










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Suicide makes up one of the most relevant social issues in modern societies. According to the World Health Organization (2018), more than 2,000 people die from suicide every day. In Spain, 65,778 people died by suicide between 2000 and 2018, and 3,539 deaths by suicide were registered in 2018 (Instituto Nacional de Estadística, 2019). Currently, suicide is the leading external cause of death in Spain (Santurtún et al., 2017). Consequently, a substantial number of studies analysing suicide from different perspectives have been carried out (Goñi-Sarries et al., 2019; Mejias-Martin et al., 2018; Pérez et al., 2019; Santurtún et al., 2018; Voltas et al., 2020).
Suicidal ideation is defined by the Centers for Disease Control (CDC) as “thinking about, considering, or planning suicide” (Crosby et al., 2011). Several theories have been developed to explain suicidal ideation (Joiner, 2005; Klonsky & May, 2015; O’Connor, 2011): the Interpersonal Theory of Suicide, the Integrated Motivational-Volitional Theory, and the Three-Step Theory. All of them combine emotional factors to explain suicide. The Interpersonal Theory of Suicide (Joiner, 2005) considers the combination of personal perception of alienation from others and the feeling of low belonging with perceived burdensomeness. The Integrated Motivational-Volitional Theory (O’Connor, 2011) contemplates the feelings of defeat and humiliation with entrapment. Finally, the Three-Step Theory (Klonsky & May, 2015) takes into account the feeling of psychological pain with hopelessness.
From a suicide prevention perspective, crisis helplines can facilitate the identification of persons at risk for suicide (Gould et al., 2016; Joiner et al., 2007; Witte et al., 2010). Some helplines are specifically focused on suicide (Pil et al., 2013; Ramchand et al., 2017); others provide counselling for any type of emotional and/or mental problem (Bassilios et al., 2015). All helplines play an important role in preventing suicide (Tyson et al., 2016). The rates of suicidal ideation in suicide-specialized helplines range from 21% to 29% (Gould et al., 2013; Lifeline Australia, 2019; Ramchand et al., 2017). In non-specialized helplines, the rates range from 0.45% to 6% (Barber et al., 2004; Sindahl et al., 2019; Till et al., 2013; Villanueva et al., 2019).
Teléfono de la Esperanza (TE) is the main Spanish helpline providing telephone listening and support for callers in crisis situations. TE is available across the entire country, is not only focused on suicide, and offers counsellors who are specifically trained in active listening to provide emotional support. In a recent study carried out on this helpline with 10,765 callers (Villanueva et al., 2019), 1.87% of the sample (n = 201) presented with suicidal ideation. However, no more data on this topic are available, and more studies are needed in Spain.
Not all callers with suicidal ideation present with suicide attempts (López-Goñi et al., 2019). Suicidal behaviour is considered a continuum that begins with suicidal ideation and may continue with planning, attempts, and suicide completion (Thompson et al., 2012). Moreover, a higher suicidal ideation severity is associated with more severe suicide attempts with lethal results (Shelef et al., 2019). In this sense, the study to validate the C-SSRS scale found that the two highest levels of suicidal ideation present the highest probability of attempting suicide (Posner et al., 2011). From a prevention perspective, early identification of suicidal ideation and specific characteristics related to suicidal ideation severity are crucial to develop specific prevention strategies for suicide.
Studies carried out on the general population have shown that suicidal ideation severity is related to younger individuals (Bernal et al., 2007; Gabilondo et al., 2007; Thompson et al., 2012), specifically people under 50 years old (Miret et al., 2014). On the other hand, the ODIN study, involving five European countries, showed that loneliness, lack of support for events, living in urban areas, and depression were directly associated with severe suicidal ideation (Casey et al., 2006). However, no previous studies identifying factors related to suicidal ideation severity among helpline callers have been carried out.
Regarding characteristics of helpline callers, some studies have shown that the rate of suicidal ideation is higher in women than in men. Moreover, suicidal ideation mainly affect single callers, with a mean age ranging from 30 to 49 years old (Gould et al., 2007; Villanueva et al., 2019). From a gender perspective, some differences have also been found in callers with suicidal ideation. Specifically, women are older, less frequently partnered, and not employed in a higher proportion than men. On the other hand, men present more frequently depression, hopelessness, and lack of hope for the future, as well as a higher alcohol and/or drug abuse (Villanueva et al., 2019).
Some studies have shown a relationship between suicidal behaviour and time characteristics (Marco et al., 2017; Santurtún et al., 2018; Santurtún et al., 2017; Woo et al., 2012). Specifically, suicides peak high in spring and early summer, mainly if the weather is cloudy. Regarding helpline callers, the study of Villanueva et al. (2019) found that most of the ideators called in summer or spring, on weekends, and in the evening or night-time.
Due to the relevance of suicidal ideation severity in suicide behaviours and the few studies carried out to date identifying predictors of suicidal ideation severity, the main aims of this study were: 1) to identify callers with severe suicidal ideation and, as a consequence, with a higher risk of suicide; 2) to explore differential characteristics (sociodemographic, call timing, risk factors, and suicidality variables) between callers with severe and low-moderate suicidal ideation; and 3) to predict severe ideation risk among callers with suicidal ideation. The main hypothesis of this study is that relevant differences between callers with severe and with low-moderate suicidal ideation will be found. Specifically, according to the literature, being under 50 years old, loneliness, and depression will be predictors of severe suicidal ideation. This is the first study to analyse the specific characteristics associated with suicidal ideation severity among callers to a helpline.
Method
The protocol for this study was approved by the ethics committees of the Public University of Navarra (PI-005/16) and the Teléfono de la Esperanza (03/2016).
Participants
The initial sample consisted of 26,032 callers (16,151 women, 62%; 9,881 men, 38%) to Navarra (Spain) TE telephone helpline from February, 1st 2016 to June, 30th 2019. TE is the best-known Spanish helpline aimed at providing telephone counselling to people seeking help for any type of problem related to emotional health. This research includes calls received in the helpline in the region of Navarra (Spain).
The admission criteria were as follows: a) calling the TE helpline to seek help; b) presenting with suicidal ideation; and c) not presenting a suicide attempt in progress. Using these criteria, 735 callers presented with suicidal theme. However, 171 callers could not be assessed with the assessment tool used in this study (ATENSIS; Villanueva, 2014). In these cases, counsellors identified suicidal ideation, but considered that they were not sufficiently trained to use ATENSIS. Moreover, 20 callers were in a suicide attempt in progress. Therefore, 544 people were included in the study (Figure 1).

The mean age of the 544 participants included in the study was 46.6 years (SD = 13.5 years). The sample included 281 (51.7%) women and 263 (48.3%) men. Most of the callers were Spanish (94.9%), 52% were single, and 47.2% were unemployed (Table 1).

Instruments
ATENSIS (Villanueva, 2014) is an assessment digital tool designed to: a) collect information related to suicidal ideation among callers to telephone helplines; b) classify the risk of suicide in 4 levels (low, moderate, high, and very high); c) offer different orientations to cope with the problem according to the risk observed; and d) develop a safety plan based on callers’ characteristics.
ATENSIS was developed by considering empirical data describing suicide risk assessment and risk factors for suicide (Oquendo et al., 2003; Posner et al., 2011). Specifically, ATENSIS includes the Columbia-Suicide Severity Rating Scale (C-SSRS; Posner et al., 2011) and considers the Interpersonal-Psychological Theory of Suicidal Behaviour (Joiner, 2005) and the Integrated Motivational-Volitional Model of Suicidal Behaviour (IMV; O’Connor, 2011). Questions are adapted for use in a telephone interview format, using the technique of active listening that allows delving into each variable analysed and making a therapeutic intervention. For example, when faced with feelings of failure, the counsellor may ask questions such as “Despite your feeling of failure, can you tell me one thing in your life that you are proud of? What personal qualities helped you achieve it? Were you surprised to discover that you were capable?”.
This instrument identifies behaviours that may be indicative of an individual’s intent to take his life. Specifically, the instrument consists of 4 sections: sociodemographic variables, telephone call timing characteristics, suicide risk factors (physical disease, mental disorder, life crisis, loneliness, capability of suicide attempt), and suicidality variables (suicidal ideation and suicidal behaviour). ATENSIS identifies 5 levels of suicidal ideation severity (wish to be dead, suicidal thoughts, suicidal thoughts with method, suicidal intent without specific plan, suicidal intent with specific plan) according to the C-SSRS (Posner et al., 2011). Moreover, ATENSIS provides the 4 levels of risk of suicide not only from suicidal ideation severity, but also from other variables related to suicidality, such as preparatory behaviours, previous attempts, and the risk factors identified. A summary of the assessment process of ATENSIS for the suicide risk can be found in Figure 2.

Design
A retrospective cross-sectional study using a sample of callers to a helpline was carried out.
Procedure
Telephone counsellors were trained in the use of ATENSIS. Specifically, counsellors were instructed not to use the questionnaire as an interview but to conduct calls according to the centre’s protocol, which is based on active listening, and to use the digital questionnaire to collect information about several variables related to the caller’s risk factors of suicide. The training for counsellors was carried out in face-to-face sessions, twice a year.
Calls were eligible for inclusion in the study if the counsellor deemed suicidal ideation to be present at any time during the call. Once suicidal ideation was detected, the counsellor directed the conversation to explore and fulfil the areas included in ATENSIS.
After fulfilling the ATENSIS protocol, the caller’s suicidal ideation severity was classified into two categories: severe (including “suicidal intent without a specific plan” and “suicidal intent with a specific plan” according to C-SSRS levels 4 and 5) and low-moderate (including “wish to be dead”, “suicidal thoughts” and “suicidal thoughts with a method” according to C-SSRS levels 1, 2 and 3). Callers from both categories were compared among all the variables studied. The severity ideation was dichotomized because the help intervention in TE is decided depending on these two categories.
Data Analysis
The distribution of missing data was studied, and no significant differences were found between subjects with and without available data in each of the variables studied. Therefore, the pairwise deletion method was selected; this method involves analysing the available cases in each variable.
Descriptive analyses were performed on all the variables. Specifically, N values, means, and standard deviations were calculated.
In the bivariate analyses between men and women, a χ2 or Student’s t-test for independent samples was used, depending on the nature of the variables analysed. A difference of p < .05 was considered significant. To account for the use of multiple comparisons and reduce the risk of type I error, Bonferroni adjusted p-values were used.
Regarding multivariate analyses, a logistic regression analysis (forward conditional method) was conducted to determine which specific factors were more relevant in differentiating between callers with a severe level of suicidal ideation severity and callers with low-moderate severity. Only variables with statistically significant differences were included as independent variables. The variable entry criterion was set to .05, and the variable retention criterion was set to .10. Moreover, the Hosmer-Lemeshow test was used to assess the goodness of fit of these models. All statistical analyses were performed using SPSS (version 25.0) software.
Results
Prevalence and Severity of Suicidal Ideation among Callers to the Telephone Helpline
The presence of some type of suicidal ideation (without suicide attempt in progress) was identified in 715 cases (386 women and 329 men) of the 26,032 telephone calls received at the TE helpline during the study period. Therefore, the identified prevalence rate of suicidal ideation among telephone callers was 2.8%, with statistically significant differences (χ2 = 20.3, p = .000) between men (3.3%) and women (2.4%).
Regarding severity, the distribution of the sample with suicidal ideation was as follows: wish to be dead (n = 107, 19.7%), suicidal thoughts (n = 276, 50.7%), suicidal thoughts with a method (n = 97, 17.8%), suicidal intent without a specific plan (n = 29, 5.3%), and suicidal intent with a specific plan (n = 35, 6.4%). Therefore, 64 (11.8%) of the sample presented with severe suicidal ideation, and 480 (88.2%) presented with low-moderate severity.
Differences in Callers with Severe and Low-Moderate Suicidal Ideation Severity
Sociodemographic characteristics. A comparison of the sociodemographic characteristics between both groups is presented in Table 1. The results showed statistically significant differences only in age.
Specifically, callers under 50 years old showed a greater severity in suicidal ideation than those over 50.
However, when a gender-based analysis was carried out, the age difference was only found in men (χ2 = 11.2, p = .001). Women did not show a statistically significant difference (χ2 = 0.8, p = .369).
Telephone call timing characteristics. Most of the calls were made in summer or spring, on weekends, and in the evening or night-time. No differences between severe and low-moderate groups were found with respect to the time of the call (Table 2).

Risk factors. Regarding the five risk factor categories explored with ATENSIS, 95.8% of callers with suicidal ideation presented with some type of life crisis, 76.1% with a diagnosed mental disorder, 66.4% with loneliness, and 16% with a physical disease. Moreover, 34.9% of the sample presented some risk factors that showed an acquired capability to attempt suicide according to Joiner’s (2005) interpersonal theory of suicide (Table 3).
Table 3. Comparison of Risk Factors

Note. In each category, the total number of people with risk factors is lower than the sum of people for the variables of the category because some people present with more than one risk factor.Bonferroni adjusted p = .025.
The comparison of risk factors between both groups showed statistically significant differences for two categories (loneliness and attempt capability) and seven variables. Specifically, attempt capability was higher in callers with severe suicidal ideation and loneliness in the low-moderate group. Regarding specific variables, the group with severe suicidal ideation showed a greater rate of hopelessness and lack of life sense as well as reported either several lifetime suicide attempts or one lifetime suicidal attempt and non-suicidal self-injuries. On the other hand, the rate of loneliness was higher in people with low-moderate severity than in people with severe suicidal ideation.
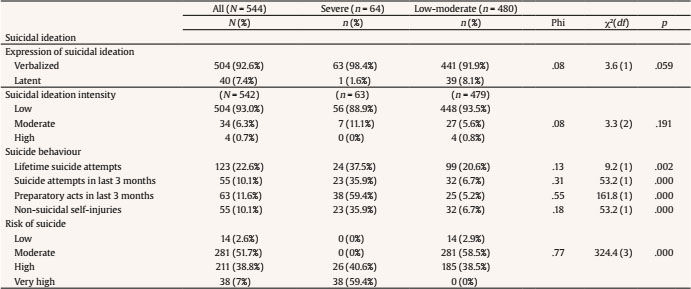
Suicidality variables. Regarding suicidality variables, most of the sample verbalized suicidal ideation and presented a low suicidal ideation intensity. The results of the comparisons between groups showed that callers with severe suicidal ideation presented more suicide behaviours and a higher risk of suicide than callers with low-moderate severity (Table 4).
Multivariate Analysis for Differentiating between Callers with Severe and Low-Moderate Suicidal Ideation Severity
The results of the logistic regression analyses showed that the main variables related to the presence of severe suicidal ideation were the following: preparatory acts in the last 3 months, suicide attempts in the last 3 months, non-suicidal self-injuries, lack of life sense, age (< 50 years old), and hopelessness. These variables correctly classified 91.9% of cases (Table 5).

Discussion
This is the first study analysing the specific characteristics associated with suicidal ideation severity among callers to a helpline. The differences between callers with severe and low-moderate suicidal ideation were explored. The results from this study show that the prevalence rate of suicidal ideation among telephone callers was 2.8%, which is within the range of the prevalence rate found in other studies (Barber et al., 2004; Till et al., 2013; Villanueva et al., 2019). Most suicidal ideators presented with low-moderate severity, while 11.8% of the sample showed severe suicidal ideation. No previous comparable studies could be found to test these figures.
The identification of the specific differential variables associated with severe suicidal ideation is essential to intervene in them. In this study, comparisons between both levels of suicidal ideation severity showed significant differences in several variables. Regarding sociodemographic characteristics, male callers with severe suicidal ideation were younger than those with low-moderate suicidal ideation. Specifically, men under 50 years old were associated to a greater extent with severe ideation than those over 50, in line with a previous study carried out in Spain (Miret et al., 2014). Other previous studies have also found that age is a factor associated with suicidal ideation (Bernal et al., 2007; Gabilondo et al., 2007; Thompson et al., 2012). For example, the results of the study of Thompson et al. (2012) indicated that the age of onset of suicidal ideation is inversely correlated with the severity of suicidal behaviour.
Previous studies have found a relationship between suicidal behaviour and telephone call timing characteristics (Marco et al., 2017; Santurtún et al., 2018; Santurtún et al., 2017; Villanueva et al., 2019). In this study most of the calls were made on weekends, and in Spring/Summer, in line with previous studies. However, no timing differences between severe and low-moderate suicidal ideation callers were found. Anyway, call timing should be considered to coordinate resources, mainly the assignment of trained counsellors, in moments in which suicidal calls peak high.
One of the core results of this study is that previous suicide behaviours (both recent preparatory acts and recent suicide attempts) and non-suicidal self-injuries are the main predictors of severe suicidal ideation. There is ample evidence regarding the predictive effect of previous suicide attempts on a new suicide attempt (Ayuso-Mateos et al., 2012; Kann et al., 2000; Shelef et al., 2019; Yoshimasu et al., 2008). Moreover, non-suicidal self-injuries have also been associated with severe ideation, confirming the importance of considering these behaviours in callers with suicidal ideation (Brausch & Boone, 2015; Klonsky et al., 2013; Tyson et al., 2016; Whitlock et al., 2013). The identification of these variables, together with a lack of life sense, hopelessness, and an age below 50 years, should alert the counsellor to the presence of severe suicidal ideation and the need for a rapid and accurate intervention.
A specific result of this study is that none of the factors associated with severe suicidal ideation are related to a diagnosis of a mental disorder. In this study, depression is the leading mental disorder (42.6% of cases) informed by callers with suicidal ideation, in line with previous studies (Casey et al., 2006; van Duijn et al., 2018; Villanueva et al., 2019). However, depression occurs equally among those with mild-moderate ideation and those with severe ideation. Thus, depression is not related to suicidal ideation severity. Our study shows the relevance of emotional variables also found in previous studies, such as loneliness (Casey et al., 2006) or a lack of life sense and hopelessness (Thompson et al., 2012). Consequently, beyond psychopathological characteristics, patients with severe suicidal ideation present with emotional problems. These dynamic risk factors can be modified and should constitute a priority goal of intervention for prevention and treatment programmes.
Although the main goal of this study was to identify factors related to severe ideation, low-moderate suicidal ideation should not be underestimated. The concept of suicidal process implies a progression from a behaviour with low suicidal ideation to a completed suicide. Early forms of the suicidal process are associated with the ultimate seriousness of suicidal behaviour (Thompson et al., 2012). Therefore, low-moderate suicidal ideations should not be associated with a lower need for intervention. A prevention approach during the first stages of the suicide continuum becomes crucial.
Some limitations of the present study must be highlighted. First, the exploratory and descriptive nature of this study implies that the specific causal role of the variables explored cannot be established. Second, this research included callers to a specific telephone helpline in a region of Spain, which may create a bias that prevents us from generalizing results to other helplines in other contexts. Third, a potential self-report bias in assessing suicidal callers might have occurred. This was a general crisis helpline, and not all callers were specifically asked about suicide. Consequently, some suicidal callers may have been missed. Finally, in this study, the relationship between the severity of suicidal ideation and suicide attempts was not considered. Future research should consider the differences between ideators who attempt suicide and those who do not.
This is the first study to investigate specific differences between helpline callers with severe and low-moderate suicidal ideation. According to the results obtained, a systematic screening of severity in callers to helplines with suicidal ideation should be implemented. The identification of specific risk factors of suicidal ideation severity would allow carrying out psychological interventions with these persons. Due to the low number of papers on this topic, more research is needed.

