










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Moderate physical activities such as yoga are linked with increases in well-being (Marquez et al., 2020), which is broadly defined as feeling good and functioning well (Keyes & Annas, 2009). Given that mental illnesses cause the world 1 trillion USD per year in terms of lost productivity (World Health Organization, 2017), using public funding to subsidize yoga and other activities has been proposed as a way of improving well-being (Bilderbeck et al., 2013; Cartwright et al., 2019). Indeed, yoga could be part of a suite of positive psychology interventions (PPIs) that works with other widely recognized PPIs, such as expressing gratitude (Bono et al., 2020), practising kindness (Hui & Kogan, 2018), and meditating (Galante et al., 2016). With the number of US yoga practitioners rocketing from 20.4 million to 55.1 million between 2012 and 2020 (Zuckerman, 2020), there is an increasing body of research on the benefits of yoga (e.g., Gupta & Maurya, 2020; Lim & Hyun, 2021). However, there were limitations in previous work.
Firstly, as reported in one systematic review and five meta-analyses, most previous studies have focused on the effects of yoga on the clinical population with physical issues or psychiatric disorders (Brinsley et al., 2020; Gonzalez et al., 2020; Li et al., 2021; W. L. Wang et al., 2020). In fact, there were only 12 and 17 studies on the general population reported in a systematic review (F. Wang & Szabo, 2020) and a meta-analysis (Hendriks et al., 2017), respectively. Secondly, most empirical studies used small sample sizes, and their study designs were of low quality. To put this into perspective, 90 out of 97 yoga studies covered in the above systematic review and meta-analyses used a sample size of less than 200 participants, which might not have enough power to (i) detect the main effect, (ii) examine the underlying mechanisms, and (iii) explore how individual differences moderate the effect. Thirdly, as proposed by Huppert et al. (2009), well-being is a multifaceted concept. Comprehensive well-being indicators have been used to better understand the beneficial effects of regular yoga (e.g., Divya et al., 2021; Moszeik et al., 2020). However, few studies have looked into the effects of hot yoga, a particular style of yoga that is now gaining a lot of attention (Clarke et al., 2015). Building on the previous studies of regular yoga, the current study employed a randomized controlled trial (RCT) design to look into the effects of hot yoga on various well-being indicators in 290 healthy participants. Furthermore, using the experience-sampling method (ESM), we tracked the moment-by-moment emotional/hedonic well-being of the participants. To sum up, the study had the following overarching goals: (a) to establish whether hot yoga has an impact on a comprehensive set of well-being measures through the experimental method, (b) to determine what mechanism is responsible for the psychological benefits of hot yoga, and (c) to identify whether particular sub-groups benefit more from hot yoga.
Comprehensive Well-being and Yoga Practice
Although the construct of well-being—and its measurements—is constantly evolving, well-being is generally regarded as a multifaceted concept of feeling good (Fredrickson, 2001) and functioning well (Waterman, 1993). Specifically, the experience of frequent positive emotions is referred to as hedonic well-being (Fredrickson, 2001), while the sense of functioning well and achieving self-actualization is often referred to as eudaimonic well-being (Waterman, 1993). Therefore, in addition to traditional measures of mental health, life satisfaction, and general health, both hedonic and eudaimonic indicators are necessary components of a comprehensive assessment of well-being (Thorsteinsen & Vittersø, 2020). Somewhat overlapping with eudaimonic well-being, flourishing refers to the optimal human functioning and consists of eight core components: meaning and purpose, supportive and rewarding relationships, engagement and interest, contribution to the well-being of others, competence, self-acceptance, optimism, and being respected (Diener et al., 2010; Howell & Buro, 2015). As research studies have shown that yoga may be beneficial to human flourishing among teachers (Conboy et al., 2010) and adolescents (Schulte, 2015), we extended the growing literature by investigating the effect of hot yoga on flourishing. To make the assessment thorough, we also looked into what people seek in hot yoga and whether it fulfils the widely promoted claims of boosting the sense of presence, mindfulness, and calmness in participants (e.g., Aryal, 2020; Isaacs, 2008). Thus, it is crucial to examine the effects of hot yoga on peace of mind (i.e., an internal state of peacefulness and harmony) (Lee et al., 2013) and mindfulness (i.e., non-judgmental and non-reactive awareness of experiences in the present moment) (Kabat-Zinn, 2005). Additionally, it is insightful to account for the nature of the practice of hot yoga and its fundamental components, which include mindfulness and the promise of increased emotional regulation (e.g., Patel et al., 2018). As such, the momentary emotional well-being of hot yoga users is also worth investigating.
A Brief History of Yoga and Hot Yoga
Yoga is a practice that can be traced back to 3300-1900 BCE (Crangle, 1994). It was described at the beginning of the common era, including within The Yoga Sutras of Patanjali (Bryant, 2015). Among various definitions, Patanjali defined yoga as "the suppression of the activities of mind" (Mallinson & Singleton, 2017, p. 55). Following this notion, yoga is understood as the calming of agitation in patterns of consciousness, so as to attain a state of physical and mental well-being called "samadhi" (bliss) (Mallinson & Singleton, 2017). To achieve mental thriving and the balance between mind and body, ancient yoga encompassed ethics, breath regulation, concentration, and meditation, and focused more on the mind than physical exercise. Over the years, it has evolved to centre on physical postures whilst retaining many of its historical components including mindful attention, emotional regulation, and breathing control (Singleton, 2010). Amongst various emerging yoga styles, hot yoga has become one of the most popular workouts across the US in the past decade (Clarke et al., 2015). This form of yoga consists of a set of 26 held postures and breathing exercises practised in room heated to 40°C , and is proposed to have additional benefits over other yoga styles (Choudhury, 2007). For example, hot yoga has been reported to bring extra physical benefits, since practising in the heat improves blood flow (Hunter et al., 2013; Perrotta et al., 2016), metabolic rate (Larson-Meyer, 2016; Pate & Buono, 2014), and flexibility (Tracy & Hart, 2013). The sequence of movements is also designed to work through the whole body, which stimulates internal organs, the muscular-skeletal system, and general coordination (Choudhury, 2007). Moreover, exercising in a hot and humid environment is mentally and physically challenging. As such, hot yoga is thought to help participants promote focus and awareness on breathing (Hewett et al., 2011), thereby boosting mindfulness, calmness, determination, and peace of mind. For the above reasons, hot yoga is often advertised as a way to improve one’s physical health and mental well-being, despite the lack of a scientific basis for such claims.
Yoga Research to Date
To date, the research on hot yoga and well-being in healthy adults has been limited. Nevertheless, empirical studies on regular yoga are available to offer insights into hot yoga’s potential efficacy. For instance, regular yoga has been shown to promote psychological flourishing (Conboy et al., 2010), eudaimonic well-being (Ivtzan & Papantoniou, 2014), and hedonic well-being (Narasimhan et al., 2011). It has also been shown to help control anger, fatigue and inertia (Khalsa et al., 2012), decrease mood disturbance and anxiety (Noggle et al., 2012), reduce depression in older adults (Patel et al., 2012), enhance resilience to workplace stress (Hartfiel et al., 2011), and even improve school performance in adolescents (Frank et al., 2017). A number of RCT and cross-sectional studies have demonstrated the effects of regular yoga on indicators of comprehensive well-being (e.g., Divya et al., 2021; Moszeik et al., 2020; Sahni et al., 2021). However, to the best of our knowledge, no RCT studies with a sufficiently large sample size have evaluated the effects of hot yoga on a comprehensive range of indicators of well-being, including mindfulness, peace of mind, mental health, flourishing, satisfaction with life, general health, and hedonic and eudaimonic well-being. Some research efforts have been made to examine the relationship between hot yoga and psychological well-being, including its effects on mindfulness and perceived stress (Hewett et al., 2011), mood (Mace & Eggleston, 2016), positive-/negative-affect and state-anxiety (Szabo et al., 2017), emotions and psychological resources (Park et al., 2020), as well as life satisfaction and core self-evaluation (Rissell et al., 2014). There are also studies that focus on the physical benefits of hot yoga, such as its effects on sleep quality (Kudesia & Bianchi, 2012), cardiovascular disease risk factors (Hunter et al., 2013), bone density (Sangiorgio et al., 2014), and general physical fitness (Tracy & Hart, 2013). Nonetheless, the sample size was small in most studies. Taking the above nine studies as an example, their sample sizes ranged from 9 to 157 participants (average = 55.38), with only one study (N = 21) following the RCT protocol (Tracy & Hart, 2013). Clearly, the correlational nature of most studies and their small sample sizes have limited the evidence-based and causal conclusions that can be drawn.
Building on the comprehensive well-being and yoga (and hot yoga) discussion above, we hypothesized that hot yoga intervention would have positive effects on a range of well-being indicators, including mindfulness, peace of mind, satisfaction of life, general health, eudaimonic well-being, flourishing, and mental health. In addition, based on the aforementioned research which suggests yoga practice may be beneficial to emotion regulation (e.g., Patel et al., 2018), and affects and emotions (e.g., Park et al., 2020; Szabo et al., 2017), it is plausible that yoga practice might also contribute to better momentary emotional well-being in the ESM study. Therefore, we hypothesized that hot yoga intervention would have a positive effect on momentary emotional experiences/hedonic well-being over time.
Harder to predict is the duration of such effects, which have generally been neglected by previous research. Leveraging the ESM design—which is seldom used in hot yoga studies—we considered it worth exploring whether the emotional well-being boost would fade out shortly or last until the next beep in the ESM study or the next day after hot yoga practice. Since there were no studies available for reference, we intended to make this hypothesis undirected. In other words, we hypothesized that the effect of hot yoga on momentary emotional well-being would last for an unknown period of time.
Mechanism of Action
For the past 10 years, research has generally focused on the underlying physiological and psychological mechanisms of yoga. According to the most widely-proposed physiological mechanism, certain yoga techniques (e.g., poses, breathing, focus, etc.) may down-regulate the hypothalamic-pituitary-adrenal axis and the sympathetic nervous system at multiple levels (Ross & Thomas, 2010). On the other hand, research on the psychological mechanisms is sparse, although some have suggested that yoga may improve stress management skills through enhanced mindfulness (Hewett et al., 2011; Jansen, 2005). It has also been proposed that the cognitive benefits of yoga can be attributed to the development of focus (Gothe et al., 2016), and the improved self-esteem can be mediated by an increased subjective sense of energy (Golec de Zavala et al., 2017). Despite the substantial evidence for the effects of mindfulness—an important component of yoga practice—on emotional regulation (Sedlmeier et al., 2012), little research has addressed how the emotional benefits of yoga might boost well-being. Probably the strongest clue is that research has shown yoga having a positive effect on emotional functioning (e.g., Daly et al., 2015), whilst other psychological research has revealed that emotions and psychological well-being are closely linked, especially in an ESM setting (e.g., Hui & Kogan, 2018). Collectively, these two lines of research suggest one possibility that hot yoga may increase positive emotions and reduce negative emotions, resulting in a higher level of overall well-being. Thus, we initially hypothesized that the effects of hot yoga intervention on the indicators of well-being would be mediated by momentary emotional experiences throughout the trial.
Yoga and Well-being: Are We All Equal?
Until now, there has not been enough research on hot yoga to draw conclusions as to how its effectiveness as a PPI may vary according to individual differences. However, research in other areas may be able to shed light on the topic. For example, a meta-analysis reviewing the effect of PPIs has found that individuals with the lowest scores of well-being benefit the most from interventions (Sin & Lyubomirsky, 2009). Meanwhile, research in clinical settings also suggests that there is a large potential for yoga to help individuals with the lowest levels of well-being. For instance, a meta-analysis investigating the effects of yoga on depression has shown that the most depressed individuals gain the most benefits from practising yoga (Cramer et al., 2013). Another empirical study has also demonstrated that hot yoga is particularly effective in reducing negative-affect and state-anxiety in individuals who are under substantial stress in daily life (Szabo et al., 2017). Whilst the above evidence suggests that those with the lowest well-being may get the most out of yoga in general, the moderating role of baseline well-being in the impact of hot yoga remains poorly understood and warrants further investigation. Taken together, we hypothesized that the indicators of baseline well-being would moderate the effects of hot yoga intervention on the momentary emotional experiences/hedonic well-being, such that people with lower (vs. higher) levels of baseline well-being would benefit more from the increase in momentary emotional experiences/hedonic well-being.
The Present Study
Despite the growing interest in the effects of yoga in general, research on hot yoga remains scarce, mostly comprises small sample sizes, and is largely centred on its physical and physiological benefits. As for the few studies that examine the psychological benefits, their interest lies solely in the clinical population. Furthermore, there is currently no comprehensive measures of well-being in hot yoga RCTs.
The existing literature gives hints on the effects of (i) regular yoga on comprehensive well-being, and (ii) hot yoga on some psychological well-being indicators. Consequently, we predicted that hot yoga would impact both hedonic and eudaimonic well-being, mindfulness, satisfaction with life, peace of mind, flourishing, general health, as well as emotional experiences/hedonic well-being. Past research on yoga has seldom looked into the duration of the effect. Leveraging the ESM design, the present study explored when the momentary emotional well-being boost would fade out. We also expected that the effects of hot yoga intervention on the indicators of well-being would be driven by an immediate increase in positive emotional experiences and a decrease in negative emotional experiences during the trial. Finally, as suggested by previous literature, we predicted that the effects of hot yoga intervention on emotional experiences/hedonic well-being would be more significant in people with lower levels of baseline well-being.
In sum, based on the past research, we formulated five hypotheses:
Hypothesis 1: Hot yoga intervention would have positive effects on a range of well-being indicators, including mindfulness, peace of mind, satisfaction of life, general health, eudaimonic well-being, flourishing, and mental health.
Hypothesis 2: Hot yoga intervention would have a positive effect on momentary emotional experiences/hedonic well-being over time.
Hypothesis 3: The effect of hot yoga on momentary emotional well-being would last for a certain period of time during the trial.
Hypothesis 4: The effects of hot yoga intervention on the indicators of well-being would be mediated by momentary emotional experiences throughout the trial.
Hypothesis 5: The indicators of baseline well-being would moderate the effects of hot yoga intervention on the momentary emotional experiences/hedonic well-being, such that people with lower (vs. higher) levels of baseline well-being would benefit more from the increase in momentary emotional experiences/hedonic well-being.
For our investigation, we took several methodological approaches in the RCT to overcome the limitations of past research. Firstly, we used a large sample size of 290 healthy adults, which provided us with sufficient data to examine individual differences in baseline well-being. Secondly, all participants were yoga-naïve (as determined from the telephone screening process) so that we could rule out any carry-over effects from past experience in yoga practice. Thirdly, we employed various measures to identify the facets of well-being that were most influenced by hot yoga. Finally, we adopted the ESM and asked all participants to report on their emotional experiences/hedonic well-being four times a day for six weeks. This allowed us to track the changes in their emotional well-being over time and observe whether these changes could explain the relationship between hot yoga and increased well-being.
Method
Participants
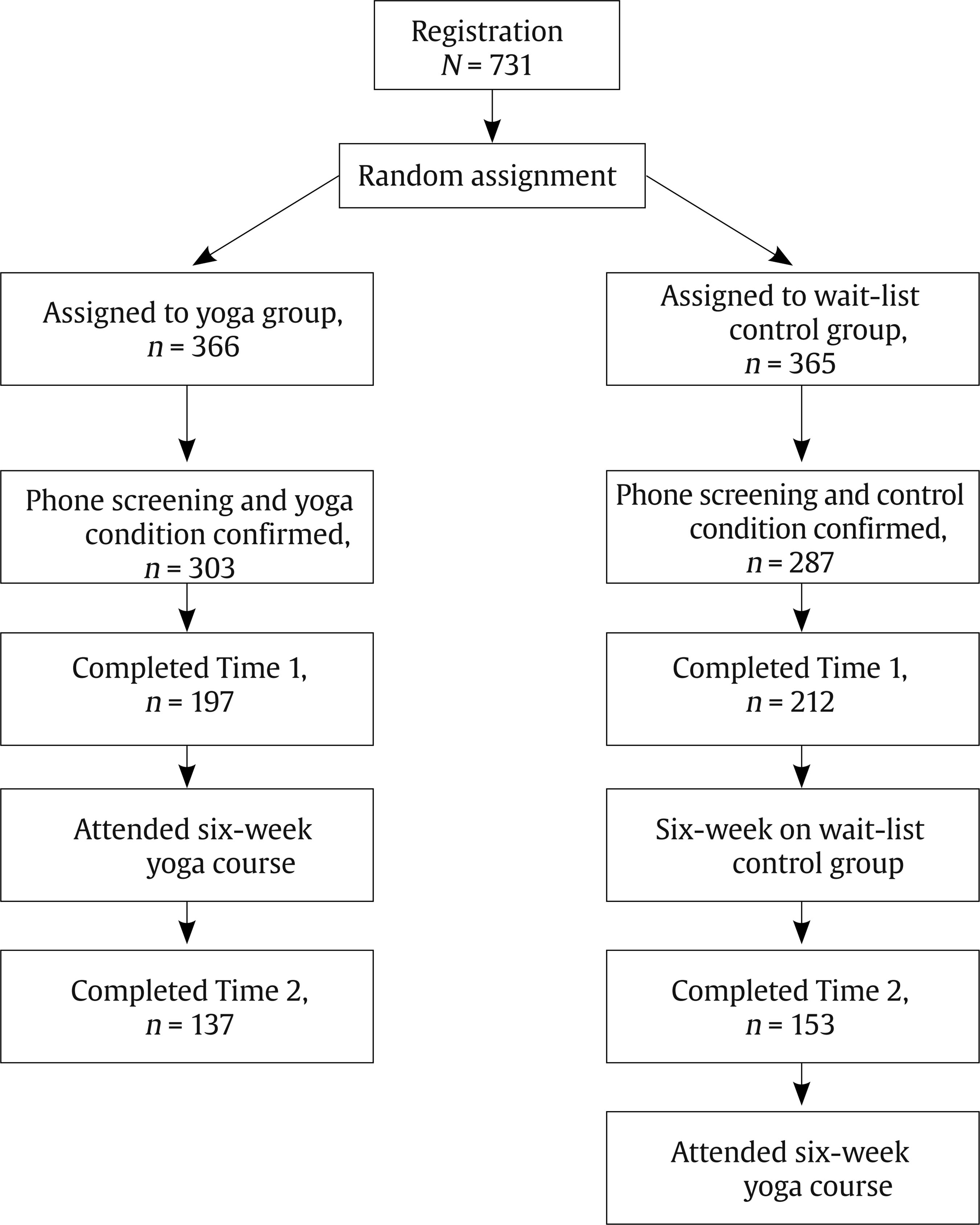
A community sample was recruited through advertisements in the local press, media outlets, newsletters, universities, local fairs, flyers, and street posters. A total of 290 participants completed the study based on their feasibility and availability (79% female; Mage = 29.43, SDage = 8.26, rangeage = 18-62; Mfemale age = 29.23, SDfemale age = 8.40, rangefemale age = 18-62; Mmale age = 30.32, SDmale age = 7.72, rangemale age = 18-55), with 137 in the experimental group (78% female; Mage = 29.54, SDage = 8.39, rangeage = 18-55; Mfemale age = 29.38, SDfemale age = 8.55, rangefemale age = 18-55; Mmale age = 30.38, SDmale age = 7.95, rangemale age = 18-55) and 153 in the wait-list control group (80% female; Mage = 29.34, SDage = 8.18, rangeage = 18-62; Mfemale age = 29.11, SDfemale age = 8.31, rangefemale age = 18-62; Mmale age = 30.27, SDmale age = 7.65, rangemale age = 18-47). The two groups did not differ significantly in their age and gender. Sample size and power analyses were not conducted prior to data collection. We used the proportion of variance explained by both the fixed and random factors (i.e., conditional R2) in our multilevel modelling analyses as an effect size. Assuming a small to medium effect size—ranging from .42 to .68 in our models—our sample size (Level-1: average number of beeps from each participant = 106; Level-2: number of participants = 290) was sufficient to produce a power estimate of .90 (Scherbaum & Ferreter, 2009).
Procedure
After expressing interest in joining our study, potential participants were randomly assigned to the hot yoga group or the wait-list control group. To ensure the participants met the study criteria, we screened them by telephone to double-check whether they: (a) were new to yoga; (b) had a smartphone; and (c) aged 18 or above (see Figure 1 for the whole process). All participants were told the purpose of the study (i.e., to investigate the impact of hot yoga on well-being), but remained unaware of the existence of the other experimental group. We received written consent from all of them to take part in the study and obtained ethical approval from the University of Cambridge Research Ethics Committee. Although no monetary reward was given to the participants, they were offered hot yoga intervention through six weeks of free classes (90 minutes per class, worth about £100 in total) at a studio in the city centre of Cambridge, UK. Participants were allowed to attend a maximum of four classes per week, with no minimum attendance requirements. Subsequently, they took part in an average of 17 (SD = 5, range = 6-24) out of 24 classes, which was equivalent to 2.8 classes per week. It should be noted that there was no minimum requirement of attending one class per week either. We divided the participants into two groups of attendance: high (≥ 17 classes) and low (< 17 classes), independent t-tests showing that there were no significant differences between the two groups in all well-being indicators (see Appendix A). On the other hand, the wait-list group also received six weeks of free yoga classes, but with a waiting period of six weeks. Participants filled in two online surveys at baseline (T1) and post-treatment (T2). Among those who had completed the first survey at T1, 60 of them dropped out of the hot yoga group and 59 dropped out of the wait-list control group. During the six-week study, participants also installed an ESM smartphone application which was available on both Android and iOS systems. The application was programmed to randomly beep them four times per day, asking them to report their momentary emotional experiences. At the end of the sampling period, participants completed an average of 106 (SD = 40, range = 6-166) momentary assessments, i.e., 2.5 beeps per day. No participants were excluded because of low participation, as long as they had completed the surveys at both T1 and T2.
Measures
Surveys at T1 and T2
Mindfulness. Mindfulness was usually tapped by the 39-item Five Facet Mindfulness Questionnaire (Baer et al., 2006). Because this measure had to be used in combination with other instruments and administered at multiple time points, this study employed a shorter version of the 24-item Five Facet Mindfulness Questionnaire (Bohlmeijer et al., 2011). To measure mindfulness, participants were asked to indicate on a 5-point Likert scale ranging from 1 (never or very rarely true) to 5 (very often or always true). Sample items included "I watch my feelings without getting carried away by them" and "I find it difficult to stay focused on what’s happening in the present moment (reverse item)". Due to the unstable factor structure and poor internal reliabilities of the subscores in the present study (see Appendix B), we decided to keep the measure as parsimonious as possible, and thus followed previous studies to assess the global dimension of mindfulness only (Baer et al., 2012; Duan, 2016). Similar to the Cronbach’s alpha of .74 in Cladder-Micus et al. (2019), the Cronbach’s alphas at T1 and T2 in this study were .72 and .69, respectively.
Peace of mind. Peace of mind was measured by the 7-item Peace of Mind Scale (Lee et al., 2013). Participants were asked to indicate how often they experienced the internal states described in each item (e.g., "My mind is free and at ease") on a 5-point Likert scale ranging from 1 (not at all) to 5 (all the time). The factor structure of this scale has been validated using confirmatory factor analysis (CFA), and the Cronbach’s alpha was .94 (e.g., Lee et al., 2013). In the present study, the Cronbach’s alphas at T1 and T2 were .82 and .81, respectively.
Satisfaction with life. The 5-item Satisfaction with Life Scale was employed for participants’ global evaluation of life satisfaction (Diener et al., 1985). Participants were asked to indicate agreement with each item (e.g., "I am satisfied with my life") on a scale of 1 (strongly disagree) to 7 (strongly agree). The factor structure of this scale has been validated using CFA (e.g., Whisman & Judd, 2016), and the Cronbach’s alpha in previous studies was high, specifically .82 and .87 (e.g., Diener et al., 1985). In the present study, the Cronbach’s alphas at T1 and T2 were .87 and .89, respectively.
General health. The 12-item General Health Questionnaire was employed to identify minor psychiatric illnesses (Donath, 2001). Participants rated themselves according to the degree to which they experienced each symptom (e.g., "felt constantly under strain") over the past few weeks on a scale of 1 (better than usual) to 4 (much less than usual). The factor structure of this scale has been validated using CFA, and the Cronbach’s alpha was .84 (e.g., Liang et al., 2016). In the present study, the Cronbach’s alphas at T1 and T2 were .84 and .81, respectively. A higher score reflected poorer general health.
Eudaimonic well-being. The 21-item Questionnaire for Eudaimonic Well-being was used to measure eudaimonic well-being (Waterman et al., 2010). Responses for all items were anchored on a 5-point scale, with 0 indicating strongly disagree and 4 indicating strongly agree. Sample items included "I can say that I have found my purpose in life" and "I believe I have discovered who I really am". The factor structure of this scale has been validated using CFA, and the Cronbach’s alpha was .85 (e.g., Waterman et al., 2010). In the present study, the Cronbach’s alphas at T1 and T2 were .78 and .81, respectively.
Flourishing. The 8-item Flourishing Scale was used to measure social-psychological prosperity, which complemented measures of subjective well-being (Diener et al., 2010). Participants rated their level of agreement with each item (e.g., "my social relationships are supportive and rewarding") on a 7-point Likert scale ranging from 1 (strongly agree) to 7 (strongly disagree). The factor structure of this scale has been validated using CFA (e.g., Datu et al., 2020), and the Cronbach’s alpha was .87 (e.g., Diener et al., 2010). In the present study, the Cronbach’s alphas at T1 and T2 were .88 and .87, respectively.
Mental well-being. The 14-item Warwick-Edinburgh Mental Well-being Scale was employed to assess positive aspects of mental health (Tennant et al., 2007). Participants selected what best described their experience of each statement over the past two weeks (e.g., "I’ve been feeling cheerful" and "I’ve been feeling confident") using a 5-point Likert scale ranging from 1 (none of the time) to 5 (all of the time). The factor structure of this scale has been validated using CFA, and the Cronbach’s alphas were .89 and .91 (e.g., Tennant et al., 2007). In the present study, the Cronbach’s alpha was .92. This scale was used at T1 only for testing whether participants with lower levels of well-being benefited the most from the increase in momentary emotional experiences.
Measure in ESM study
Momentary emotions. To maintain sufficient conceptual distinction between positive and negative emotions while keeping the survey brief, we used eight sets of positive and negative emotions from the Modified Differential Emotion Scale (Fredrickson et al., 2003). The four sets of positive emotions included: (1) glad, happy, joyful; (2) grateful, appreciative, thankful; (3) interested, alert, curious; and (4) proud, confident, self-assured. In contrast, the four sets of negative emotions included: (1) angry, irritated, annoyed; (2) ashamed, humiliated, disgraced; (3) disgust, distaste, revulsion; and (4) repentant, guilty, blameworthy. We first gave participants the following instruction: "Please rate the extent to which you have felt each of the following emotional experiences since the last beep." Then, participants were asked to respond to each of the above eight sets of emotions starting by "I feel..." on a 5-point Likert scale ranging from 1 (not at all), 2 (a little bit), 3 (moderately), 4 (quite a bit), to 5 (extremely). The positive and negative emotion scores were derived by summing the corresponding sets, respectively. Average Cronbach’s alphas for positive emotion and negative emotion in this study were .85 and .72, respectively.
Data Analysis
The present dataset included participants’ data at T1 and T2 as well as the ESM data. Thus, it had a multilevel structure with participants’ momentary emotional experiences (level-1) nested within individuals (level-2). We analysed data at T1 and T2 using multiple linear regression, which was implemented via the psych package (Revelle, 2018) in R. The effect size was captured by the change of R2 (ΔR2) between the final and previous models. To examine the data from the ESM study, we used the multilevel modelling (MLM) framework (Raudenbush & Bryk, 2002) through the lem4 package (Bates et al., 2015) in R. Due to the nested structure of the data, the effect size was quantified by a conditional R2 value which represented the total variance explained by both fixed and random effects (Nakagawa et al., 2017). In addition, we conducted multilevel mediation with Mplus (Preacher et al., 2011; Preacher et al., 2010). The effect size was represented by the percentage of the explained variance in a model which was contributed by the mediated effect (Fairchild et al., 2009). Finally, we conducted a bootstrap analysis in which bias-corrected confidence intervals were constructed by drawing 5,000 random samples with replacement from the full sample. For handling missing data, listwise deletion of cases was used when running multiple linear regression for data at T1 and T2. After noticing that 6% of values in the dataset had missing values, we imputed those missing values with R’s MICE package (Buuren & Groothuis-Oudshoorn, 2011) using predictive mean matching with five iterations. The two missing data handling methods did not produce substantially different multiple linear regression results. MLM dealt with missing data by allowing individuals to contribute partial data and using their data for the occasions where they contributed. In the ESM dataset, neither the missing patterns relating to the sequence of time variable nor the fluctuations of momentary emotions at different time points were random. This means that these missing values could not be predicted by existing data, so multiple imputation might not be applicable. However, there were 1.9 to 3.4% of data missing from the same momentary assessment in each of the statistical models we ran. Thus, multiple imputation was conducted for those missing values via the pan package (Zhao & Schafer, 2018) in R. No MLM results showed any substantial differences in datasets with and without multiple imputation. As for the multilevel mediation model conducted using Mplus, full-information maximum-likelihood estimation was used as a default to account for any missing data. All data and code used in the study are available from the corresponding author upon request.
Table 1. Means, Standard Deviations, Reliability Coefficients, and Correlation for the Measures at Time 1 and Time 2 (N = 290)

Note. 1Male = 1, female = 2; MFT1 = mindfulness at Time 1; PoMT1 = peace of mind at Time 1; SWLT1 = satisfaction with life at Time 1; GHT1 = general health at Time 1; EUWBT1 = eudaimonic well-being at Time 1; FlsT1 = flourishing at Time 1; MFT2 = mindfulness at Time 2; PoMT2 = peace of mind at Time 2; SWLT2 = satisfaction with life at Time 2; GHT2 = general health at Time 2; EUWBT2 = eudaimonic well-being at Time 2; FlsT2 = flourishing at Time 2; WEMT1 = Warwick-Edinburgh Mental Well-being at Time 1.The reliability coefficients are found along the diagonal line.*p < .05, **p < .01, *** p < .001.
Table 2. Multiple Regression Models Predicting the Effect of Hot Yoga on Post-Treatment Well-being Indicators

Note. 1Male = 1, female = 2; 2wait-list control = 0, hot yoga = 1; MFT1 = mindfulness at Time 1; PoMT1 = peace of mind at Time 1; SWLT1 = satisfaction with life at Time 1; EUWBT1 = eudaimonic well-being at Time 1; GHT1 = general health at Time 1; FlsT1 = flourishing at Time 1; MFT2 = mindfulness at Time 2; PoMT2 = peace of mind at Time 2; SWLT2 = satisfaction with life at Time 2; EUWBT2 = eudaimonic well-being at Time 2; GHT2 = general health at Time 2; FlsT2 = flourishing at Time 2.*p < .05, **p < .01, ***p < .001.
Results
Descriptive statistics and correlation coefficients for age, gender, and measures of well-being at T1 and T2 are presented in Table 1. Age was significantly correlated with some measures of well-being, such as mindfulness at T1 (r = .12, p = .047) and T2 (r = .13, p = .031), satisfaction with life at T1 (r = -.19, p = .001) and T2 (r = -.18, p = .003), as well as eudaimonic well-being at T2 (r = .12, p = .043). Meanwhile, gender was also significantly correlated with some measures of well-being, such as eudaimonic well-being at T1 (r = .16, p = .007), and flourishing at T1 (r = .13, p = .030) and T2 (r = .14, p = .011). After the six-week trial, we tested whether hot yoga improved the well-being of participants. Specifically, using the survey data collected at T1 and T2, multiple linear regression analyses were conducted to predict well-being at T2. To control for the possible confounding effects of age, gender, and well-being at T1, these variables were added into the linear regression models. As shown in Table 2, with the exception of flourishing, b = -0.43, p = .599, ΔR2 = .00, we found that practising hot yoga predicted higher levels of most well-being indicators at T2 as compared to the participants in the wait-list condition. These indicators included mindfulness, b = 1.76, p = .010, ΔR2 = .01, peace of mind, b = 0.23, p = .001, ΔR2 = .02, satisfaction with life, b = 0.35, p < .001, ΔR2 = .02, eudaimonic well-being, b = 0.09, p = .015, ΔR2 = .01, and general health, b = -0.28, p < .001, ΔR2 = .08. Almost consistent with Hypothesis 1, the results suggested that hot yoga practices led to an increase in most indicators of well-being, though the effect was small, as indicated by the effect size of R2 for the multiple regression (i.e., .0196, .13, and .26 for small, medium, and large effect sizes, respectively) (Cohen, 1988). Given that multiple outcomes might lead to the inflation of type-one errors, as a robustness check, we used the Bonferroni-corrected level of significance, α = .026, which takes into account the number of outcomes (i.e., 6) and their mean correlation (i.e., .43) (Uitenbroek, 1997). Even after correcting the results, all findings remained significant. Furthermore, all results remained substantially unchanged when the covariates of age and gender were excluded.
Next, we tested Hypothesis 2, whether hot yoga intervention would have a positive effect on momentary emotional experiences/hedonic well-being during the six-week trial through the ESM study. We analysed participants’ multiple time-point ESM data using multilevel modelling. Each participant had completed up to 168 momentary assessments, and we used this variable to model how their emotional experiences varied over time. Since we aimed to evaluate the results of the time analysis relative to the same time point for each participant, we centred time on the full sample mean (i.e., grand means centring). On the contrary, the variable of condition (i.e., hot yoga or wait-list control condition) on level-2 did not require centring, since it is a binary variable.
Table 3. Interaction of the Sequence of Time and Hot Yoga Condition on Positive and Negative Emotions in Multilevel Modelling

Note. 1Wait-list control = 0, hot yoga = 1. R2 is a conditional R2 which captures the proportion of overall variance explained by both fixed and random effects.*p < .05, ***p < .001.
As shown in Table 3, the interaction between the sequence of time and condition significantly predicted momentary positive emotional experiences, γ = .00, p = .042, but not negative emotional experiences, γ = .00, p = .756. The conditional R2, which captured the amount of variance explained by both fixed and random effects, was .68. Since the negative emotional experiences were not significant, we only looked at the outcome of momentary positive emotion in subsequent analyses. A simple slope test showed that the positive relationship between the sequence of time and positive emotional experiences was significant in the yoga condition, but not significant in the wait-list control condition (see Figure 2). Additionally, we tested whether the interaction between the sequence of time and the condition quadratically predicted positive emotional experiences to account for the non-linear impact of the sequence of time. Our results showed that positive emotional experiences were predicted by neither the sequence of time-squared alone, γ = .00, p = .515, nor the interaction between the sequence of time-squared and condition, γ = .00, p = .584. In short, Hypothesis 2 was partially supported, suggesting that positive emotions increased for average participants who joined the six-week hot yoga course, but not for those on the wait-list.

Note. Statistics are simple slope coefficient, standard error, t-value, and 95% confidence interval, respectively.
Figure 2. Sequence of Time for Each Condition (lines) Predicting Positive Emotional Experience.
To investigate the mechanisms behind the increase in momentary positive emotional experiences, we employed the ESM data for the undirected Hypothesis 3 to examine whether the effect of hot yoga on momentary positive emotional experiences would last for a certain period of time during the trial. Our aim was to determine whether the effect would fade out shortly, last until the next beep in the ESM study, or last until the next day after hot yoga practice. We tested whether being at the yoga premises (a yoga event), as reported by participants’ location at the time of the momentary survey, was associated with increased positive emotional experiences. Furthermore, we investigated whether this effect would sustain itself, bearing in mind that most yoga sessions were in the evening, and that the following survey would most likely be taken on the following day. We rearranged the ESM data such that the multilevel models included the variables of being at the yoga studio, the first subsequent momentary assessment, and the second subsequent momentary assessment.
As shown in Table 4, even after controlling for the effects of the sequence of time over the six weeks, being at the yoga studio significantly predicted momentary positive emotional experiences, γ = .15, p < .001. However, the effect did not sustain itself in the first subsequent momentary assessment, p = .140, nor in the second assessment, p = .996. The conditional R2 was .50. Basically, the undirected Hypothesis 3 was supported, suggesting that the effect of hot yoga on momentary positive emotional experiences lasted when being at the yoga studio, but not afterwards.
Table 4. Attending Studio Predicting Positive and Negative Emotions in Multilevel Modelling

Note. YogaEvent = attending studio at the current time; YogaEvent + 1-lag = attended studio at the previous time; YogaEvent + 2-lag = attended studio at two time points ago. R2 is a conditional R2 which captures the proportion of overall variance explained by both fixed and random effects.**p < .01, ***p < .001.
For Hypothesis 4, in order to investigate whether the effects of hot yoga intervention on the indicators of well-being would be mediated by momentary emotional experiences throughout the trial. To test this hypothesis, we looked into all well-being indicators in the T1 and T2 surveys, along with the ESM momentary emotion data, in the hot yoga condition. Since the momentary emotion data were at level-1, while the T1 and T2 well-being measures were at level-2, we conducted the 2-1-2 multilevel mediation analysis suggested by Preacher et al. (2011).
As shown in Table 5, we estimated the indirect effect for the path between a well-being indicator at T1 and the same well-being indicator at T2 through positive emotional experiences using the bootstrap analysis. For the path between T1 and T2 mindfulness, the indirect effect was significant, γ = .06, p = .029. The mediated effect contributed to 21% of the explained variance in the model. Similarly, for the path between T1 and T2 peace of mind, the indirect effect was significant, γ = .09, p = .09. The mediated effect contributed to 31% of the explained variance in the model. In terms of the path between T1 and T2 general health, the indirect effect was again significant, γ = .09, p = .009. The mediated effect contributed to 11% of the explained variance in the model. In contrast, the indirect effects were not significant for the paths between T1 and T2 satisfaction with life, γ = .04, p = .194, eudaimonic well-being, γ = .03, p = .129, and flourishing, γ = .61, p = .275.
Table 5. Results of Direct, a-path, b-path, and Indirect Effects Mediated by Positive Emotion

Note. MFT1 = mindfulness at Time 1; MFT2 = mindfulness at Time 2; PoMT1 = peace of mind at Time 1; PoMT2 = peace of mind at Time 2; GHT1 = general health at Time 1; GHT2 = general health at Time 2; SWLT1 = satisfaction with life at Time 1; SWLT2 = satisfaction with life at Time 2; EUWBT1 = eudaimonic well-being at Time 1; EUWBT2 = eudaimonic well-being at Time 2; FlsT1 = flourishing at Time 1; FlsT2 = flourishing at Time 2.* p < .05, ** p < .01, *** p < .001.
On the other hand, negative emotional experiences did not mediate any paths between T1 and T2 mindfulness, γ = .00, p = .994, peace of mind, γ = .04, p = .089, general health, γ = .02, p = .345, satisfaction of life, γ = .01, p = .543, eudaimonic well-being, γ = .02, p = .169, and flourishing, γ = .13, p = .672.
In sum, the results suggested that the relationships between T1 and T2 mindfulness, T1 and T2 peace of mind, and T1 and T2 general health could be explained by the increase in positive emotional experiences. There was no evidence for negative emotional experiences as a mediator. Because of multiple outcomes, we also checked the robustness by adjusting the level of significance (α) using Bonferroni correction. Taking into account the number of outcomes (i.e., 6) and their mean correlation (i.e., .43), the adjusted value of α was .026 (Uitenbroek, 1997). The indirect effects of positive emotional experiences on the two paths concerning T1 and T2 peace of mind and T1 and T2 general health were still significant, whilst that on the path concerning T1 and T2 mindfulness was marginally significant, suggesting that the effects remained basically unchanged. Therefore, the results partially supported Hypothesis 4.
Finally, we tested Hypothesis 5 to explore whether the indicators of baseline well-being would moderate the effects of hot yoga intervention on momentary positive emotional experiences. For our analysis, we used all well-being variables in the T1 survey from the hot yoga group as moderators, and momentary positive emotional experiences in the ESM data as the outcomes.
As shown in Table 6, we found that three T1 well-being indicators significantly interacted with the sequence of time to predict momentary positive emotional experiences in the hot yoga group: eudaimonic well-being, γ = -.00, p = .020, conditional R2 = .45, flourishing, γ = -.00, p = .004, conditional R2 = .61, and mental well-being, γ = -.00, p = .007, conditional R2 = .65. Meanwhile, all other T1 well-being indicators (i.e., mindfulness, peace of mind, general health, and satisfaction with life) did not yield significant results. Simple slope tests revealed that hot yoga led to a more significant increase in positive emotional experiences for people with lower levels of eudaimonic well-being, flourishing, or mental well-being, as compared to those with higher levels of well-being at T1 (see Figure 3).We also ran additional tests to rule out any possible ceiling effects. Relevant statistics were shown in Appendix C. In sum, Hypothesis 5 was partially supported.
Table 6. Moderation of Baseline Well-being for Predicting the Change of Positive Emotion during Yoga Intervention in Multilevel Modelling
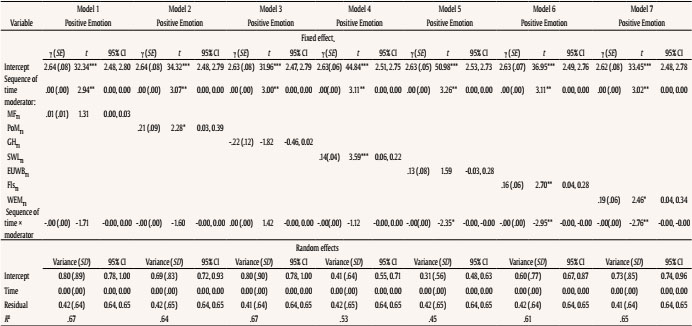
Note. MFT1 = mindfulness at Time 1; PoMT1 = peace of mind at Time 1; GHT1 = general health at Time 1; SWLT1 = satisfaction with life at Time 1; EUWBT1 = eudaimonic well-being at Time 1; FlsT1 = flourishing at Time 1; WEMT1 = Warwick-Edinburgh Mental Well-being at Time 1. R2 is a conditional R2 which captures the proportion of overall variance explained by both fixed and random effects.*p < .05, **p < .01, ***p < .001.

Discussion
Our research is probably the largest evaluation of the impact of yoga in general, and hot yoga in particular, on multifaceted well-being indicators so far. We conducted an RCT in 290 healthy adults who were assigned to either a six-week hot yoga group or a wait-list control group. Mostly consistent with previous studies on the effects of hot yoga on mindfulness and perceived stress (Hewett et al., 2011), and life satisfaction (Rissell et al., 2014), we found that hot yoga intervention enhanced various aspects of well-being including life satisfaction, general health, mindfulness, peace of mind, and eudaimonic well-being—except for flourishing—in an RCT with a relatively large sample size. This suggests that hot yoga is an effective enhancer of well-being.
Based on our research, there are similarities between the effects of hot yoga and other forms of yoga on well-being. For instance, our study demonstrated that hot yoga intervention had a significant effect on general health, in the same way that some previous studies reveal the significant effect of Hatha yoga on general health (Smith et al., 2007). Another example is that our hot yoga intervention led to a significant improvement of participants’ mindfulness, which is similar to Kripalu yoga—a specific form of Hatha yoga that has proven significant effects on mindfulness (Conboy et al., 2010). After our hot yoga intervention, the participants reported increased life satisfaction. Coincidentally, people practising Dru yoga shared the same effect (Hartfiel et al., 2011). We also discovered the effect of hot yoga on eudaimonic well-being, which resembles the significant association between general yoga experience and eudaimonic well-being (Ivtzan & Papantoniou, 2014). Having said that, there are differences between how hot yoga and other forms of yoga affect well-being. For instance, according to a study on Viniyoga, this specific form of Hatha yoga contributes to increased flourishing in participants (de Manincor et al., 2016). However, our hot yoga intervention did not bring the same benefit, suggesting that the empirical evidence has been far from conclusive.
Additionally, we assessed participants’ momentary emotions, allowing us to measure their moment-by-moment hedonic well-being. Previous research has suggested no effect from Iyengar yoga (Vogler et al., 2011), whilst a considerable number of past studies have shown the positive effects of a range of Hatha yoga (Conboy et al., 2010; Luu & Hall, 2017; Park et al., 2020) and hot yoga (Szabo et al., 2017) on affects and emotions. Nonetheless, little is known about whether hot yoga would lead to an increase in momentary emotional experiences. Using a combination of the ESM and experimental design, the present study also found that the hot yoga intervention was better at increasing momentary positive emotional experiences than the wait-list condition, thereby adding ecologically-valid and experimental data to the field.
Through the use of the ESM, another of our new finding is that being at the yoga studio significantly predicted an increase in positive emotional experiences. However, the effect did not hold in the first and second assessments that took place after the classes. Given our time frame setting (where no survey was likely to be conducted after an evening yoga class) and the survey response rate (2.3 out of four surveys per day), the subsequent assessments were most likely to take place on the day after the class. While our data imply that the effects of hot yoga are not sustained the following day, future research would benefit from shortening the assessment window to determine how long exactly the effects last during the day of practice. Although the emotional benefits were momentary, they remained consistent throughout the six-week duration without a detectable difference due to time. In other words, there was no habituation to this "positive boost" throughout the study.
Building on the aforementioned line of research on yoga practice and emotion, our mediation analysis further added that positive emotional experiences significantly mediated the relationships between baseline well-being and post-treatment well-being for mindfulness, peace of mind, and general health. This confirmed our initial hypothesis that positive emotional experiences associated with practising hot yoga could be a key underlying factor for post-treatment increases in well-being. Our results were also consistent with the "broaden and build" theory of positive emotions, which states that experiencing more positive than negative emotions broadens one’s awareness and encourages novel and exploratory thoughts and actions, thereby leading to resources for long-term well-being for individuals to flourish (Fredrickson, 2001). It is also worth discussing that the levels of positive emotional experiences may be associated with how much a participant liked each hot yoga class. Together with positive emotional experiences, the degree to which each yoga class was liked might also play a mediating role in the relationship between baseline well-being and post-treatment well-being. Unfortunately, we did not collect any data on the degree to which each class was liked.
Finally, we investigated whether baseline well-being affected the benefits of hot yoga intervention. Our results suggested this might be the case, as hot yoga participants with lower levels of flourishing, mental well-being, and eudaimonic well-being at the T1 stage (i.e., before starting classes) experienced a stronger boost in positive emotion during the six-week intervention. Our research has added valuable experience-sampling data to a group of studies that document people with lower levels of well-being, such as those who are depressed and stressed, gaining the most from practising yoga (e.g., Cramer et al., 2013; Szabo et al., 2017). Coupled with previous empirical evidence, our findings may provide insights into not only PPIs, but also the allocation of social resources to people most at risk of mental problems. Whilst practising yoga, and hot yoga in particular, is potentially beneficial to healthy adults (F. Wang & Szabo, 2020), it can also be a promising way to help vulnerable groups in society, such as people with mild psychological disorders or at risk of other mental problems. Mental illnesses cost the global economy at least $1 trillion in lost productivity annually, with depression being the leading risk factor (World Health Organization, 2017). By offering hot yoga intervention to people most at risk and boosting their well-being through hot yoga, we could alleviate some of the world’s burden at a reasonable cost. While future research could be directed at evaluating the cost-benefit ratio of various psychological interventions, our study suggests that hot yoga could be a good candidate.
Admittedly, there are some limitations to this study. Firstly, there is a lack of an active control group undertaking a different form of exercise. Engaging in hot yoga sessions up to four times per week constitutes a somewhat intensive physical exercise intervention. However, our study is unable to disentangle this from other potential elements and their synergy. Therefore, the heavy exercise component of the hot yoga classes cannot be overlooked as a potential driver of the observed benefits. Secondly, although we used the ESM design to investigate the momentary effects of hot yoga intervention, we did not look into whether they could be translated into longer-term effects, such as the effects after one month or even half a year. This would be highly desirable in future research (F. Wang & Szabo, 2020). Thirdly, although we recruited a community sample and used random assignment in our study design, it would be worth paying more attention to certain sample characteristics in future studies. For instance, female participants accounted for almost 80% of our sample, which might limit the applicability of our results to the general population. Furthermore, some national statistics in the US have reported that people with higher levels of educational attainment are more likely to engage in the use of complementary health approaches such as yoga (Clarke et al., 2015). Hence, we may have to include educational attainment in future research. Fourthly, the present study looked at only one specific type of yoga and has not addressed a number of variables, including the variety of yoga types (e.g., Hatha, Ashtanga, etc.), duration of classes (20 to 90 minutes), frequency of classes (daily, weekly), and lengths of yoga intervention (weeks, months) (Field, 2016). Fifthly, even though there were no significant differences in age and gender between the hot yoga group and the wait-list control group—suggesting that the random assignment was successful—the sample sizes of the hot yoga group (n = 137) and the wait-list control group (n = 153) could have been more equal. One possible reason for the gap was that we conducted the random assignment before the phone screening process. Future RCTs would benefit from conducting pre-screening prior to random assignment, to better equate groups on potential confounding variables.
Conclusion
The present study demonstrated a broad range of benefits from a six-week hot yoga intervention studied using an RCT. These benefits included the immediate boost of momentary hedonic well-being following the practice of hot yoga each time. This could potentially explain the observed increase in post-treatment well-being, especially in people that had the lowest baseline well-being. In summary, our research showed that hot yoga has the potential to be an effective PPI. As such, hot yoga would benefit from in-depth investigations in the future.



