City. Salud Pública Mex 1998;40:133-40. [ Links ]
21. Hernández-Ávila M, Resoles M, Parra S. Sistema de Evaluación de Hábitos Nutricionales y Consumo de Nutrimentos (SNUT). Cuernavaca, Mexico: INSP; 2014. [ Links ]
22. Newby PK, Weismayer C, Akesson A, Tucker KL, Wolk A. Long-term stability of food patterns identified by use of factor analysis among Swedish women. J Nutr 2006;136:626-33. [ Links ]
23. Kim JO, Muller C. Factor analysis. Newbury Park, CA: Sage Publications, Inc.; 1984. [ Links ]
24. Clark P, Lavielle P. Risk perception and knowledge about osteoporosis: Well informed but not aware? A cross-sectional study. J Community Health, 2014. DOI 10.1007/s10900-014-9923-x. [ Links ]
25. Institute of Medicine: Dietary reference intakes for calcium and vitamin D. Washington, DC: The National Academies Press; 2011. [ Links ]
26. Chico G, Rivas R, Clark P, Vivanco N, Huitrón-Bravo G. Nonlinear relationship between 25-hidroxivitamin D and PTH levels in a sample of Mexican population. Osteoporosis Int 2013;24(Suppl. 1):S359. [ Links ]
27. Bailey RL, Dodd KW, Goldman JA, Gahche JJ, Dwyer JT, Moshfegh AJ, et al. Estimation of total usual calcium and vitamin D intakes in the United States. J Nutr 2010;140:817-22. [ Links ]
28. Poliquin S, Joseph L, Gray-Donald K. Calcium and vitamin D intakes in an adult Canadian population. Canadian Journal of Dietetic Practice and Research 2009;70:21-7. [ Links ]
29. Denova-Gutiérrez E, Tucker KL, Salmerón J, Flores M, Barquera S. Validity of dietary patterns in an adult Mexican population assessed by a food frequency questionnaire. PhD Thesis. Instituto Nacional de Salud Pública, Centro de Investigación en Nutrición y Salud; 2014. [ Links ]
30. Martínez ME, Marshall JR, Sechrest L. Factor analysis and the search for objectivity. Am J Epidemiol 1998;148:17-9. [ Links ]
31. Astrup A. Yogurt and dairy product consumption to prevent cardiometabolic diseases: Epidemiologic and experimental studies. Am J Clin Nutr 2014;99(Suppl. 5):1235S-1242S. [ Links ]
![]() Correspondence:
Correspondence:
Patricia Clark.
Clinical Epidemiology Unit.
Hospital Infantil de México Federico Gómez.
Ciudad de Mexico, Mexico
e-mail: patriciaclark@prodigy.net.mx
Received: 04/12/2015
Accepted: 17/02/2016
