










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Behavioral problems (aggressiveness, rebellion, social and emotional problems, disobedience) in childhood, preadolescence and adolescence are a main concern for families (Montiel-Nava, Montiel-Barbero & Peña, 2005; Robles & Romero Triñanes, 2011) to the extent that, according to an epidemiological study conducted with a sample of 1,220 parents, 59.6% believed that their children have such behavioral problems and 52% believed they needed psychological help to solve the indicated problems (Cantero-García & Alonso-Tapia, 2017). The way in which parents face such problems affects not only children’s behavior, but also parents’ psychological well-being (Luengo, 2014; Pérez, Menéndez & Hidalgo, 2014). The management of these behavioral problems can sometimes become a stressful life situation, an adverse situation, so that families can sometimes demand help to deal with this type of situations. These situations can come from sudden events or major crises that the family is going through, but also from more normative and expected situations, such as the vital transition that represents the arrival of children in preadolescence and adolescence. (Rodríguez, Martín & Rodrigo, 2015).
Faced with these situations, the most normal thing is that levels of resilience, as well as parents’ emotional well-being are affected. The origin of the concept of resilience goes back to investigations such as Rutter (1987), in which he argues that in the face of a difficult situation it is important to reduce the perception of threat as this can lead to a maladaptive coping. In addition, this author emphasizes that it is important to make sense of experiences and therefore neutralize those that are negative. However, improving the environment or eliminating adversities does not necessarily make people more resilient since the mere elimination of stressful situations does not help them to deal with them properly. In spite of the numerous investigations that have been carried out on the topic during the last decades, it continues existing problems of conceptualization and methodological problems in relation to this term (e.g., Luthar, Cicchetti & Becker, 2000). This has resulted on a proliferation of definitions (Windle, 2011). Among them we highlight the definition of Luthar (2006), the author who considers that resilience is positive adaptation or recovery from adverse situations or experiences, and this implies the two elements: 1) significant threat and 2) positive adaptation. Other authors consider that the resilience is the stable balance in the behavior before a traumatic event without affecting the performance and the daily life (Skinner & Zimmer- Gembeck, 2007). More recently, Windle (2011) defines resilience as the process of negotiation, management and adaptation to significant sources of stress or trauma, a process in which the individuals’ resources, their lives and their environment facilitate this ability to adapt and recover from adversity. In addition, this author points out that resilience is not a static feature, but on the contrary, resilience is a dynamic process that varies throughout the life cycle, depending on the areas and situations. In the same line, Alonso-Tapia, Nieto and Ruiz (2013) define resilience as positive adaptation or recovery in potentially adverse situations that have a high risk of generating a mismatch of the person. As can be seen, differences between cited authors are more in form than in substance, since they all highlight the two elements cited by Luthar. For this reason, in this study we will assume the definition proposed by Luthar (2006) and Leipold and Greve (2009).
Regarding the evaluation of resilience, there are numerous instruments developed (Windle, Bennet and Noyes, 2011) since the amalgama of definitions has given rise to multiple scales. Some of these scales measure factors that are associated with resilience (eg, CD-RISC) but are not resilience assessment scales per se, that is, most scales do not have both elements present (adversity and positive adaptation) proposed by Luthar (2006). Similarly, there is no scale that allows us to assess the resilience of parents who face an adverse situation such as the behavioral problems of their children. Although there are some scales specifically designed for parents (Martín, Cabrera, León & Rodrigo, 2013), they have not taken into account resilience’s two essential elements.
Exceptionally, according to the review carried out by Windle et al. (2011) the only scale that measures both elements (adversity and positive adaptation) is the BRS (Smith et al., 2008). For this reason, this scale has been translated into many languages, including German. (Leontjevas de Beek, Lataster, & Jacobs, 2014), Spanish (Rodríguez-Rey, Alonso-Tapia & Hernansaiz-Garrido, 2016), and Malay (Amat, Subhan, Jaafar, Mahmud, & Johari, 2014). In addition, it has been validated in populations with different health problems (rehabilitation of patients with heart problems, women with fibromyalgia), or populations that have experienced stressful life situations (Hernansaiz-Garrido, Rodríguez-Rey, Alonso-Tapia, Ruiz-Díaz & Nieto-Vizcaíno, 2014) (parents of children with cancer problems, parents of hospitalized children for long duration). In all cases presented in this study, the scale has had good psychometric properties, as well as good results in terms of its validity and reliability. However, the BRS measures resilience in general and, as we have said, resilience varies depending on the type of problem. That is why the objective of this study is to develop, from the BRS (Smith, 2008), a scale of resilience to the problems of behavior of children, as well as to study its factorial validity, its reliability and its convergent validity.
Method
Participants
615 parents participated, of whom 116 were men and 499 were women. The age of the sample ranged from 27 to 69 (M = 44.1, SD = 5.77). Regarding the educational level, 422 had completed university studies and 193 had completed primary, secondary, high school or FP education. Participants had between 1 and 4 children (M = 2, SD = .70) aged from 6 to 16 years old (M = 9.8, SD = 3.66).
Instruments
Brief Resilience Scale against Behavior Problems (BRS-PC). This questionnaire was designed for the present study. First, the items were adapted independently of the specific context to which the study refers. Next, an interjudge agreement was made. Subsequently, the instrument was reviewed by two members of the research team. This scale includes 6 items that measure resilience to the behavior problems of children. They are parallel to those of the Brief Resilience Scale (BRS,Smith et al., 2008), three formulated positively and three negatively. Examples of these are: "Even though I go through difficult situations due to my son's misbehavior, I get along relatively well" and "I have a hard time when I have to face stressful situations related to my son's bad behavior (disobedience, aggressiveness…"). They are answered on a Likert scale indicating the degree of agreement from 1 (totally disagree) to 5 (totally agree)
Brief Resilience Scale (BRS; Smith et al., 2008). This scale includes 6 items formulated both positively and negatively, which are answered on a Likert scale, indicating the degree of agreement from 1 (totally disagree) to 5 (totally agree). In this study, the Spanish version of Rodríguez-Rey, Alonso-Tapia and Hernansaiz-Garrido (2016) was used. The reliability in the original Spanish sample was α = .83, and of .80 in the sample of this study.
Procedure
The study was approved by the Ethics Committee of the Autonomous University of Madrid. Families from all over Spain were contacted through educational centers and parents' associations, they were informed of the research objectives and their collaboration was requested. A link with the questionnaire was sent to parents who agreed to participate, along with the informed consent and the instructions to respond. Both questionnaires were carried out anonymously.
Data-Analyses
To study the structural validity of the scale, the total sample was randomly divided into two subsamples (n 1 = 300, n 2 = 315), one for the initial analysis of the scale and the other for the cross validation analysis. In the initial analysis, a confirmatory factor analysis was performed with the first subsample. The structure put to the test was the same as that established in the BRS validation article in Spanish (Rodríguez-Rey, Alonso-Tapia & Hernansaiz-Garrido, 2016, see Figure 1). As an estimation method maximum likelihood was used and the criteria described by Hu & Bentler (1999) were adopted to accept or reject the model based on its adjustment (χ2 / gl <3; GFI, IFI and CFI> .95; RMSA <.06; SRMR <.08). After the initial analysis, the cross-validation analysis was performed using the first and second sub-samples, with the same estimation method and the same acceptance criteria. In this second analysis, it was verified whether the adjustment of the proposed model was equivalent in the two subsamples.

Once the structure of the scale was found, the reliability of the scale was analyzed using the Cronbach index and its convergent validity was tested by calculating the correlation between the scores on that scale and the scores on the original BRS.
The analyzes were performed using AMOS 23 and SPSS 23.
Results
Confirmatory factorial analyses
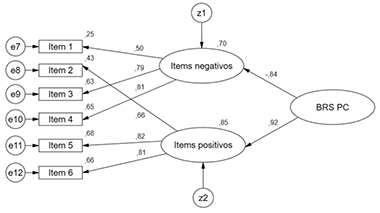
Figure 2 shows the factorial structure of the questionnaire obtained with the first random subsample (n 1 = 300). As it is observed, high proportions of variance of the items were explained and in turn these had high factorial weights in the first order factors (which collect, respectively, the positive and negative items of the questionnaire) and in the second order factor, which represents resilience in the face of behavior problems of children. Regarding the adjustment of the model, the χ2 statistic and the other adjustment indices were within the limits of acceptance, which indicates that the model adjusted adequately to the data (χ2 / gl = 1.59, TLI = .99; CFI =. 99, RMSEA = .04, SRMR = .02).

Cross-Validation
The cross-validation analysis was performed using the two random sub-samples (n1 = 300; n2 = 315). The χ2 statistc, the ratio χ2/gl and all the remaining adjustment índices are well inside the limits that allowed the model to be accepted (χ2/gl = 2.07; TLI = .98; CFI = .98; RMSEA = .04; SRMR = .04). The comparison of the groups showed that the adjustment indices do not decrease significantly when comparing models if restrictions are imposed for the acceptance of the equality of the results of the two samples in measurement weights ((χ2 = .46, p = .98), structural weights ((χ2= 1.20, p = .95), structural covariances ((χ2 = 4.16, p = .66), structural waste ((χ2 = 5.24, p = .63) and waste measurement ((χ2 = 18.24, p = .15). All this indicates that there are no differences in the fit of the model in both samples, so it can be considered that it is well estimated.
Reliability
The internal consistency of the scale was evaluated by Cronbach's α, obtaining a value of α = .84, indicative of good reliability.
Convergent Validity
A correlation analysis was performed between the original BRS scores and the developed scale of resilience versus behavioral problems. The correlation obtained was (r =.80, p < .001), indicating the existence of evidence of convergent validity of the developed scale with a similar one.
Discussion
The objective of this study was to develop a specific resilience questionnaire for a population subjected to specific stressors such as children’s behavioral problems.
Results obtained indicate, first, that the scale has a good structural validity, as indicated by the confirmatory factor analysis and the cross validation analysis. It has also shown good reliability and good convergent validity. These results are comparable to those found by other studies, which have also found the same factorial structure, comparable levels of reliability and good convergence (Rodríguez et al., 2016; Leontjevas, et al., 2014 & Amat, et al., 2014). This indicates that the scale developed is a valid and reliable instrument to measure resilience children’s problems of behavior. That is, the BRS-PC, is a scale that allows us the possibility of observing changes in the levels of resilience of parents to behavioral problems, considering that it is a very novel element and necessary at present for work with families.
This study has certain limitations that deserve attention. First, parents’ decision concerning the participation in the study may have resulted into that only those who were motivated have participated in the study. A second limitation has to do with the fact that in this study the behavioral problems have been understood in a very general way, understanding behavioral problems as those behaviors that pose a difficult challenge for parents to face. A third limitation has to do with the wide range of children's ages. In the face of future research, it would be necessary to measure the resilience in parents of children with a specific behavioral disorder such as ADHD, the conduct disorder, or the the oppositional defiant disorder, as well as to limit the age of the children depending on the different evolutionary stages. A fourth limitation has to do with the fact that only one of the members of the couple has filled in the questionnaire, and as we can see most of the people who answered the questionnaire were mothers. These limitations should be addressed in future investigations. The results obtained have theoretical implications, as well as implications for the evaluation and intervention. Regarding the former, although researchers have developed previously instruments that allow us to know the levels of resilience to certain specific problems (HIV, parents of children oncology, people who face stressful life situations; e.g., Hernansaiz-Garrido, et al., 2014), there was no instrument that allowed evaluating parental resilience in the face of specific stressors such as the management of children's behavior. Our study has provided such an instrument, which has been shown to be valid for measuring the resilience of parents who have children with behavioral problems.
Regarding the implications for evaluation and intervention, the fact of having instruments that allow us to know the perception that parents have about their levels of resilience is positive because it allows us to obtain information about parents, which can be valuable diagnosis that will also help guide a future intervention based on the needs they raise. The developed scale allows us to evaluate where we started from, an aspect that will serve to guide the intervention. Working with parents on basic aspects such as their level of resilience and emotional well-being are aspects that will contribute to improving the psychological well-being of parents, as well as improving the family climate. On the other hand, working on the promotion of effective educational guidelines, which help to exercise their parental role in an appropriate manner, can contribute significantly to improving the emotional well-being of parents and their resilience. Through the improvement of psychological well-being and parental resilience, as well as the family climate, it can contribute to the improvement of children's behavior problems.

