










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Complete knee dislocation (CSF) is an uncommon lesion that should receive immediate attention due to the danger of secondary complications. It is usually caused by high energy trauma, such as traffic accidents; but they can also be the result of minor accidents (i.e. sports injuries) [1].
The CSF is classified according to anatomical criteria according to the position of the displacement of the tibia on the femur in anterior (40%), posterior, internal or external. In general, it usually presents concomitant lesions of the stabilizing structure of the knee and is often accompanied by neurovascular lesions, including popliteal thrombosis, compartment syndrome and neuroapraxia, which may reach the neurotmesis of the peroneal or tibial nerve [1,2].
A purpose of a case of a patient with a complete anterior dislocation of the left knee, we summarize a brief review of this pathology.
CASE REPORT
A 51-year-old patient was admitted in the Emergency Department (ED) after a skiing accident. Femoral fracture and ligament injury in the left knee are suspected, as well as contusion in the left gluteal area. Denies head trauma. There has been no loss of consciousness or thoracic or abdominal trauma.
On physical examination the patient has good general condition, with pale skin and affected by pain. Any disturbs were observed at cardiac, pulmonary as well as abdominal exploration. No pain on palpation or mobilization of lumbar, dorsal or cervical spine was also observed. Attending to lower left limb, hypoesthesia in 1/3 distal was observed, with posterior tibial doppler flow +, negative pedio, although with good capillary filling. No pain to compression of the pelvis or pubic symphysis. Pain in the left gluteal area was also referred, without bruising or external wounds.
X-ray was performed to complete the study of the lower left limb, showing anterior dislocation of the knee with fracture of the left fibula head (Figure 1). According to these results, a traumatology assessment was realized, transferring the patient to the operating room to perform a closed reduction.

The day after the surgery, the patient referred mild pain at the level of twin musculature as well as paresthesias below the knee to the proximal region of the ankle and anesthesia of the ankle and foot. Physical examination showed complete motor deficit of the ankle and foot, without thermal disrupts as well as correct distal capillary filling, but with weak distal pulses. After this examination, a computerized axial angiotomography (angio-CT) was performed (Figure 2) revealing a complete obliteration of the left popliteal artery at the level of the femoral condyles, without observing contrast leakage suggesting a rupture or blood collections. Distal repermeabilization of the three tibioperoneal trunks was observed.
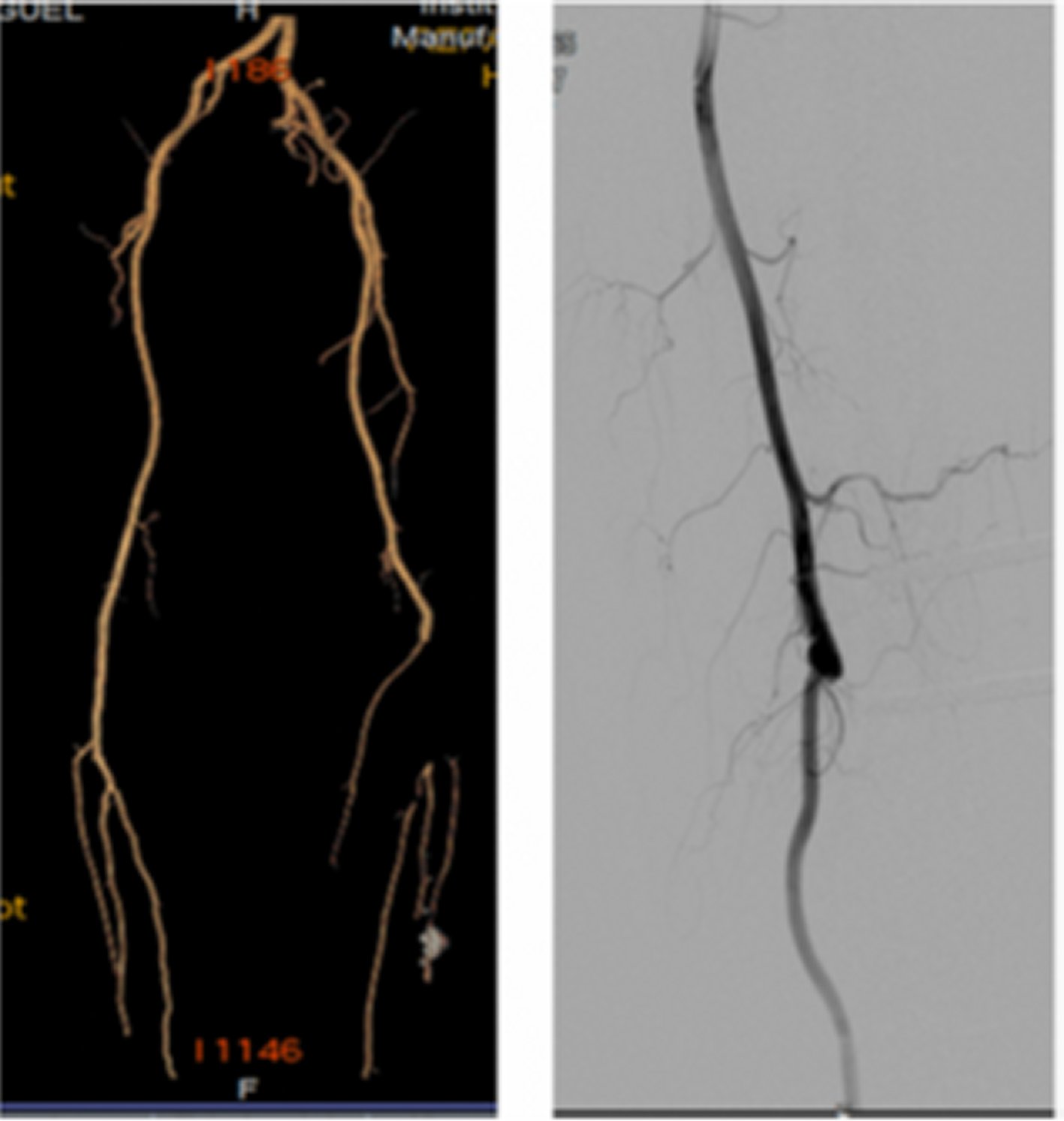
Figure 2. Angio-CT scan showing complete obliteration of the left popliteal artery at the level of the femoral condyles, without observing contrast leakage. Distal repermeabilization of the three tibioperoneal trunks is observed.
Attending to these results, a thrombectomy of the distal trunks from the third popliteal portion was performed extracting part of a good caliber saphenous vein, a distal anastomosis of inverted saphenous terminoterminal vein in the third popliteal artery and intercondylar tunneling. After that, a proximal anastomosis in the first terminal lateral popliteal portion was also realized.
After surgery, the patient was transferred to the Intensive Care Unit (ICU) suffering a compartment syndrome, performing a fasciotomy on the left lower limb. 10 days after his admission in ICU, the patient was discharged to the Department of Traumathology to manage the postoperative process. The patient was discharged from the hospital after 10 days.
DISCUSSION
The complete anterior dislocation of the knee represents about 0.2% of the trauma emergencies, being a rare but a difficult pathology to manage [1]. The literature describes that CSF may be reduced spontaneously, however, the majority are accompanied by inadvertent lesions, being extremely relevant a correct initial assessment. Normal radiological examinations, after a spontaneously reduction do not rule out concomitant lesions or complications, including popliteal artery Injury, compartment syndrome, nerve lesions and ligament and menisci lesions [1,2].
The CSF classification may suggest these complications. In example, popliteal artery injury is observed in 30-40% of cases, being more frequently showed in anterior dislocations due to the mechanism of hyperextension. On the other hand, posterior dislocations are produced by shear, being less frequent this injury [1]. Attending to the diagnosis, the literature is controversial, suggesting that the arteriography or angio-CT must be performed routinely in all cases of knee dislocation [3], or only requested in case of clinical suspicion [4]. When an extremity has an absence of distal and popliteal pulses, cyanosis, ecchymosis, palpation pain, swelling and foot with temperature decrease, arteriography should not be delayed [3]. Successful completion of revascularization is between 6 and 8 hours, showing a high rate of limb amputation (85%) if this time is increased [4].
Within this group of complications we include compartment syndromes, produced due to an increase in interstitial pressure within a closed compartment with neurovascular involvement [5]. They produce very similar symptoms and that often overlap with those of pure vascular or nervous origin. However, when the pain is disproportionate we must think that compartmental syndrome is involved. Clinical suspicion is confirmed if intracompartmental pressure is greater than 30mmhg being necessary a fasciotomy with posterior close of the incision at 72h with separate points [1]. If it is not available to measure the pressure and the clinic is unequivocal, the fasciotomy should be also performed.
The nerve injury ranges between 16 and 43%, being more frequently observed in posterolateral dislocations. The external popliteal sciatic nerve is the most common injured [6]. To evaluate this injury, a physical examination under anesthesia should be realized, performing Magnetic Resonance Imaging to confirm the suspicious. If a progressive deterioration of neurological function is observed, an ischemic complication or a compartment syndrome should be suspected [7].
The treatment of choice in the ED is the closed reduction of dislocation in the operating room in one or two times, depending of the hemodynamic stability [8].
In conclusion, the CSF is a rare pathology that involves multidisciplinary team, including the ED, Traumathology, Radiology, Vascular Surgery, and Plastic Surgery departments, in order to prevent or treat as soon as possible associated lesions.

