










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Nowadays, child abuse is a prominent problem in the worldwide public health sector that is present in all socioeconomic and educational backgrounds. It persists despite the numerous information and awareness-raising programs in place to educate both professionals and the general public. Such programs focus on the occurrence, the indicators of suspicion, the complaint mechanisms and the possible sequels [1]. More concretely, the OMS estimates that, each year, 22.9% of the children under the age of 18 in the European region suffer from physical abuse and 9.6% from sexual abuse. Despite the alarming numbers, many of those cases of child abuse are not reported [2].
Children can be exposed to multiple forms of abuse with different consequences in the oral cavity and teeth. That is why dentists might be the first ones to detect them. Thus, dentists should be provided with the relevant training to identify those lesions and manage the situation adequately. Dentists, similar to other healthcare professionals, are obligated to notify signs of child abuse suspicion. As a result, a well-prepared and aware oral healthcare professional is a basic pillar in the protection of the minor [3].
The objective of this work is to revise the oral aspects derived from child abuse so as the psychological consequences in the dentist-patient relationship and the role of dentists in the detection and notification of such circumstances.
METHODS
Systematic review study according to PRISMA statement [4]. Two search strategies [Search 1 and 2] from the MEDLINE/PubMed database were carried out until July 2019. Search 1 used the following equation: "Child abuse"[MeSH Terms] AND "Dentists"[MeSH Terms], without year limit. The filters applied were Full text and English language, with the equation: "Child abuse"[MeSH Terms] AND "Dentists"[MeSH Terms] AND ["loattrfull text"[sb] AND English[lang]]. Search 2 was based on the following equation: “Dentist-Patient Relations”[Mesh] AND Dental abuse, without year limit, with filters Full text and English language, and so the equation is given by: "Dentist-Patient Relations"[Mesh] AND [["dental health services"[MeSH Terms] OR ["dental"[All Fields] AND "health"[All Fields] AND "services"[All Fields]] OR "dental health services"[All Fields] OR "dental"[All Fields]] AND ["substance-related disorders"[MeSH Terms] OR ["substance-related"[All Fields] AND "disorders"[All Fields]] OR "substance-related disorders"[All Fields] OR "abuse"[All Fields]]] AND ["loattrfull text"[sb] AND English[lang]].
Figure 1 shows the flux diagram of both bibliographic search strategies and the study selection process. In Search 1, without filters applied, 228 publications were identified. After the application of the selection criteria 65 publications remained. After this, 45 publications were excluded as their titles were not related to the current study. Additionally, 8 more publication were discarded as the abstract did not relate to the objectives of our revision. Consequently, 12 publications were included in the final selection. On the other hand, in Search 2, without filter application, 116 articles were identified, that were reduced to 48 after the search filters were applied. 30 of these publications were then discarded after identifying that the title was not related to the revision, with 18 articles remaining. Similarly, after the analysis of the abstracts, 11 publications were excluded from the selection as their objectives did not meet the ones of our study. Finally, 7 publications were selected for our revision.
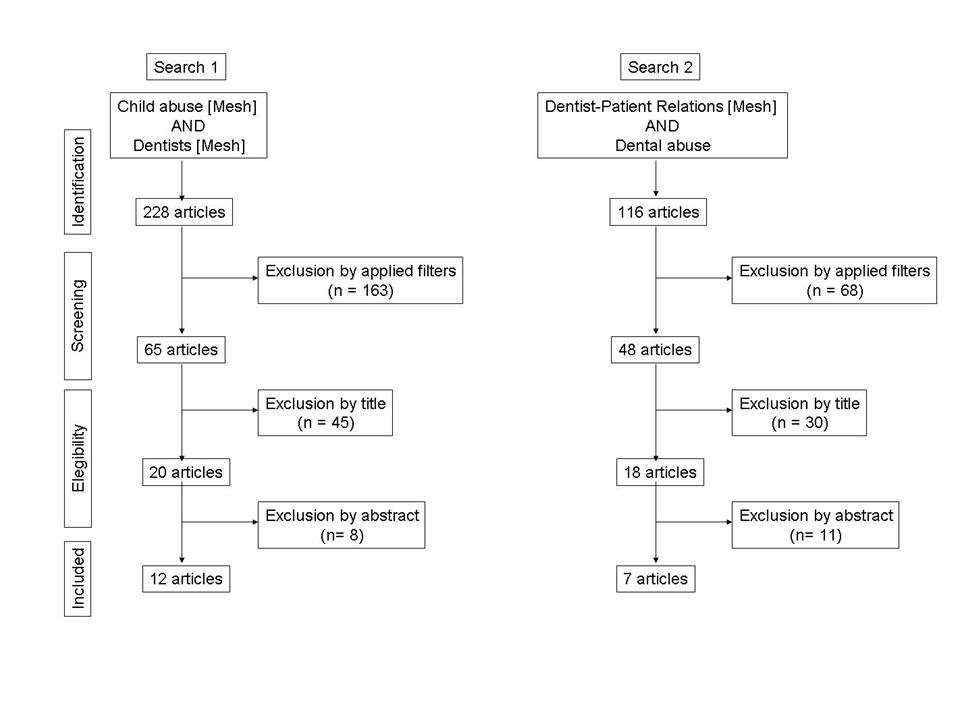
The combination of both bibliographic searches resulted in 19 publications that were selected for revision and whose results are described in the discussion section.
RESULTS AND DISCUSSION
ORAL LESIONS AND DISEASES OF CHILD ABUSE
Most frequent forms of child abuse include physical abuse, neglect and sexual abuse. Lesions and diseases related to those abuses often appear in the craneofacial region and more concretely in the oral region [up to 55% of physical abuse and up to 15% of sexual abuse cases]. As a result, a dentist might be the first healthcare professional that examines the victim of child abuse. Unfortunately, a high percentage of dentists [between 60-80%] state that they possess limited information on the topic and appear to lack the appropriate training to detect it [5, 6, 7, 8, 9, 10, 11]. Consequently, it is essential for dentist to acquire the knowledge to detect lesions and diseases that could be a consequence of abuse.
In Table 1 we list the oral and dental lesions and diseases which constitute indicators of suspicion of physical abuse and neglect [5, 6, 7, 8, 9, 10, 11, 12, 13, 14].
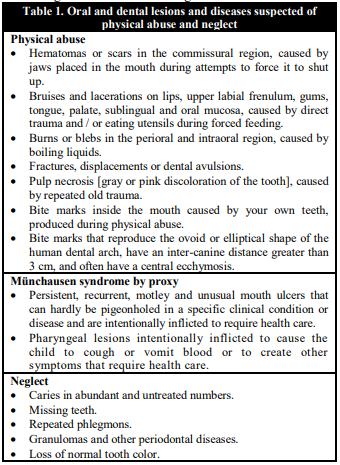
Regarding physical-abuse-related lesions, it is important to consider that as none of them are pathognomonic it is essential to focus on indicators of high suspicion. This indicators are: lesions incompatible in either extension, depth, location, distribution or pattern-type with the child age or their development level; lesions incompatible with the provided story; lesions in different stages of healing; frequent and reiterated lesions in children under 6 years old; lesions in children under 9 months old or children that do not yet move autonomously.
Despite it being infrequent, the Münchausen syndrome by proxy or factitious disorder imposed on another should be taken into account due to the severe physical and emotional damage that could manifest in the minor. The syndrome generally occurs in children under 5 years old and lesions are typically intentional, conscious and planned as the mother reiteratively injures the child. After this, the mother usually seeks for healthcare assistance with the objective of obtaining some diagnosis and treatment. Nevertheless, her conscious behaviour does not produce any economic or social benefit but only the ‘psychological benefit’ from being in contact with health professionals and gaining their sympathy, solidarity and compassion for being the carer of a ‘poor sick child’. Her psychological motivation is in assuming the role of the ill through her own child.
Diseases related to neglect in the oral care and attention are usually linked to other health problems derived from chronic physical neglect in diet, hygiene, home safety and basic healthcare. As a result, these lesions are often examined by dentists after the children have entered the child protection system and, from there, are derived to oral healthcare services for their treatment.
In Table 2, we list the oral lesions and diseases that suggest or indicate sexual abuse [12, 13, 14, 15, 16].

Beyond the finding of sperm or seminal fluid in the perioral are and/or the oral cavity, only infections of Treponema pallidum and Neisseria gonorrhoeae can be considered as clear indicators of sexual abuse. The rest of the lesions and diseases might suggest sexual abuse but are not pathognomonic.
Treponema pallidum infection manifests as a painless and indurated necrotic ulcer with raised edges, which lasts between 3 to 6 weeks, typically present in the amygdalae with associated ipsilateral adenopathy and less often in the pharynx and other zones of the perioral and oral cavity.
Neisseria gonorrhoeae infection appears as multiple ulcers with a white pseudomembrane accompanied by bright red oral mucous. It often appears as pharyngitis, but can sometimes appear as tonsillitis, gingivitis, stomatitis or glossitis. Despite it being most commonly asymptomatic, it can cause itch or burn feeling or even become painful.
Human papillomavirus infection manifests in the perioral level as condyloma acuminatum, verruca vulgaris or squamous papillomas, typically not painful, and in any surface of the pharyngeal or oral mucosa.
Chlamydia trachomatis infection appears as an ulcer in the oral cavity or the pharynx, which can be painful and that disappears without treatment. Additionally, painful inflammation of the lymph nodes near the initial lesion appears after 2 to 6 weeks.
Herpes simplex virus infection manifests as gingival enanthema, oral mucosa haemorrhage and clustering of small blisters, which evolve into pustules, in all regions of the oral mucosa including tongue, palate and perilabial skin. These blisters and pustules often burst giving rise to highly painful ulcers with dimensions around 1-5 mm. These ulcers, with corrugated edges and surrounding erythema, tend to coalesce.
PSYCHOLOGICAL ASPECTS OF CHILD ABUSE IN THE DENTIST-PATIENT RELATIONSHIP
The psychological patterns as a consequence of child abuse are numerous and many can persist even during adulthood. One of these is the fear of dentists. Dental phobia is an indicator of oral health. Patients suffering dental phobia do not typically get regular checks, suffer from more oral health problems and would only meet their dentists when they require treatment. Some signs of dental phobia are easily detected. Patients usually voluntarily say they feel nervous. Dentists can observe physiological reactions during treatment. Other factors are harder to detect, such as lack of trust or negative reactions to physical intimacy. Several studies have linked the fear of dentists or dental phobia with victims of physical or sexual abuse and not just individuals with negative dentist experiences in the past. In particular, 34% of women with a strong fear of dentists reported histories of sexual abuse as children; this includes 15% who reported rape attempts and 13% reporting rape or incest. Thus, there is a significant link between the fear of the dentist and child abuse arising from the similarity between situations of abuse and dental treatment [12, 15, 16, 17, 18].
As a result, it is essential to differentiate between two types of fear of dentists: the one linked to negative previous dental experiences and the one associated to child trauma or abuse. Victims of sexual abuse can associate certain situations during dental treatments with traumatic memories. In both situations, the minor is left alone with a more powerful individual that then positions them horizontally, anticipating or experiencing pain. Abusers often start with some activity that seems harmless and frequently link their sexual behaviour with positive motivations, such as love or the need for education. Similarly, in the dental clinic, patients are expected to rely on the dentist and their ability to provide the best possible treatment for them. Dentists usually assure the patient that, similarly to the abusers, despite the experience potentially being painful or unpleasant, the result would be positive. In addition, sexual activity often involves both mouth and genitalia of the minor which links with the dental treatment that requires accessing the mouth of the patient. Over 90% of the victims of forced oral sex report deep dental phobia, fear of being trapped in the dental chair, fear of drowning and nausea when dental instruments are introduced in their oral cavity. As a result, dentist struggle to build a trust relationship with those patients. Therefore, it is essential for the dental care of victims of sexual child abuse that dentists adapt their treatment planning to the specific needs of those patients [12, 17]
THE ROLE OF DENTISTS IN THE DETECTION AND REPORT OF CHILD ABUSE
Reporting a suspected case of child abuse can become a clinical, ethical and legal dilemma that arises from the different professional roles, difficulties to confirm the suspicion of abuse and perceived deficiencies in the child protection system. Compared to other healthcare professionals, dentists report a lower number of cases than doctors or nurses, with 18%, 38% and 44% respectively. The most common cause of report by dentists is from repeatedly missing dental appointments and the lack of dental care while other forms of abuse are rarely reported. It is important to consider that missing dental appointments arises from complex family problems and it is more common in families with poor dental care. This is also linked to dental phobia. Additional studies have proven that between 21-38% of the suspected cases of child abuse are not reported. In order to successfully confirm cases of suspicion it is essential to establish adequate clinical records. In potential cases of abuse, lesions and diseases in the oral cavity should be recorded together with other significant psychological signs, such as the way that the minor interacts with their parent or guardian. It is essential to obtain photographic evidence of the lesions and, in the event of suspicion of sexual abuse, samples of the oral mucous and tongue with an air-dried sterile cotton swab which is then conserved adequately for laboratory analysis. These records would them become essential for both assessing the treatment evolution and supporting the legal procedure for the child protection [6, 8, 9, 17, 19, 20].
The apparent difficulties that dentist experience when reporting cases of child abuse stand out. For example, in the USA, between the years 1995-2012, approximately only 1% of child abuse reports received were created by dentists. A surprisingly low percentage specially taking into account that dentist has an advantageous position to detect and report suspected child abuse cases with oral signs. One of the main reasons that affect the dentist ability to report abuse is that between 20-67% of dentists ignore the contact people in the report process. In addition to this, dentists detecting signs of suspicion outside their professional competence, typically focus on guaranteeing the general wellbeing of the child rather than suspecting abuse. In many of the cases of sexual or physical abuse, the signs were often too vague to create a report with a proper description of the abuse suspicion. Cases where parents were making their child miss the treatment despite an untreated cavity would confirm their abuse suspicions. However, in cases were the parents would acceptably fulfil the dental treatment requirements, dentists expressed their dilemma in whether to inform or not. As a result, it is complex to establish well-defined thresholds for the obligation to notify abuse with varying opinions in the evaluation among the child abuse experts [8, 11, 16, 21].
The hesitation to report can also arise from the uncertainty of the notification actually improving the child situation and the fear that an unnecessary report could damage the family relationship. Furthermore, dentists often seem to prioritise providing the dental treatment over reporting to social services. This might be caused by the possibility of a report interrupting the dental treatment and damage the family relationship or by the concern whether enough evidence exists for a report. It is important to highlight that in cases of hesitation in the informant, the social services comments played an essential role in the decision to report. On the other hand, in cases of confirmed dental negligence, reports were created despite this lack of communication. Other possible barriers for the report and notification are related to the fear of violence against the professional and the fear of a court case. Nowadays, the number of child abuse reports has increased, but a significant mismatch exists in the number of suspected and reported cases [8, 22, 23].
Now, we will discuss several indicators that might confirm the sexual abuse suspicions. This includes irrational or incompressible fear to the visit to the dental office, potential nausea arising from either the latex-glove smell or the oral exploration and the dental carelessness. Common fears reported by the victims include the need to lay down to receive treatment, the presence of objects in their mouths, the feel of the dentists hand over their mouths and/or noses, the inability to breathe or swallow, the perceived loss of control and the concern of upsetting the dentist. Moreover, patients who were sexual abuse victims might experience anxiety or powerlessness as they are unable to close their mouths or communicate during the dental care. Dental phobia can become more complex than just fear of pain or needles as the supine position being unable to speak, the lack of control and the fear to be touched can appear in the patients without the dentist being aware [7, 13, 17].
After a potential child abuse case is detected, it should be notified to social services, the child protective services and/or the juvenile prosecution service. This is a mandatory step in order to ensure the intervention and guarantee the legal and professional obligation. In the case of Spain, the notification is through a specific document, “Notification form of risk and child abuse”, that all autonomous regions currently use [24]. The use of these notification forms promotes the systematic information gathering and the inter-institutional coordination, increasing the efficiency in the decision-making process. Each form consist of three copies: one addressed to the child record in the specific area [in this case, the health sector]; another for the social intervention, addressed to the primary care social services relevant to the ordinary action protocol or the corresponding entity for the minor protection in the case that the procedure requires urgent action; the last copy is addressed to the child abuse center in the autonomous region for statistical purposes. Once the necessary forms have been completed, there are two notification procedures, as we mentioned, ordinary and urgent protocol. In the ordinary protocol the information available about the case is reported to social services. Then, social services can evaluate initially if the intervention is made by them or if the case required to be derived to child protection services. On the other hand, the urgent protocol is activated in the event of reasonable indicators of the health and/or safety of the minor being at risk or being threatened and in the lack of a family or attachment figure that could take care of the minor. In these cases, regardless of the area where this situation is detected, child protection services are contacted directly. Dentists possessing suspicion or evidence of a child abuse case have then the duty to complete these notification forms and send them to the corresponding authorities. The professional would then also send the prescriptive lesion or medical report to the duty court or the prosecutor’s office. Furthermore, in the event of risk for the child integrity, the minor should be kept in the health center until, either social services or the corresponding police force, transfer the victim to a child protection center.
CONCLUSIONS
Lesions and diseases resulting from child abuse often appear in the oral region and, consequently, the dentist can play an essential role in their detection and notification. The most common psychological sign of child abuse in the dentist-patient relationship is the fear of the dentist or dental phobia. Dentists face important barriers in the detection and notification of child abuse including: the lack of training in the subject, the fear of a wrong suspicion, the professional impact in the professional practice, the fear of negative consequences in the minor, the fear of violence against the professional, the unawareness of the required documents and processes and the fear of a court case. There is a high discrepancy in the figures of suspected child abuse cases and the reports created by dentists. Consequently, it is necessary to train the professionals and establish protocols of action. The dentist is legally obligated to notify social services, the child protective services and/or the judicial system.

