










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
In Spain [1] and other countries of the European Region of the World Health Organization (WHO) [2] oral health has been reported as poorer in the immigrant child population than in the native population and the need for dental care was considered one of the key problems among the immigrant child population. Spain is the fourth country in the European Union that is home to the largest number of immigrants in the last 25 years [3] and Latin American immigrants, defined by their origin and not by access to Spanish nationality, are the second-largest group [4].
In many Latin American countries, caries is considered a public health problem due to the high prevalence reported [5]. According to the World Dental Federation (FDI), caries is mainly due to exposure to sugar and the lack of effective prevention and limited access to oral care, in addition to other risk factors [6]. Among the risk factors, it has been observed that caries is a disease associated with social vulnerability and deprivation and that there are numerous environmental, family and individual factors that contribute to the high prevalence of untreated carious teeth in children who suffer abuse or are in a situation of social risk [7, 8, 9, 10].
The objective of this study is to investigate the prevalence of untreated dental caries in immigrant children of Latin American origin who enter into the child protection system of the Autonomous Community of Aragon (Spain) and to observe if there is an association with demographic factors, body mass index (BMI), or vulnerability circumstances.
METHODS
Observational cross-sectional study. The data object of the study was obtained by reviewing the health and social records of all immigrant children of Latin American origin, with an age range between 6-17 years-old, who entered residential care of the child protection system of the Autonomous Community of Aragon (Spain) during the period 2000-2019.
The Social Services Institute of Aragon is, by law, the competent body of the child protection system in the Autonomous Community of Aragon [11]. This institution is the one that compiled their records and directed the protection measures assessed their vulnerability conditions [12].
A standard anthropometric and oral evaluation by healthcare professionals, together with the recollection of their demographic data, was carried out as these children accessed the welfare system.
For anthropometric evaluation, weight was recorded as the average of two determinations using a Seca 799 electronic column scale, with an accuracy of 100 g, and height was recorded as the average of two measurements with a stadiometer built into the scale with the child in an erect position to the nearest millimeter. The same explorer made all measurements. To define overweight and obesity, the BMI (weight/height squared) was calculated and to interpret its value, the specific cut-off points for age and sex prepared by Cole et al., and proposed by the International Obesity Task Force (IOTF) [13].
For oral evaluation, the WHO standardized protocols and forms [14] and the FDI notation were used [6].
According to FDI two-digit tooth numbering system, in permanent teeth, the 1st digit refers to the quadrants of the mouth (1, upper right; 2, upper left; 3, lower left; 4, lower right) and the 2nd digit refers to the teeth (1, central incisors; 2, lateral incisors; 3, canines; 4, 1st premolars; 5, 2nd premolars; 6, 1st molars; 7, 2nd molars; 8, 3rd molars). In deciduous teeth, the 1st digit refers to the quadrants of the mouth (5, upper right; 6, upper left; 7, lower left; 8, lower right) and the 2nd digit refers to the teeth (1, central incisors; 2, lateral incisors; 3, canines; 4, 1st molar; 5, 2nd molar) [6].
To perform the oral examination, among other instruments, plane mouth mirror Cone Socket#5 and metallic periodontal probes with ball tip conforming to WHO specifications were used. A tooth was considered present in the mouth when any part of it was visible. The criteria for diagnosing a tooth status and the coding were as follows. Sound crown (A, deciduous tooth; 0, permanent tooth): when shows no evidence of treated or untreated clinical caries. Sound root (0): when it is exposed and shows no evidence of treated or untreated clinical caries. Carious crown (B, deciduous tooth; 1, permanent tooth): when a lesion in a pit or fissure, or on a smooth tooth surface, has an unmistakable cavity, undermined enamel, or a detectably softened floor or wall. Carious root (1): when a lesion feels soft or leathery on probing with the examination. Filled crown, with caries (C, deciduous tooth; 2, permanent tooth): when it has one or more permanent restorations and one or more areas that are decayed. Filled root, with caries (2): when it has one or more permanent restorations and one or more areas that are decayed. Filled crown, with no caries (D, deciduous tooth; 3, permanent tooth): when one or more permanent restorations are present and there is no caries anywhere on the crown. Filled root, with no caries (3): when one or more permanent restorations are present and there is no caries anywhere on the root. Missing tooth, due to caries (E, deciduous tooth; 4, permanent tooth): when that have been extracted because of caries and are recorded under coronal status. Permanent tooth missing due to any other reason (5, permanent tooth): when teeth deemed to be absent congenitally or extracted for orthodontic reasons or because of periodontal disease, trauma, etc. Fissure sealant (F, deciduous tooth; 6, permanent tooth): for teeth in which a fissure sealant has been placed on the occlusal surface, in pits or for teeth in which the occlusal fissure has been enlarged with a rounded or “flame-shaped” bur, and a composite material placed. Fixed dental prosthesis abutment, special crown or veneer (G, deciduous tooth; 7, permanent tooth): when a tooth forms part of a fixed bridge abutment [14].
The following demographic variables were analyzed: countries of origin, two age groups (6-13 years-old and 14-17 years-old) and four generational groups (generation 2, children of immigrants born in Spain; generation 1.75, children of immigrants born in origin who arrived in Spain between the ages of 0-5 years-old; generation 1.5, those arriving between the ages of 6-12 years-old; generation 1.25, those arriving between the ages of 13-17 years-old) [15].
Statistical analysis. The data obtained from the social and health records were entered into an Excel® sheet. The arithmetic mean and standard deviation (SD) of the children's age and BMI and the percentages of the variables under study were calculated. Statistical analyses were performed with the Social Science Statistics v.2018® program. For the comparison of independent means, the two-tailed T-test was used, with a significance level of p<0.01. For the comparison of population proportions, the two-tailed Z test was used, with a significance level of p<0.01.
RESULTS
During the period 2000-2019, 231 children of Latin American origin with an age range between 6-17 years-old were admitted to residential care of the child protection system of the Autonomous Community of Aragon (Spain). The mean ± SD age was 13.6 ± 3.8 years and 55.8% were women.
Table 1 details, and compares by sex, the demographic variables, and the countries of origin of the sample of Latin American children in the protection system of Aragon. No significant differences were observed in terms of sex, age, and age groups. Regarding the generational groups, only 7.4% belonged to the second-generation and a statistically significant difference was observed in favor of the male of the 1.75 generation (p=0.004). The countries with the highest representation in the sample were Ecuador, Colombia, the Dominican Republic, and Brazil, comprising 69.3% of the total. No significant differences by sex were observed between the countries of origin.
Table 1. Demographic variables and countries of origin of 231 Latin American children in the child protection system of Aragon (Spain)
* p<0.01
Table 2 details, and compares by sex, the prevalence of untreated dental caries, overweight and obesity, and the vulnerability conditions in the sample of Latin American children at the time of entry into the protection system of Aragon. The prevalence of untreated dental caries was 16.5%, with no significant difference by sex. The prevalence of overweight and obesity was 32%, with no significant difference by sex. The most prevalent vulnerability conditions were parental inability to control child behavior and physical abuse, involving 62.8% of cases. Note that in 14.7% of children there were two or more vulnerability conditions. Only sexual abuse was significantly higher in women (p=0.004).
Table 2. Prevalence of untreated dental caries, overweight/obesity, and vulnerability conditions in 231 Alatin American children in the child protection system of Aragon (Spain)

Investigation of body mass index according to IOFT cut-off points. b In 34 (14.7%) children there were two or more vulnerability conditions. c Temporary or permanent (due to death, incarceration, physical illness, mental illness, drug addiction, or causes of a similar nature, together with the absence of relatives taking care of the child). * p<0.01
Table 3 compares the presence or absence of untreated dental caries with the demographic variables and the countries of origin of the sample of Latin American children in the protection system of Aragon. The presence of untreated dental caries was significantly higher in children of the age group 6-13 years-old (p<0.001) and those belonging to the second-generation (p=0.004) and was higher, but without statistical significance in children from Ecuador and the Dominican Republic. The absence of untreated dental caries was significantly higher in children of the age group 14-17 years-old (p<0.001) and those from Colombia (p=0.006).
Table 3. Comparison of the prevalence of untreated dental caries with the demographic variables and countries of origin of 231 Latin American children in the child protection system of Aragon (Spain)
* p<0.01
Table 4 compares the presence or absence of untreated dental caries with BMI and the vulnerability conditions of the sample of Latin American children in the protection system of Aragon. The presence of untreated dental caries was higher and statistically significant in children whose vulnerability condition was the temporary or definitive parental inability to provide child welfare (p=0.009) due to death, incarceration, physical illness, mental illness, drug addiction, or causes of a similar nature, together with the absence of relatives taking care of the child. The absence of untreated dental caries was significantly higher in children whose vulnerability condition was the parental inability to control child behavior (p=0.001). No significant differences were observed between the presence or absence of untreated dental caries and nutritional status according to BMI.
Table 4. Comparison of the prevalence of untreated dental caries wth BMI and the vulnerability conditions of 231 Latin American children inthe child protection system of Aragon (Spain)
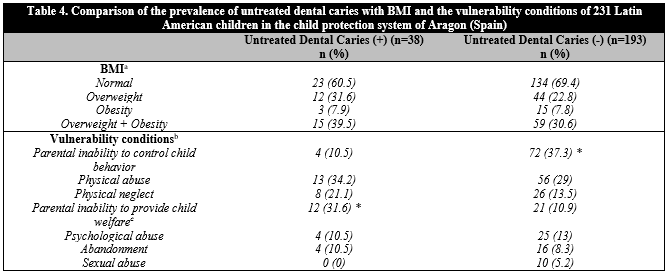
a Investigation of body mass index according to IOFT cut-off points. b In 34 (14.7%) children there were two or more vulnerability conditions. c Temporary or permanent (due to death, incarceration, physical illness, mental illness, drug addiction, or causes of a similar nature, together with the absence of relatives taking care of the child). * p<0.01
DISCUSSION
According to FDI, untreated dental caries is the most widespread chronic disease in the world. Figure 1 shows the epidemiological distribution of dental caries in Latin America, noting that the DMFT index in 12-year-olds is high or moderate in a significant number of countries [6]. Ecuador and the Dominican Republic are two of the countries with a DMFT index high, and in this study children from these countries showed the highest prevalence of untreated dental caries.
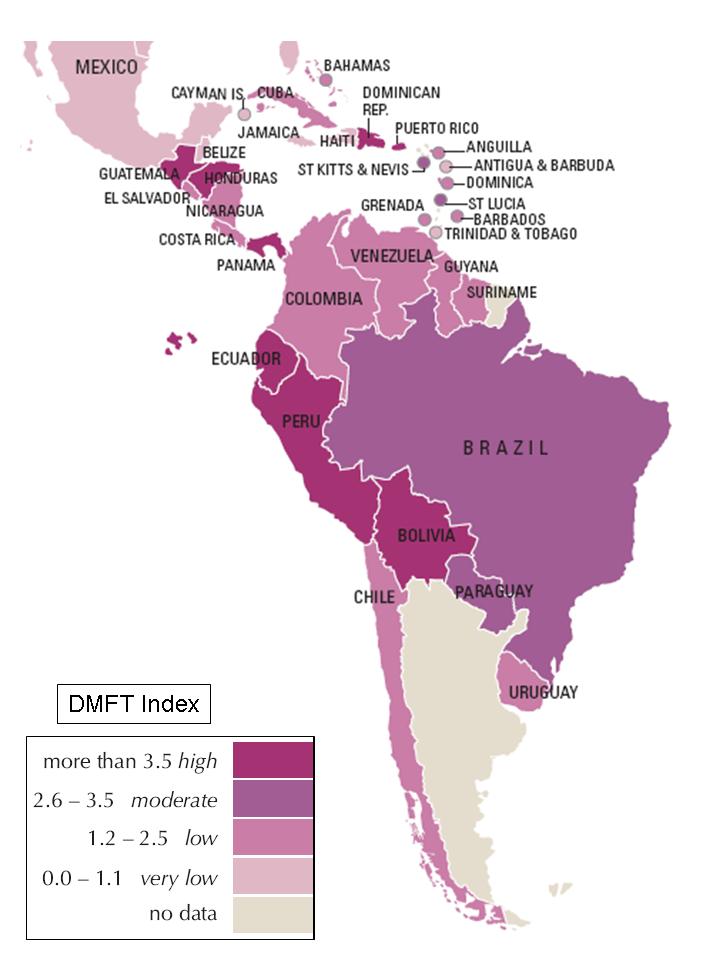
The DMFT index. Average number of decayed (D), missing (M), and filled (F) teeth in 12-year-olds. Latest available data 1994-2014. Source: FDI World Dental Federation; 2015.
Figure 1. Dental caries in Latin America.
In Spain, the Oral Health Survey carried out in 2015 showed a prevalence of untreated dental caries in 12-year-old children of 14.6% [16]. In the Autonomous Community of Aragon, the results of a study of the Child and Youth Oral Care Program carried out in 2011 showed a prevalence of untreated dental caries in 12-year-old children of 8.6% [17]. In the studied sample of children of Latin American origin, the prevalence of untreated dental caries was 16.5%, slightly higher than that of Spanish children but almost twice higher than that of children in the host community, noting a positive association with the age group of 6-13 years-old and with those belonging to the second-generation, that is with those born in Spain. Several studies have highlighted that the school-age population that migrated with their families to European countries or with the antecedent of migration of their parents (second-generations) generally has a higher prevalence of caries than that of the host population. The highest prevalence of caries in this population seems to be related to native cariogenic dietary habits, cariogenic diets in host countries, inadequate dental care, and nutritional deficiencies [1, 2, 18, 19, 20, 21, 22].
According to FDI, caries is mainly due to exposure to sugar [6], and recent studies point in particular to the intake of added sugars [23, 24]. Furthermore, experts link excess sugar consumption with overweight and obesity [25]. According to this association, overweight and obese children should have a higher prevalence of caries. Various studies show that immigrant children and children with lower socioeconomic status have a higher risk of developing overweight and obesity compared to other children [26, 27, 28, 29]. Specifically in Latin American children, a higher prevalence of risk factors related to the development of overweight and obesity has been demonstrated, among which the high consumption of sugary drinks and fast foods rich in carbohydrates stands out [30].
In this study, the prevalence of overweight and obesity in the sample of first and second-generation Latin American children in the child protection system of Aragon was 32%. This proportion is higher than that observed in the study performed in 2014 by the Ministry of Health, Social Services, and Equality on the prevalence of overweight and obesity in first and second-generation Latin American children in Spain, estimated at 22.3%. Both proportions are higher than those observed in their native peers, which was 16.9% [31]. Despite the high prevalence of overweight and obesity observed in the sample of Latin American children, no positive association was found in this study between the presence of overweight and obesity and the existence of untreated dental caries. The absence of an association between caries and overweight and obesity would be according to what was noted in most of the studies of a systematic review of the literature and meta-analysis [32, 33, 34].
Concerning the relationship between the vulnerability conditions that led these children to their placement in the child protection system of Aragon and the presence of untreated dental caries, the temporary or permanent parental inability to provide child welfare showed a positive association. This association agrees on studies that recognize that untreated dental caries is a disorder linked to socio-family vulnerability and deprivation [7, 8, 9, 10].
CONCLUSIONS
The prevalence of untreated dental caries in the sample of Latin American children in the child protection system of Aragon (Spain) was higher than that of autochthonous children. Ecuador and the Dominican Republic were the countries of origin with the highest prevalence.
The presence of untreated dental caries showed a positive association with the age group 6-13 years-old, the second-generation, and the temporary or permanent parental inability to provide child welfare due to death, incarceration, physical illness, mental illness, drug addiction, or causes of a similar nature, together with the absence of relatives taking care of the child.
The prevalence of overweight and obesity was high, but no association was observed between the presence of untreated dental caries and nutritional status according to BMI.
We observe either that, besides cariogenic dietary habits acquired in their native community or their foster one, socio-family vulnerability and deprivation play an essential role in the high prevalence of untreated dental caries.

