










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
ASD is a neuro-developmental disorder characterised by persistent difficulties in social communication and interaction, and restrictive and repetitive patterns in behaviour, interests and activities. Symptoms appear in the initial phases of development and lead to clinically significant functional, social and occupational impairments1. Table 1 summarises the different levels of severity in diagnostic criteria and classifications2.
Table 1. Diagnostic criteria and classification according to severity2.
| Diagnostic criteria | ||
|---|---|---|
| A. Deficits in communication and social interaction in a range of contexts, expressed as: 1. Deficiencies in socio-emotional reciprocity (abnormal social approach, lack of shared interests or affections). 2. Deficiencies in non-verbal behaviours (abnormal eye contact or body language, difficulties with comprehension and use of gestures, limited facial expressions). 3. Deficiencies in development and maintenance of relationships (ranging from incapacity to share games of imagination to absence of interest in other persons). | ||
| B. Restrictive and repetitive patterns of behaviour, interests and activities, expressed as: 1. Stereotyped movements, speech or use of objects (changing location of objects, echolalia). 2. Excessive inflexibility of routines, with ritualised patterns and insistence on monotony (greeting rituals, rigid thinking, difficulties with changes). 3. Restricted and fixed interests, abnormal in terms of intensity or focus of interest (unusual objects with restricted and insistent interest). 4. Hyper-reactivity or hypo-reactivity to sensorial stimuli (indifference to pain or temperatures, adverse response to specific sounds, excessive smelling or touching of objects). | ||
| C. Symptoms present from early stages of development, although they may appear when social demands exceed their limited capacity, or when strategies learned to conceal the disorder fail. | ||
| D. Symptoms cause a clinically significant deterioration in social and occupational settings and in other important areas of habitual functioning. | ||
| E. The symptoms are not more effectively explained by intellectual disability or global developmental delay. | ||
| Level 1 (Asperger's syndrome) | Level 2 | Level 3 |
| Presents difficulties in opening social interactions, with atypical answers during initial social exchanges with others. Offers complete sentences but fails in extended conversations. Attempts to make friends are strange and usually fail. Presents inflexible behaviour, with difficulties in alternating activities and problems of organisation and planning. | Social problems apparent, even with assistance, with limited initiation of interactions and lack of response to external social gambits. Special, highly specific interests. Restricted behaviours frequently appear and interfere with normal functioning. Anxiety with difficulties in changing the focus of action. | Few intelligible words, rarely starts interactions with others; when they try to do so, they use unusual strategies, responding to very direct approaches. Inflexible behaviour, with extreme difficulties in facing changes, very difficult to change the focus of action. |
The disorder has significantly increased over the last decade, with a worldwide prevalence of 1-1.5%3.
The estimated presence in Spain is 1.23%, with a proportion between sexes of 4.5 in favour of males4.
The prevalence of the disorder in penal settings is significantly higher than in the community5: around 4% of inmates present some autistic traits6,7, although figures of between 98 and 18%9. have also been detected. The general belief is that ASD is under-diagnosed in prisons, for reasons ranging from lack of human and material resources to a shortage of specific skills10,11.
The core symptoms of the disorder (lack of empathy, absence of communication skills, tendency to make false interpretations, poor recognition of emotions, emotional dysregulation, sensory problems, motor difficulties, intolerance to change) can predispose an autistic person to commit offences12. The links between ASD and criminal behaviour is first detected in childhood and adolescence: symptoms of autism have been found to be more common amongst young offenders than in the community, and are associated with future criminal conduct, even after adjusting the risks by including other externalising disorders13.
Up to 10% of young offenders (between 18 and 25 years) meet the criteria for diagnosis of ASD. Such inmates present poor academic performance, antisocial behaviour that commences at an early age and more aggressive behaviour14.
The risk of these patients committing a crime (and being imprisoned as a result) is determined by a lack of empathy, with difficulties in experiencing the emotional states of others15. It is important to distinguish between these deficits and others that form part of other psychiatric disorders such as antisocial personality disorder: while someone with ASD has difficulties in developing cognitive empathy (“I don't know what others think”), psychopaths are characterised by dysfunctional affective empathy (“I don't care what others think”)16.
On the other hand, autistic symptoms have a significant negative influence on a wide range of issues prior to a trial, in the court proceedings themselves and in sentencing17. For example, the lack of social skills of persons with ASD lead to them being sentenced with greater frequency, since they are incapable of lying or manipulating others for their own benefit18.
Although the number of criminal offences involving offenders with ASD has increased in several jurisdictions over the last decade17, most of the diagnoses of inmates are carried out after forensic assessments, when the offender is already involved in the judicial system12. This situation highlights the degree of ignorance of the problem, the lack of tools for early diagnosis, the shortage of specific professional training and poor adaptation of the penal system.
In short, ASD is highly prevalent in the penal setting, and inmates diagnosed with the disorder present unique social, clinical and criminal characteristics. However, there is little in the way of research on the status of autism in prisons, and there is no literature in Spanish on this issue. The lack of evidence makes it difficult to include diagnostic and therapeutic considerations for ASD within the prison psychiatric setting, but it seems indisputable that ASD is a multi-faceted and common condition with a complex profile. The aim of this review therefore is to analyse the characteristics of autism in the prison setting, to summarise and update our knowledge about the disorder in this area, and provide some foundations for future research.
Material and method
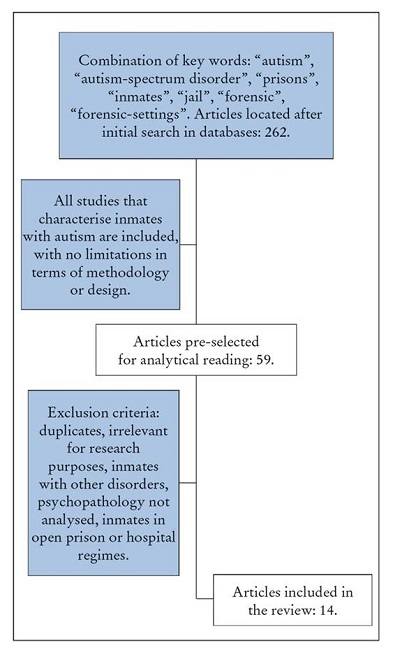
A systematic review was carried out using databases and search engines (PubMed, Dialnet, Cochrane and Google Scholar), according to the recommendations for preferred reporting items for systematic reviews and meta-analyses (PRISMA) with the following descriptors of medical subjects: “autism” AND “prisons”; “autism” AND “inmates” OR “prisoners”; “autism-spectrum-disorder” AND “prisoners” OR “inmates”; “autism-spectrum- disorder” AND “jail”; “autism” OR “autism- spectrum-disorder” AND “forensic-settings”.
All the studies that describe socio-demographic, clinical, judicial and/or penitentiary characteristics amongst inmates diagnosed with ASD were included. There was no exclusion criterion for the design, methodology, language or date of publication. Given that comparisons by sex were not included, no differences were established for this criterion. All the articles included were published before 20 November 2022, which was when the databases were analysed for the last time.
The studies were selected by two independent reviewers, who identified and compiled the relevant data. 262 articles were initially detected with the key words. 14 of these were selected after reading the titles and abstracts. The other studies were excluded because they were duplicated, irrelevant to the research or presented a different study sample (e.g. patients with intellectual disabilities or other neuro- developmental disorders, or serving sentences in open prison). Since there is little research in this field, all the results of the studies were described and presented, regardless of the extraction procedure, variables or statistical analyses.
The article selection process is shown in Figure 1.
RESULTS
Most of the studies were descriptive and focused on characterising inmates with ASD in comparison to their neurotypical peers. The analysis of the methodology and findings of the studies can be seen in Table 2.
Table 2. Analysis of studies included in the review.
| Author and year | Methodology | Results |
|---|---|---|
| Allen et al. (2008)29 | Semi-structured interviews with autistic patients housed in different forensic and prison units in South Wales for aggressive behaviour. All the patients were male with an average age of 34.8 years (range: 18-61). | The participants describe aspects of the prison dynamic that they find hard to cope with: uncertainty, boredom, accepting external routines, difficulties in making friends, transfers after getting used to the setting, sharing cells with strangers, lack of common areas and lack of comprehension from staff. |
| Haw et al. (2013)22 | Case-control study in a low security centre, with two units with ASD patients and one without patients with this diagnosis. 51 autistic patients and 43 controls were included. Cases were 27 years old on average, while the controls were 33 years of age. The mean age for diagnosis of ASD was 21 years (range: 6-56). Socio-demographic, clinical and criminal variables were compared. | Inmates come into contact with the psychiatric services at an earlier age, and have more contact with courts and prisons. Almost 75% have a psychiatric comorbidity. The diagnosis of schizophrenia is especially common. The control subjects on the other hand suffer more frequently from personality and substance use disorders. The autistic inmates present sexually inappropriate behaviour, physical violence and non-compliance with medication less frequently. However, 78% have presented disruptive behaviour at some time in their lives. |
| Murphy (2014)25 | Evaluation of 20 males with ASD housed in a high security centre between 2002 and 2011. The mean age was 35.3 years. The Autism Spectrum Quotient and the State Trait Expression of Anger Inventory was applie | Differences in self-reporting of anger amongst patients whose offence is related to achieving a specific end or concern, and those who commit impulsive and aggressive acts. The first group describes more sensitivity in coping with the details of the immediate surroundings, with difficulties in expressing their anger. The second group is associated with more psychiatric comorbidity and less capacity in controlling external expressions of anger. |
| McCarthy et al. (2015)20 | Sample made up of 240 inmates of a prison in London, who were evaluated with the 20-item Autism Quotient and the Mini International Neuropsychiatric Interview. | Autistic traits are detected in 16% of participant. This variable has statistically significant associations with suicidal tendencies and episodes of generalised anxiety and depression. |
| Newman et al. (2015)30 | Interviews with eight males housed in seven correctional centres in New South Wales (Australia). Their ages range from 21 to 43 years (average of 24). According to the DSM-IV criteria, and based on their clinical record, two patients suffered from autism and six were diagnosed with Asperger's syndrome. The prison sentences ranged from 3 months to 6.5 years, with an average of 2 years and 10 month | Participants declare that they feel that they are in an unpredictable environment, and complain about difficulties in understanding the dynamics of the prison setting. They also mention difficulties with regulating and controlling their own world. Their habitual reactions to demands that they cannot cope with are self-isolation and avoidance |
| Loureiro et al. (2018)32 | 101 inmates at a high security prison in Coimbra (Portugal) were recruited between October 2015 and January 2016. The mean age was 37.4 years (range: 22 to 63). The control group was recruited between January and October 2016 and was made up of male volunteers, with no previous criminal or psychiatric record, paired by age and educational level. The mean age was 39.3. They were evaluated with self-questionnaires that included the Brief Symptom Inventory, the Adult ADHD Self-Report Scale-V1.1, the Triarchic Psychopathy Measure and the Autism Spectrum Quotient. | The prison sentences for the sample were for crimes against property (41.6%), manslaughter (26.7%), crimes of bodily injury (15.8%), drug trafficking (7.9%) and theft (4%). The inmates present higher autistic traits than the members of the control group, regardless of age, educational level, general psychopathology, symptoms of ADHD or level of psychopathy. The sub-domains of communication and imagination are statistically significant. No association is found between autistic and psychopathic traits. |
| Helverschou et al. (2018)31 | Interviews with nine persons diagnosed with ASD, recruited from patients who underwent a psychiatric-forensic examination in Norway between 2000 and 2010. The sample was made up of eight males and one female with a mean age of 34 years. | They describe a situation where the diagnosis is not understood in the judicial and prison systems. They acknowledge that stress was one of the triggering factors in the crimes committed, along with misinterpretations, obsessions and beliefs commonly held by persons with the disorder. Most comment that they have adapted well to prison, probably because of the fixed structure and existence of inflexible regulations. Several participants showed little understanding of the crimes committed or their impact on third parties. |
| Girardi et al. (2019)24 | Retrospective evaluation of demographic, clinical and legal variables amongst admissions with autism in prison psychiatric units in England. The final sample consisted of 28 men admitted between 2014 and 2016. | Violent episodes are recorded in over 50% of the subjects with ASD, with more physical than verbal aggression. The scales used do not predict any violent episode above random levels. Psychiatric comorbidity constitutes a statistically significant risk factor in the appearance of difficult behaviour. |
| Hofvander et al. (2019)27 | Interviews with males recruited between 2010 and 2012, using the Development of Aggressive Antisocial Behaviour Study, a national cohort of young people held in nine prisons in Sweden for violent crimes and sex offences. 26 patients with ASD were included in the 269 participants (mean age of 21.6 years). The Structured Clinical Interview for DSM-IV and the Psychopathy Checklist-Revised were administered. | When compared to their neurotypical peers, inmates with ASD present higher levels of psychiatric comorbidity with complex clinical trajectories that include psychosocial difficulties (periods in foster care, etc.). No differences were found with regard to externalising behaviours, violent attitudes and variables related to the offence. |
| Vinter et al. (2020)28 | Interviews with seven autistic inmates at a prison in Whatton (UK). The average age was 34.4 years (range: 23-47). All of them were serving sentences for sex offences. | The participants recognise that they find it difficult to interact with others, and to interpret emotions and feelings. They also admit to a tendency to misinterpret certain situations. They find the prison structure, with its rules and routines, frustrating and stressful, with too much noise. They also feel that their cellmates and prison professionals do not understand the diagnosis and its implications. |
| Payne et al. (2020)26 | Semi-structured interviews with nine autistic inmates at prisons in England and Wales, with an average age of 29.5 years (range: 22-50). The average IQ, using the Wechsler Abbreviated Scale of Intelligence, was 87.56 (range: 64-102). All of them were serving sentences for sex offences. | The inmates gave their lack of social skills as a reason for committing the offences (feeling different from others, loneliness), along with problems with understanding situations (lack of perspective, analysis of consequences, reasoning, established rules, degree of seriousness), limitations in affective and sexual relationships, difficulties with adequate self-control and a situation of personal instability (lack of social and family support, substance use, increased impulsiveness). |
| Bosch et al. (2020)23 | The sample was made up of 32 patients with ASD admitted to a forensic psychiatric hospital in the Low Countries. 90.6% were men, with an average age of 37.7 years (range: 22.4-57.3). 62.5% of the sample had been previously convicted of violent crimes. They were evaluated with the Historical Clinical Future-Revised, the Social Dysfunction and Aggression Scale-11 and the Structured Assessment of Protective Factors for violence risk. | A high presence of comorbidity was detected, with a notable prevalence of substance use (46.9%), psychotic disorders (31.2%), paraphilic disorders (15.6%), personality disorders (15.6%), intellectual disability (9.4%) and ADHD (3.1%). The evaluation instruments have a limited usefulness, as no associations with the risk of aggression in hospital are detected. |
| Van Buitenen et al. (2021)21 | All the inmates with a diagnosis of autism who were admitted into psychiatric hospitals in the Low Countries between May 2013 and December 2019 were included. A final sample of 394 offenders with an average age of 31.7 years was identified. Socio-demographic variables, psychiatric monitoring records and information about criminal records were examined, including the age when the first offence was committed and any recidivism. | 78.9% present psychiatric comorbidity, with a notable prevalence of substance use disorder (39.8%), psychosis (31.7%) and neuro-developmental disorders (24.1%). Inmates with comorbidity added to ASD are more likely to repeat offences and require more prolonged psychiatric treatment. |
| Chaplin et al. (2021)19 | The sample consisted of 240 male inmates at a prison in London. ASD was evaluated with the Autism Quotient and the Autism Diagnostic Observation Schedule. Symptoms of depression and anxiety, and self-harming and suicidal behaviours were explored with the Mini International Neuropsychiatric Interview. | Inmates with autistic traits have a significantly higher probability of thinking about self-harming and/or committing suicide in the previous month. 64.9% report having attempted suicide at some point in their lives, compared to 11.6% of neurotypical inmates. Autistic traits are also associated with psychiatric comorbidity (depression, anxiety, personality disorder). |
Note.ADHD: attention deficit hyperactivity disorder; DSM-IV: fourth edition of the Diagnostic and Statistical Manual of Mental Disorders; ASD: autism spectrum disorder.
It was found that inmates with autistic traits are significantly more likely to present self-harming behaviours and committing acts of self-injury19,20. They run a higher risk of developing a concomitant mental disorder and are associated with higher rates of disruptive and violent behaviour19.
Notable features in the high levels of comorbidity (78,9%) are substance use disorder (39.8%), schizophrenia spectrum disorders (31.7%) and other neuro-developmental disorders (24.1%)21. When compared to neurotypical inmates, they present higher levels of psychotic comorbidity and less physical violence and deviant sexual behaviour22.
It was also found that psychiatric comorbidity and the existence of a negative social environment (where subjects can be influenced) are statistically significant predictors for violent crimes21. What is more, the assessment tools traditionally used to predict the risk of violence are not adapted to inmates with ASD, and do not effectively anticipate disruptive episodes23,24. Self-reporting of attacks of rage are crucial in this regard, since they enable personnel to understand the causes of the attack and so anticipate this type of reaction25.
Difficulties with social skills, weak central coherence, poor understanding of the seriousness of their behaviour and the lack of appropriate relationships are the main causes of sex offences26, which are more common amongst autistic inmates27.
One interesting feature is the subjective experiences of this type of inmate in prison. Inmates with autism describe how they regard prison as an unpredictable environment, characterised by constantly changing routines and complex social situations28,29. It is difficult for them to find predictability and feel confused and anxious when obeying orders that come into conflict with their logic30. However, there are other contradictory results that indicate that they can adapt better to prison thanks to the high levels of structuring, with firm and unchanging regulations31.
Autistic traits are significantly higher amongst inmates in high security units in comparison to the general population, especially in the domains of communication and imagination. Even so, no correlation was found between autism and psychopathy, indicating that the presence of the first element acts as an independent risk factor for imprisonment32.
Finally, given that inmates with ASD describe adverse backgrounds since early infancy (with abuse and socio-economic insecurity), early diagnosis is essential to limit the impact of the disorder (including the period of criminal behaviour)27.
Discussion
Our systematic review is the first study in Spanish that summarises and analyses the status and situation of autism in prison, and the characteristics of inmates diagnosed with this disorder. It is evident that such inmates present a special profile that requires specific management by medical professionals who work in the judicial and penitentiary settings.
Previous publications concluded that inmates with ASD suffer from considerable distress because they cannot establish any degree of uniformity in a constantly changing environment that they experience as threatening and unpredictable30. They are more vulnerable to harassment, social isolation and sexual victimisation33. Social deficits and difficulties in communication make it difficult for them to successfully cope with the complex situations that exist in the prison setting30. They do not understand formal and informal social hierarchies, and find it difficult to interiorise rituals and routines imposed by others34. All this is borne out in the results found in our research, and back up the notion that autistic inmates are a vulnerable sub-population in prison, with a higher associated risk of exposure to intimidation, exploitation, confrontations, anxiety and social isolation35.
Most of the inmates with autism spectrum disorder are undiagnosed, and do not receive specific medication unless they have associated disorders (especially intellectual disabilities)30. The fact that they only receive treatment if they have a comorbidity may be justified if one considers that inmates with neuro-developmental disorders present a higher probability of suicidal ideation and concurrent mental disorders (psychosis, anxiety, depression, substance abuse)36, which makes it easier to detect and treat them.
However, as our review shows, most autistic inmates suffer from psychiatric comorbidity. Furthermore, disruptive and violent behaviour is stimulated and triggered by concomitant disorders37. It was found that inmates with autism and attention deficit and hyperactivity disorder (ADHD) present more severe behavioural changes than autistic inmates without this comorbidity8.
Being male and having a psychiatric comorbidity (ADHD, psychosis and substance abuse) are the risk factors most commonly associated with episodes of violent criminal behaviour38,39, which in turn lead to entry into the criminal justice system40. Young people with autism also run a higher risk of being accused of a serious crime (with a prison sentence of more than two years), than their neurotypical peers41.
Between 3%42 and 5.7%43 are accused of at least one offence when they reach adulthood, while up to 60% sentenced for sex offences meet the diagnostic criteria for ASD44: the social deficits inherent in the diagnosis, along with difficulties in social cognition, increase the risk of this type of crime45. Many of the offenders sentenced for crimes of sexual aggression were found to be autistic46.
Despite the magnitude of the problem, prison services do not provide adequate support to inmates with ASD. Improvements are required in diagnostic processes, as is multi-disciplinary collaboration between internal and external providers to develop a care model based on individualised case management47. There is also a need to develop a tool that evaluates the specific risks of persons with ASD, since the commonly used evaluations do not effectively predict the risks run by this patient profile of committing a violent crime24.
It is essential to promote specific training for prison staff48,49) and develop interventions for sexual-affective education that are adapted to the levels of awareness and knowledge of autistic persons, in order to prevent sex offences26. Such training should be extended to other agents in the judicial system, including lawyers and the police50. The institutions themselves should also promote policies for inclusion, including awareness-raising campaigns on neuro- diversity amongst inmates51.
It should be noted that awareness of inmates with ASD has increased in recent years. For example, in 2015, the Feltham Young Offenders Institution in London was given accreditation for a specialisation in autism regulated by the National Autistic Society, making it the first prison in the world to achieve such a milestone52. Even so, there is still a great deal of work to do.
Early identification of the diagnosis enables the provisions needed by inmates to be promptly evaluated, and minimises the risk of the onset of other comorbid mental disorders, with emphasis on the provision of specialist services and reduction of recidivism. The penitentiary context needs to be changed and adapted to offer approaches for processing inmates with autism, encouraging coordination with outpatient services that can guarantee continuity of care after release from prison.
Limitations
There were a wide range of study designs included in the review, and variations in the diagnosis and characterisation of the inmates with autism. There are few studies on this issue, with very limited samples, and the focus is usually on judicial settings (interactions with the penal system). Other studies consider the matter solely from a medical perspective (in psychiatric/prison hospitals). Few studies have focused exclusively on providing a complete evaluation within prisons.
On the other hand, some studies included research from countries with different socio-cultural contexts, and so some care should be taken when generalising the results.
Finally, although the disorder presents a differential prevalence, all the studies focused on male autistic inmates, so more in-depth studies on the female sub-population are highly recommended, given the important implications this could have for tailoring intervention approaches.
Conclusions
This review shows that inmates with autism spectrum disorder present a differential socio-demographic, clinical and judicial profile. Inmates with ASD run a higher risk of self-harming and disruptive behaviour. They also present complex psychiatric comorbidities, suffer from difficulties in adapting to a hostile and inflexible environment, and their psychopathology evades traditional screening methods.
Their approach to reality is rigid, unregulated, distant, ambiguous and literal, all of which plays a large part in their criminological profile and their interactions with the judicial and penitentiary systems.
The magnitude of the problem makes it necessary to develop specific approaches inside the prison itself, optimising resources and infrastructures that can help with the fragile nature of this type of inmate. A more flexible prison setting, new evaluation methods and changes to therapeutic management would be effective in this regard.

