










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.102 n.6 Madrid Jun. 2010
PICTURES IN DIGESTIVE PATHOLOGY
Clipping of a post-sphincterotomy bleeding
Tratamiento con clip del sangrado post-esfinterotomía
J. Espinel1, E. Pinedo2 y C. Bailador3
Servicio de 1Aparato Digestivo y de 2Radiodiagnóstico. Hospital de León.
3Servicio de Aparato Digestivo. Hospital Virgen de la Concha. Zamora
Case report
An 88-year-old female with a previous history of retinopathy requiring treatment with Adiro® (acetylsalicylic acid) presented with jaundice, pruritus and right upper quadrant pain. An abdominal ultrasound revealed multiple stones in the common bile duct (CBD). Adiro® was stopped five days before ERCP. ERCP confirmed the presence of multiple stones in the CBD, which were extracted after performing a sphincterotomy. Four days later the patient presented with melena and anemia (hemoglobin of 8.9 g/dL).
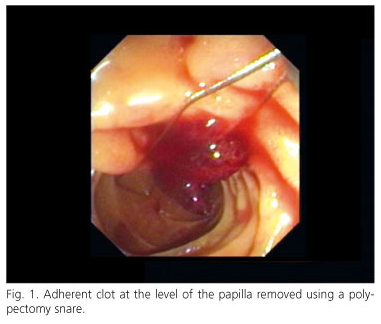
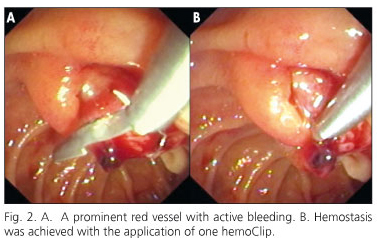
Post-sphincterotomy bleeding was suspected. A new ERCP revealed an adherent clot at the level of the papilla with active oozing bleeding. After the clot was removed using a polypectomy snare (Fig. 1) a prominent red vessel with active bleeding was seen underneath. Hemostasis was achieved with the application of one HemoClip (Fig. 2). The patient did not require blood transfusion and was discharged 48 hours later. There was no further bleeding and the patient did not develop pancreatitis.
Discussion
Approximately one-half of bleeding complications occur immediately after sphincterotomy; a delay of 24 hours up to several days is observed in other patients (1). Hemostasis can be achieved, by precise placing of a single or more hemoclips at the bleeding site. However, published cases of this treatment are limited (2,3). Clips may be difficult to apply with the side-viewing endoscope in the setting of active bleeding. In addition, clips may be inadvertently applied to the pancreatic orifice with the associated risk of pancreatitis.
References
1. Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med 1996; 335(13): 909-18. [ Links ]
2. Baron TH, Norton ID, Herman LSO. Endoscopic hemoclip placement for post-sphincterotomy bleeding. Gastrointest Endosc 2000; 52(5): 662. [ Links ]
3. Katsinelos P, Paroutoglou G, Beltsis A, Gouvalas A, Mimidis K, Vlachakis I, et al. Endoscopic hemoclip placement for postsphincterotomy bleeding refractory to injection therapy: report of two cases. Surg Laparosc Endosc Percutan Tech 2005; 15(4): 238-40. [ Links ]

