










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.7 Madrid jul. 2015
LETTERS TO THE EDITOR
Hepatocellular carcinoma with bile duct invasion presenting as acute cholangitis
Colangitis aguda como presentación de un hepatocarcinoma con trombosis tumoral de la vía biliar
Key words: Hepatocellular carcinoma. Jaundice. Bile duct thrombus.
Palabras clave: Hepatocarcinoma. Ictericia obstructiva. Trombosis biliar.
Dear Editor,
We report the case of a 72 year-old male who was admitted presenting with abdominal pain, jaundice and fever, being made a diagnosis of acute cholangitis. In the previous weeks, he had suffered significant weight loss.
In laboratory tests, we observed mild hyperbilirubinemia and hypertransaminasemia (bilirubin: 3.1 mg/dl; AST: 45 U/L; ALT: 29 U/L; GGT: 201; ALP: 343 U/L), elevated acute phase reactants and high alpha-fetoprotein levels: 885 µg/l (normal: 0-11 µg/l).
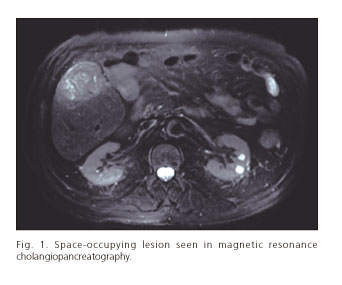
Several imaging tests were also performed (ultrasonography, computed tomography and magnetic resonance cholangiopancreatography) showing liver cirrhosis (not previously known) with a not well defined 5 cm space-occupying lesion (SOL) located in segment V (Fig. 1). The patient had high alcohol consumption for years and standard etiologic study (hepatotropic viruses, autoantibodies, etc.) was negative, so a diagnosis of chronic alcoholic liver disease was established. Radiology tests also showed dilatation of intra and extrahepatic bile ducts and occupation of these by a dense material, although the gallbladder was normal and free.
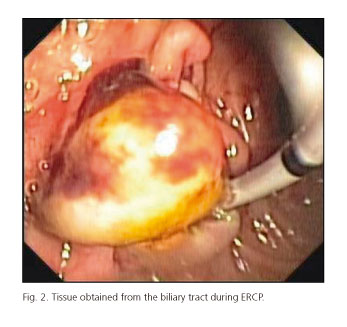
With all these findings an endoscopic retrograde cholangiopancreatography (ERCP) was performed. We found dilated bile ducts with repletion defects. Endoscopic sphincterotomy was made and an amount of soft, non-lithiasic material was obtained from the biliary tract and referred to anatomopathological study (Fig. 2). Ultrasound-guided fine needle aspiration of the SOL was also made, and both histological studies were respectively diagnostic for moderately and poorly differentiated hepatocellular carcinoma.
The liver lesion was resected and confirmed to be a moderately differentiated hepatocellular carcinoma (grade 3 of the Edmonson-Steiner's classification). However, the patient presented different complications after surgery, as well as an early recurrence and died after three months.
Hepatocellular carcinoma (HCC) is commonly associated with cirrhosis, being the leading cause of death in this population (1). Tumor thrombus in the bile duct in HCC is rare (0.79-5.5%) and the most common clinical manifestations are obstructive jaundice, abdominal pain, recurrent cholangitis or hemobilia. Biliary thrombi may be secondary to invasion of a primary liver tumor or due to a primary HCC arising on ectopic liver tissue located in the bile duct (2).
Diagnosis of this entity is difficult due to its low incidence and because findings in complementary tests are nonspecific, so many wrong diagnosis of cholangiocarcinoma or choledocholithiasis are made in these patients (3).
Surgical treatment is the first option if the lesion is resectable. It consists of resection of the lesion followed by thrombectomy. Some patients may benefit from transarterial chemoembolization and radiologic or endoscopic drainage as adjuvant therapies (3-5). These techniques can also be palliative in case of unresectable lesions (5). In selected cases liver transplantation can be considered, but there is scare evidence in terms of prognosis in this situation (6).
Patients with this entity present lower survival rates than those with HCC without biliary involvement, with early recurrence and worse response to treatment (3).
Juan Egea-Valenzuela, José Manuel Castillo-Espinosa,
Fernando Alberca-de-las-Parras and Fernando Carballo-Álvarez
Digestive Diseases Unit. Hospital Clínico Universitario Virgen de la Arrixaca. Murcia, Spain
References
1. Forner A, Ayuso C, Real MI, et al. Diagnóstico y tratamiento del carcinoma hepatocelular. Med Clin 2009;132:272-87. DOI: 10.1016/j.medcli.2008.11.024. [ Links ]
2. Ikenaga N, Chijiiwa K, Otani K, et al. Clinicopathologic characteristics of hepatocellular carcinoma with bile duct invasion. J Gastrointest Surg 2009;13:492-7. DOI: 10.1007/s11605-008-0751-0. [ Links ]
3. Qin LX, Tang ZY. Hepatocellular carcinoma with obstructive jaundice: Diagnosis, treatment and prognosis. World J Gastroenterol 2003;9:385-91. [ Links ]
4. Fukuda S, Okuda K, Imamura M, et al. Surgical resection combined with chemotherapy for advanced hepatocellular carcinoma with tumor thrombus: Report of 19 cases. Surgery 2002;131:300-10. DOI: 10.1067/msy.2002.120668. [ Links ]
5. Matsueda K, Yamamoto H, Umeoka F, et al. Effectiveness of endoscopic biliary drainage for unresectable hepatocellular carcinoma associated with obstructive jaundice. J Gastroenterol 2001;36:173-80. DOI: 10.1007/s005350170125. [ Links ]
6. Lee KW, Park JW, Park JB, et al. Liver transplantation for hepatocellular carcinoma with bile duct thrombi. Transplantation Proceedings 2006;38:2093-4. DOI: 10.1016/j.transproceed.2006.06.034. [ Links ]

