










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.1 Madrid ene. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Wilkie's syndrome
Síndrome de Wilkie o pinza aortomesentérica
Carlos Oliva-Fonte1, Cristina Lidia Fernández-Rey2, Javier Pereda-Rodríguez1 and Ana María González-Fernández2
Departments of 1Radiodiagnosis, and 2General Surgery and Digestive Diseases. Hospital General de Segovia. Segovia, Spain
Case report
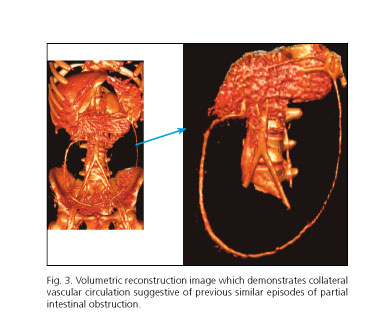
We report the case of a 14-year-old woman who presented epigastric abdominal pain, abundant vomits and an important abdominal distension for some days. Previously, she had had similar episodes. She had not any significant prior medical history. On examination, she presented distended and tympanic abdomen, without peritoneal irritating sings. CT was performed and findings resulted in diagnostic of Wilkie's syndrome (Fig. 1). Conservative management was adopted. Subsequently, magnetic resonance angiography was performed (Fig. 2). After treatment, the patient was asymptomatic and presented oral tolerance (1).


Discussion
Wilkie's syndrome is a rare condition that results from an intestinal obstruction due to compression of the third part of the duodenum between the abdominal aorta and the superior mesenteric artery. When the angle between both structures diminishes and the distance between the SMA and the aorta decreases (the most diagnostic value), duodenal obstruction occurs (the normal angle ranges from 25o to 60o and the normal distance is 10 to 28 mm). In Wilkie's syndromes both parameters are reduced (6o to 15o and 2 to 8 mm) (2).
Initially conservative management is adopted, but in some cases surgical treatment is necessary. Usually, in cases with acute presentation medical treatment is sufficient, while chronic evolution requires surgery after parenteral nutrition. In conclusion, surgery is indicated if conservative management fails, in large evolution disease with significant weight loss and progressive duodenal dilatation or after complications such as peptic ulcer secondary to obstruction.
References
1. Kennedy KV, Yela R, Achalandabaso M del M, et al. Superior mesenteric artery syndrome: diagnostic and therapeutic considerations. Rev Esp Enferm Dig 2013;105:236-8. DOI: 10.4321/S1130-0108201 3000400012. [ Links ]
2. Bakker ME, Van Delft R, Vaessens NA, et al. Superior mesenteric artery syndrome in a 15-year-old boy during Ramadan. Eur J Pediatr 2014;173:1619-21. DOI: 10.1007/s00431-013-2190-5. [ Links ]
