










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Anorexia nervosa (AN) is a life-threatening eating disorder associated with a higher chronification risk and mortality rate in comparison to other eating disorders 1,2,3. Its association with high hospital admission rates, long hospital stays, increased health costs, and severe physical, psychological, and social sequelae makes it an important social and health problem. Up to two-thirds of patients with AN are admitted to hospital at least once during the course of their disease 3,4.
Available treatments have very low success rates; thus, one review reported relapse in around half of AN patients within the first year after inpatient treatment 5. Little information is available on factors that may be associated with a favorable response. Low body weight at hospital discharge has been related to higher relapse and readmission rates 6,7, but the achievement of weight gain during hospitalization poses a major challenge in patients with AN 5).
Clinical practice guidelines (CPGs) of the UK National Institute for Clinical Excellence (NICE, 2004; last revision in 2013), the American Psychiatric Association (APA, 2006; last revision in 2012), and the Spanish Ministry of Health and Consumption (SMHC, 2009) 8,9,10 provide evidence-based recommendations on the approach to patients with eating disorders. According to these CPGs, patients with AN require a multidisciplinary approach that includes dietary-nutritional and psychological therapies.
The therapeutic objective of nutritional support (NS) in hospitalized AN patients is to recover a healthy minimum weight, correcting the physical and psychological sequelae of malnutrition. An improvement in nutritional status has been found to enhance the cognitive status of these patients, increasing the effectiveness of psychological therapies 8,9,10,11,12.
Natural feeding should be the first option for NS, because it favors psychosocial abilities and behaviors that are hindered by artificial feeding. However, the diet can be supplemented with artificial nutrition, preferably enteral, in patients with a long history of early satiety, inadequate weight recovery, or severe malnutrition, or in those who will not cooperate with food intake 8,9,10,11,12. Thus, it has been reported that hypercaloric supplements are useful to recover weight and reduce hospital stays 12,13,14,15. Furthermore, multivitamin and mineral oral supplements (mainly phosphorus, potassium, and magnesium) have been used to prevent refeeding syndrome and treat nutritional deficiencies in highly malnourished patients 8,9,10,11,12, while zinc supplementation was reported to be effective for weight recovery in patients with AN 16,17.
We hypothesized that adherence of NS prescriptions to CPG recommendations for eating disorders would improve health outcomes and reduce costs. Few published data are available on the adherence to recommendations of NS prescriptions for patients with AN and its influence on long-term effectiveness and safety outcomes. With this background, the objectives of this study were to analyze the adherence of NS prescriptions for hospitalized AN patients to recommendations in APA, NICE, and SMHC CPGs and to compare the effectiveness, safety, and costs of NS as a function of CPG adherence.
MATERIALS AND METHODS
STUDY DESIGN AND POPULATION
This retrospective observational study included patients with AN admitted to a ten-bed in-patient Eating Disorders Unit (EDU) in a general university hospital between January 2006 and December 2009 and followed until December 2014. This unit is a nationally recognized specialist center for adolescents and adults with severe eating disorders.
Inclusion criteria were: age ≥ 12 years; weight < 85% ideal weight, i.e., body mass index (BMI) ≤ 17.5 kg/m2 according to the 10th edition of the International Classification of Diseases (ICD-10, WHO, 1992), and fulfillment of all diagnostic criteria for AN (restrictive [R-AN] and purging [P-AN] subtypes) according to the American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV-TR) 18,19. Exclusion criteria were: principle diagnosis of bulimia nervosa, eating disorder not otherwise specified (EDNOS), or psychiatric disease other than eating disorder; and the receipt of therapy at other centers.
VARIABLES
Sociodemographic, clinical, anthropometric and therapeutic variables
Data were gathered from clinical records of the patients on sociodemographic variables (sex, age at admission, history of suicidal and/or self-harm behavior, consumption of toxic substances, consumption of psychopharmaceuticals, number of previous hospitalizations, and number of previous treatments for AN), clinical variables (R-AN or P-AN subtype, time with AN ["long" = ≥ 7 yrs], and physical and psychiatric comorbidities), and anthropometric variables (body weight [kg] and BMI [kg/ m2] at hospital admission and discharge, and minimum BMI [kg/ m2] reached during the course of their AN). Time with AN was defined as the interval (in years) between the diagnosis and first EDU admission.
Body weight was measured every morning after voiding, with patients in hospital gown and bare feet. Height was measured at admission. The BMI was calculated as weight (kg) divided by the square of height (m).
Plasma electrolytes, glucose levels, and deficiencies were closely monitored during the hospital stay.
NS prescriptions from psychiatrists during all hospital stays were gathered from the electronic prescription program for hospitalized patients (ATHOS-Prisma®). NS-related study variables were: type of artificial feeding (natural feeding [ordinary food] alone, supplementation with artificial nutrition, or solely artificial nutrition); intake cooperation (forced/unforced); administration route (enteral/parenteral); nasogastric feeding (yes/no) and administration (continuous [> 24 h] or discontinuous [3-5 bolus feedings/day]); types of enteral nutrition formula; vitamin and mineral supplements; maximum caloric supply (Kcal/day); dosage (mg/day, mEq/day, or IU/day) and duration (days) of NS; and reason(s) for NS prescription.
Adherence of NS prescription to CPGs
CPGs adherence was defined as the fulfillment of all recommendations, considering the "degree of adherence" as the percentage of hospitalizations with NS prescriptions that followed all recommendations. Table I compiles the nutritional recommendations of APA (2006) and NICE (2004)/SMHC (2009) for patients with AN, and the reasons for non-adherence to CPG recommendations; SMHC recommendations are the same as those in NICE guidelines.
Table I. Nutritional recommendations for patients with anorexia nervosa during weight recovery, and reasons for non-adherence of nutritional support prescriptions to recommendations

AN: anorexia nervosa.
*Considered as BMI ≤ 15 kg/m² (maximum level of severity according to the WHO categories for thinness in adults).
Variables related to NS effectiveness, safety, and cost
Evaluation of NS effectiveness considered the body weight (kg) and BMI (kg/m2) at discharge, weight gain rate (total weight gain in grams during hospitalization divided by days of hospitalization), hospital stay (number of days from admission to discharge), time to relapse (months between hospital discharge and next admission), body weight maintenance (yes/no), and number of EDU readmissions during 12 months post-discharge. Data on hospital stay and EDU admissions were furnished by the clinical documentation department of the hospital. Safety was evaluated according to the number and type of NS-related adverse effects. The NS cost (in euros) was the sum of direct costs for enteral nutrition formulas and vitamin and mineral supplements prescribed during hospital stays, extracted from the Pharmacy Department economic management program (ATHOS-Stock®).
STATISTICAL ANALYSIS
IBM-SPSS V.21.0 was used for the statistical analysis. Quantitative variables were expressed as central tendency and dispersion measures and qualitative variables as absolute and relative frequencies. Proportions among groups were confirmed by bivariate analysis with Pearson's Chi-square test or, when conditions were not met, with Fisher's exact test. Quantitative variables were compared between independent groups with the Student's t-test or, when the distribution was non-normal, the Mann-Whitney U test. The normality of variables was verified using the Shapiro-Wilks test. Survival was analyzed using the Kaplan-Meier test, comparing survival between groups with the Log Rank test (Mantel-Cox). p < 0.05 was considered as significant in all tests.
RESULTS
SOCIODEMOGRAPHIC, CLINICAL, ANTHROPOMETRIC AND THERAPEUTIC CHARACTERISTICS
During the study period, 128 patients were hospitalized in the EDU; 56 were excluded for: bulimia nervosa (n = 21), EDNOS (n = 20), principle diagnosis of psychiatric disease other than an eating disorder (n = 3), and continued receipt of therapy at other centers (n = 12).
The study finally included 72 patients with R-AN (n = 45) or P-AN (n = 27). Table II lists their characteristics at baseline. All patients had malnutrition-related physical comorbidities, including endocrine (93.1%), hydroelectrolytic (70.8%), hematologic (63.9%), hepatic (41.7%), gastrointestinal (33.3%), cardiovascular (25.0%), bone (31.9%), and renal (12.5%) disorders. No significant differences in physical comorbidities were found between subtypes. The presence of psychiatric comorbidities was observed in 56.9% of the patients, including substance-related (30.6%), personality (22.2%), anxiety (16.7%), and mood (12.5%) disorders. Substance-related disorders were more frequent (p =0.048) in patients with P-AN (44.4%) versus R-AN (22.2%).
Table II. Sociodemographic, clinical and anthropometric characteristics in 72 patientswith anorexia nervosa at first admission in the EDU
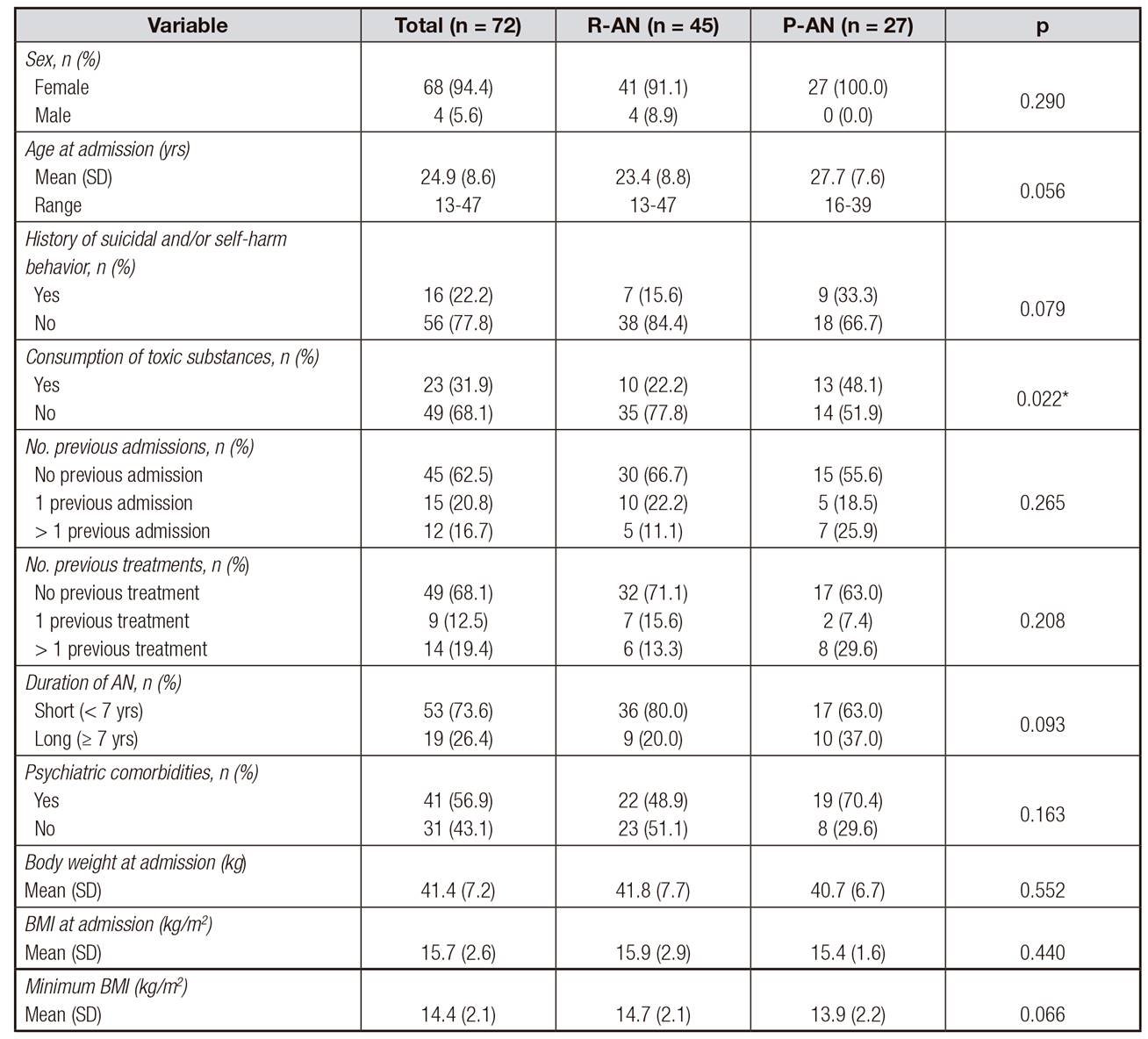
BMI: body mass index; EDU: eating disorders Unit; P-AN: purging anorexia nervosa; R-AN: restrictive anorexia nervosa; SD: standard deviation.
*Statistical significance (p < 0.05).
Almost half of the patients (47.2%) were admitted to EDU more than once (range: 1-15 admissions/patient); 177 hospitalizations were analyzed (112 for R-AN and 65 for P-AN), and the BMI at admission was ≤ 15 kg/m2 in 37.3% of these. Psychopharmaceuticals were prescribed in 71.8% of the 177 hospitalizations, finding no significant difference (p = 0.637) between R-AN (70.5%) and P-AN (73.8%) patients. Feeding was exclusively natural in 50.8% of hospitalizations, supplemented with artificial nutrition in 46.3%, and completely replaced with artificial nutrition in 2.8%. Feeding was forced in 5.6% of hospitalizations (6.3% R-AN vs 4.6% P-AN, p = 0.748), parenteral nutrition was used in 1.7% (0.9% R-AN and 3.1% P-AN, p = 0.226) and nasogastric enteral feeding in 5.1% (6.3% R-AN and 3.1% P-AN, p = 0.489), being continuous (24-h) in 44.4% of cases.
In 49.2% of hospitalizations, complete liquid enteral nutrition formulas were prescribed due to "lack of cooperation with oral intake" (44.8%), "insufficient weight recovery" (31.1%), or "life-threatening BMI" (≤ 12 kg/m2) (24.1%). The mean maximum caloric supply via enteral nutrition was 716.9 Kcal/day (range: 100-2,100 Kcal/day), and the mean time with enteral nutrition was 41.8 days (range: 12-165 days); 93.1% of the formulas prescribed were standard, polymeric, hypercaloric (1.5 Kcal/ml), and fiber-free. The macronutrient composition of the total caloric supply was 15-17% proteins, 49-55% carbohydrates and 30-35% lipids.
Oral vitamin supplements were prescribed in 23.7% of hospitalizations. Out of the 66 prescriptions for these supplements, 36.4% were for multivitamins, 31.8% for vitamin D3, 25.8% for vitamins B1-B6-B12, 4.5% for vitamin B1, and 1.5% for vitamin B6. The mean duration of vitamin consumption was 50.9 days (range: 12-174 days). Drops of vitamin D3 (66.7 IU/drop) were administered (400-800 IU/day) to prevent and/or treat osteoporosis from the lack of dietary vitamin D intake and/or sunlight exposure. Supplementation with multivitamin pills (2,500-3,600 IU vitamin A, 1.6-15 mg vitamin B1, 1.8-15 mg vitamin B2, 2.6-10 mg vitamin B6, 4-10 μg vitamin B12, 100-200 mg vitamin C, 400-500 IU vitamin D3, 15 IU vitamin E, 10-25 mg calcium pantothenate, 0.2 mg biotin, 19-50 mg nicotinamide, and 0.4-0.8 mg folic-acid per pill) or with 250-300 mg vitamin B1, 250-300 mg vitamin B6, and/or 0.5 mg vitamin B12 pills was used to prevent refeeding syndrome and treat vitamin deficiencies. Vitamins were administered once daily throughout the refeeding period. Mineral supplements were prescribed in 26.6% of hospitalizations. Out of the 65 prescriptions for these supplements, 44.6% were for calcium, 38.5% for potassium, 9.2% for phosphate, and 7.7% for magnesium. Calcium supplementation (500-1,500 mg/day) used lactogluconate/calcium carbonate pills (500 mg calcium/pill) to prevent and/or treat osteoporosis; potassium supplementation (20-80 mEq/day) used 600 mg potassium chloride capsules (8 mEq potassium/capsule) and/or injections of 1,491 mg potassium chloride (20 mEq potassium/injection); phosphate supplementation (800-1,000 mg/day) used monobasic sodium phosphate sachets (800 mg phosphate/sachet), and magnesium supplementation (53-212 mg magnesium/day) used pills of 7.17 mg magnesium bromide, 0.34 mg magnesium fluoride, and 125.06 mg magnesium hydroxide.
Minerals were included in the composition of 83.3% of multivitamin pills (61.8-125 mg calcium, 15.6-60 mg iron, 38.9-100 mg magnesium, 0.5-1 mg manganese, 1 mg copper, and 30-125 mg phosphorus per pill). In 11.3% of hospital stays, zinc was supplemented by the daily administration of a single multivitamin pill with 20.6 mg zinc sulfate (7.5 mg zinc elemental).
Oral supplements with multivitamins, potassium, phosphorus, and/or magnesium were prescribed in 43.9% of the 66 hospitalizations with admission BMI ≤ 15 kg/m2 in order to prevent refeeding syndrome.
ADHERENCE OF NS PRESCRIPTIONS TO CPGS
NS prescriptions followed all APA recommendations in 18 (10.2%) hospitalizations and all NICE/SMHC recommendations in 130 (73.4%). Among hospitalizations for R-AN (n = 112), 9.8% adhered to APA and 73.2% to NICE/SMHC CPGs. Among hospitalizations for P-AN (n = 65), 10.8% adhered to APA and 73.8% to NICE/SMHC CPGs. Table III exhibits the adherence to CPGs as a function of sociodemographic, clinical, and anthropometric variables. Causes of "non-adherence" in the 159 hospitalizations that did not meet APA recommendations were "non-supplementation with zinc" (98.7%), "non-supplementation with phosphorus, potassium, and/or magnesium" in patients with BMI ≤ 15 kg/ m2 (23.3%), "discontinuous administration" of nasogastric enteral feeding (3.1%), and "parenteral nutrition" (1.9%). Causes of "non-adherence" in the 47 hospitalizations that did not meet NICE/SMHC recommendations were "non-supplementation with multivitamins and/or minerals" in patients with BMI ≤ 15 kg/m2 (78.7%), "force-feeding" (21.3%), and "parenteral nutrition" (6.4%).
Table III. Distribution of adherence of hospitalizations (n = 177) as a function of sociodemographic, clinical and anthropometric variables

APA: American Psychiatric Association; AN: anorexia nervosa; BMI: body mass index; NICE: National Institute for Clinical Excellence; SD: standard deviation; SMHC: Spanish Ministry of Health and Consumption.
*Statistical significance (p < 0.05).
NS EFFECTIVENESS, SAFETY AND COST AS A FUNCTION OF ADHERENCE TO CPGS
Table IV compares the effectiveness, safety, and cost of NS in patients with AN between the adherence and non-adherence of prescriptions to the CPGs. After correcting for the longer hospital stay of the patients receiving nutritional supplements, the weight gain rate was significantly higher in patients receiving zinc supplementation (Table V). A total of 65 adverse effects of the NS were recorded in 28.9% of hospitalizations, including dyspepsia (30.8%), flatulence (29.2%), abdominal distension (18.5%), abdominal pain (12.3%), nausea (4.6%), regurgitation (3.1%), and vomiting (1.5%), which were all attributed to the enteral nutrition formulas. Before the initiation of NS, hypopotassemia was observed in 10.2% of hospitalizations, hypophosphatemia in 1.7%, and hypomagnesemia in 1.2%. During NS treatment, plasma levels of these electrolytes were normal. No symptoms of refeeding syndrome (e.g., cardiac arrest, rhabdomyolysis or encephalopathy) were recorded.
Table IV. Treatment effectiveness, safety and cost in patients with anorexia nervosa

BMI: body mass index; IQR: interquartile range; NS: nutritional support; SD: standard deviation.
*Statistical significance (p < 0.05).

DISCUSSION
NS prescriptions for these hospitalized AN patients showed a low degree of adherence to APA recommendations. Force-feeding by nasogastric tube was more frequent than parenteral nutrition, considered as a last resort, although nasogastric feeding was more often discontinuous than continuous, while the main cause of "non-adherence" was "non-supplementation with zinc". Supplementation with phosphorus, potassium, and/or magnesium was not always offered to severely malnourished patients during the first few days of NS treatment. NS prescriptions showed a higher degree of adherence to NICE/SMHC recommendations, largely attributable to the scant utilization of force-feeding and parenteral nutrition, while the main cause of "non-adherence" was non-supplementation with multivitamins and/or minerals for severely malnourished patients.
Among reported prognostic factors for AN chronification (age at admission, history of suicidal/self-harm behavior, consumption of toxic substances, number of treatments and hospitalizations, ≥ 7 yrs with AN, psychiatric comorbidities, and low body weight/BMI) 1,20,21, the only statistically significant differences as a function of CPG adherence were the lower body weight and BMI at admission and the lower minimum BMI reached during the course of their AN in the NICE/SMHC non-adherence versus adherence group. This apparently greater severity of illness in the NICE/SMHC "non-adherence" group may have increased the frequency of force-feeding and parenteral nutrition in life-threatening situations.
Body weight and BMI at discharge were significantly lower in hospitalizations with "adherence" versus "non-adherence" to APA. After correcting for longer hospital stay in the "APA adherence" group, a significantly higher weight gain rate was obtained in the latter in comparison to the "non-adherence" group, which may be attributable to the zinc supplementation. Daily supplementation with 7.5 mg elemental zinc increased the weight gain rate in these AN patients. This finding is consistent with two randomized, double blind, placebo-controlled clinical trials 16,17 in which anorexic patients receiving 28 mg or 50 mg elemental zinc daily showed higher weight gain and improved anxiety and depression symptoms. Zinc is present in large amounts in brain areas involved in food intake, body weight control, and serotonin metabolism, and zinc deficiencies and serotonergic activity disorders are frequent in anorexic patients 17. However, the prescription of zinc supplementation to hospitalized patients with AN was infrequent in the present study.
No statistically significant differences were found in body weight or BMI at discharge or in weight gain rate during hospitalization between NICE/SMHC adherence and non-adherence, likely attributable to the more severe malnutrition at admission in the (non-adherence) group. Hospital stay was significantly shorter in the NICE/SMHC "adherence" versus non-adherence group, which may be explained by the superior nutritional status of the former at admission. Accordingly, force-feeding and parenteral nutrition do not appear to favor weight gain or reduce the hospital stay in hospitalized patients with AN. There have been reports that a greater caloric intake and weight gain are obtained by force-feeding these patients with a nasogastric tube in comparison to oral feeding, although these benefits are not maintained over the long term 13,22,23,24,25. Moreover, force-feeding may damage the relationship between patients and healthcare professionals and has been criticized on ethical grounds 12.
CPGs recommend multivitamin and mineral supplementation in severely malnourished AN patients. According to the present results, this supplementation does not appear to increase the weight gain rate in hospitalized AN patients, likely due to the greater severity of illness (lower body weight and BMI) at admission of the patients who received it. A double-blind controlled clinical trial with placebo also found that vitamin and mineral supplementation was not useful for weight gain in anorexic patients and did not enhance the effects of pharmacological treatment 26. However, the administration of multivitamins with zinc proved to be the only NS component that significantly increased the weight gain rate in the present patients.
Most enteral nutrition formulas were hypercaloric, the type most frequently indicated in AN to reduce gastric distension and hydric overload during refeeding 27. However, fiber-enriched formulas were not routinely administered, despite the benefits of fiber for these frequently constipated patients 27. Administration of enteral nutrition formulas had no effect on weight gain and was associated with longer hospital stays, likely due to the higher malnutrition severity at admission of those treated with enteral nutrition. These findings support the proposal that exclusively natural feeding should be the first option for NS in AN patients 12,27. It was reported that enteral nutrition formulas do not yield major benefits and may possibly reinforce avoidance behavior towards normal food 12, although other researchers observed increased weight gain and reduced hospital stay with the administration of hypercaloric formulas 13,14,15,23,28.
Over the longer term, relapse was observed within 12 months post-discharge after 54.2% of hospitalizations, similar to previous observations 5, and most of the patients failed to maintain their body weight during this follow-up period. Nova et al. described a tendency for anorexic patients to reduce food intake after hospital discharge due to dissatisfaction with their body image, returning to their pre-admission size 29. In the present study, CPG adherence did not appear to contribute to weight maintenance or reduce the time to relapse or readmission rate.
NS-related adverse effects were mild and infrequent, and vitamin and mineral supplements were better tolerated than enteral nutrition formulas. No refeeding syndrome was observed in any hospitalizations. The risk of refeeding syndrome increases with parenteral nutrition, but this was very rarely utilized 8,9,10,22. The incidence of adverse effects appears to be higher for NS prescriptions that adhere to APA versus NICE/SMHC guidelines. This may be because the former support nasogastric tube feeding in patients who do not acknowledge their disease, refuse oral intake, or feel guilty when eating 9. Force-feeding with nasogastric tube has been associated with more frequent adverse effects in anorexic patients 24.
NICE/SMHC adherence was associated with a significant reduction in NS-related costs, mainly due to the shorter hospital stay. Enteral nutrition formulas were more frequently administered to patients with a greater degree of malnutrition at admission, who represented a higher proportion of the NICE/SMHC "non-adherence" than "adherence" group, increasing costs in the former.
One strength of this study was the setting of an EDU in which an AN-specific multimodal treatment program is provided; these patients are frequently admitted to general or psychiatric hospitals, in which multiple factors can influence treatment effectiveness. Study limitations include its retrospective design and the lack of randomization. Moreover, clinical records were used as the main source of information, and possible under-recording cannot be ruled out.
CONCLUSIONS
NS prescriptions for anorexic patients showed a higher degree of adherence to NICE/SMHC than APA recommendations. APA adherence was associated with improved weight gain during hospitalization but only over the short term. Patients whose NS prescriptions followed all NICE/SMHC recommendations had shorter hospital stay and reduced costs, likely due to their more favorable nutritional status at admission.

