










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
The prevalence of childhood obesity has increased across Europe 1 and it is now a recognized public health problem. According to the World Health Organization (WHO), obesity is a chronic disease that has reached epidemic proportions; in some parts of the world, 17.6% of children under five years of age are obese 2. Recent studies in different countries have shown 10% of all school-age children to have excess body fat, increasing their risk of developing chronic diseases 3. Indeed, overweight/obesity has become one of the most common nutritional problems among children of developed countries, though it is by no means limited to them 3) (4.
Obesity is increasingly affecting all age groups and is associated with increased morbidity and mortality 5) (6. The complications of obesity most commonly appear during adulthood, although nowadays they are also being detected in childhood. Many factors are associated with its appearance; genetic, sociodemographic (including sex and level of parental education) and lifestyle factors are all involved, including the duration of breastfeeding, the daily taking of breakfast, getting enough sleep, time spent in front of monitors 7 and the amount of physical activity undertaken 6) (8. Tackling obesity is commonly one of the best set out objectives in healthcare strategies 9, but understanding the factors that encourage its appearance is vital if it is to be prevented 10) (11.
The aim of the present work was to describe the prevalence of overweight and obesity in Spanish children (boys and girls) using data provided by the National Health Surveys (Encuestas Nacionales de Salud) of 1993-2011, and to determine the main socioeconomic and lifestyle factors influencing the appearance of these problems in 2011.
METHODS
DESIGN
This descriptive, cross-sectional study examined data provided by the 1993-2011 Spanish National Health Surveys (Ministerio de Sanidad, 1993; 1995; 1997; 2001; 2003; 2006; 2011). These surveys question members of the public regarding their health status and provide information on perceived morbidity, risk factors, the use of health services, and the following of preventive practices.
SUBJECTS
The data examined were those of children aged 2-15 years, chosen by stratified multi-stage sampling. Entries for children of this age were stratified by region, then by province (as conglomerates), then by "habitat" (urban or rural area). Schools were then chosen at random within these "habitats", then classes by age group between 2 and 15 years, followed by random sampling of the children in these age groups. The final sample size (which included data from only fully completed survey questionnaires) was n = 23,237 (11,663 girls and 11,574 boys). The children's heights and weights (as recorded by their parents/guardians) were used to calculate their body mass indices (BMI). Children with a BMI ≥ 25 were deemed overweight, and those with a BMI ≥ 30 were deemed obese.
STATISTICS
The prevalence (with 95% confidence intervals) of overweight and obesity was analyzed for each survey year separately.
The association of overweight and obesity with each independent variable as measured in 2011, i.e., sex, age at the time of the survey, recommended number of hours of sleep (3-4 years 12 h, 4-5 years 11 h, 5-11 years 10 h and 11+ years 9 h) 10) (12) (13, physical activity (measured as yes/no), hours spent watching TV or using other monitors (< 2 or ≥ 2 h per day) 14, having been breast-fed for the first three or six months (yes/no for each), taking breakfast daily (yes/no), level of education of head of family (no education or obligatory schooling, school baccalaureate or technical award, higher education) 15) (16, was examined using the Chi-squared test. Significance was set at p ≤ 0.05. Adjusted odds ratios (OR) were obtained by bivariate and consequent multivariate regression analysis. All calculations were performed using SPSS v.21.0 for Windows.
RESULTS
Table I shows the prevalence of childhood overweight and obesity for girls and boys over the study period. In 1993, 7.0% of boys were overweight, but in 2011 this figure had risen to 13.2%; for girls, the figures were 6.0% and 10.2% respectively. In 1993, 13.8% of boys and 8.7% of girls were obese, while in 2011, 13.6% of boys and 9.9% of girls were obese. Overweight and obesity was consistently more common among boys than in girls.
Table I Prevalence of overweight/obesity in boys and girls, as recorded in different National Health Surveys (1993-2011)

n: sample size; CI: confidence intervals.
Table II reveals that, in 2011 (note that 2011 health survey data were used to determine all risk factor associations), those children who belonged to a family whose head had no or only low-level studies showed a higher prevalence of overweight (boys 13.2%, girls 7.4%) compared to those who had higher education (boys 19.1%, girls 9.0%) (p < 0.05 in all cases). Similar results were seen for obesity (boys 16.3% and girls 5.5% compared to 10.7 and 8.1%; p < 0.05 for the comparison between boys).
Table II Distribution of normal-weight, overweight and obesity with respect to sex and lifestyle variables according to the 2011 National Health Survey results
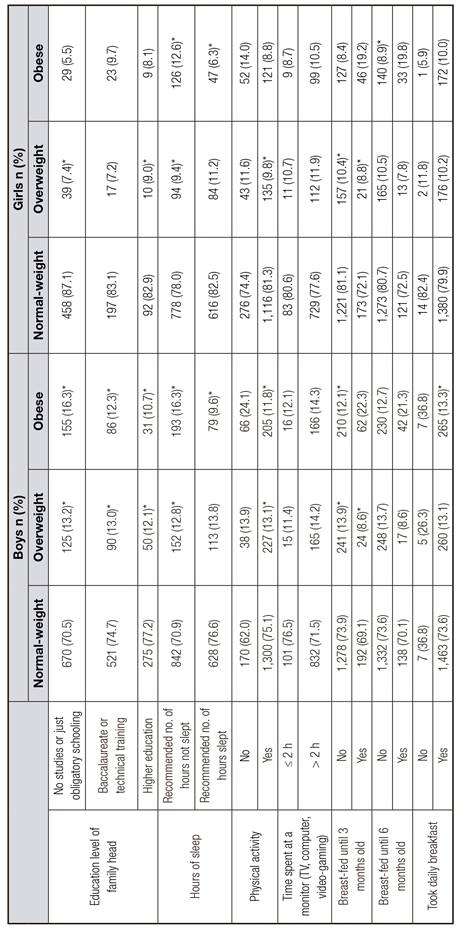
n: Sample size. *p < 0.05.
Those children who did not sleep the recommended number of hours were more commonly obese (boys 16.3%, girls 12.6%) than those who slept the recommended amount (boys 9.6%, girls 6.3%) (p < 0.05 both sexes). Those children who undertook some kind of physical activity were less commonly overweight (boys 13.1%, girls 9.8%) than those who undertook none (boys 13.9%, girls 11.6%) (p < 0.05 for both sexes); they were also less commonly obese (boys 11.8%, girls 8.8%) than those who undertook no physical activity (boys 24.1%, girls 14%) (p < 0.05 for the comparison between boys). No significant differences were seen between children who used monitors (TV, playing videogames, etc.) more than two hours per day compared to those who used them for less time, either in terms of overweight (boys 14.2%, girls 11.9% vs boys 11.4%, girls 10.7%) or obesity (boys 14.3%, girls 10.5% vs boys 12.1%, girls 8.7%).
Those children exclusively breast-fed for their first three months of life were less commonly overweight (boys 8.6%, girls 8.8%) than those who were not so fed (boys 13.9%, girls 10.4%) (p < 0.05 for boys and girls). No significant differences were seen between children who were exclusively breast-fed for the first six months of life and those who were not in terms of overweight (boys 8.6%, girls 7.8% vs boys 13.7%, girls 10.5%). No comparisons were made for obesity given the small sample size available, neither was any significant difference seen in terms of overweight between children who ate or did not eat breakfast (boys 26.3%, girls 11.8% vs boys 13.1% girls 10.2%).
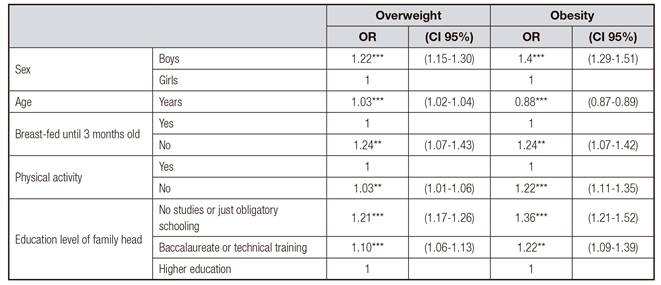
Table III shows the results of the multivariate analysis. Age, male sex, being breast-fed until three months, not undertaking physical activity, and the level of education of the head of the family were independently and significantly associated with being overweight. The same variables were independently and significantly associated with being obese.
DISCUSSION
The present results show that the prevalence of overweight and obesity increased over the study period in both boys and girls. In addition, overweight and obesity was consistently more common among boys.
The present prevalence data for 1997 were compared to those of the enKid study 16 which was performed in 1997-1998. The prevalence of overweight was higher in this latter study (boys 14.3%, girls 15.6%) than in the present work (boys 8.0%, girls 7.5%). In addition, the present prevalence data for 2011 were compared to those reported by the Aladino 2011 17. This latter study reported a higher prevalence of overweight (boys 22.9%, girls 17.4% vs the present boys 13.2%, girls 10.2%), but a lower prevalence of obesity (boys 7.7%, girls 4.7% vs the present boys 13.6%, girls 9.9%). These discrepancies might be due to differences in the methodologies employed.
According to the 2011 health survey results (used for all associations with lifestyle factors), the prevalence of overweight and obesity was higher among children of families whose heads were the least well educated. The enKid study reported similar results for obesity (15.6% vs 10.9% in families with the head in the highest education bracket) 16. Similarly, the Aladino 2011 study reported that, among normal-weight children, 58.5% of their mothers and 59.4% of their fathers had university studies, while among obese children only 14.6% of their mothers and 14.7% of their fathers had university studies. This might reflect a limitation of economic resources faced by families with low education levels, or their more limited knowledge of what makes a healthy diet, or perhaps a different aesthetic outlook 17.
Those children who slept the recommended number of hours for their age were less commonly obese than those who did not get enough sleep. Very few studies performed in Spain have examined the link between the number of hours spent sleeping and overweight/obesity. The Aladino 2011 study did report, however, results very similar to those of the present work: 10.7% of those who slept sufficient hours were obese, rising to 15.2% among those who did not, whereas in the present study these figures were boys 9.6% vs 16.3%, and girls 6.3% vs 12.6% 17.
No differences were seen in overweight or obesity between those children who spent under or over two hours per day using monitors. This is in contrast to that reported in other studies. For example, in Sweden, children who had a television in their bedrooms, or who watched television for more than two hours per day, were more likely to be overweight/obese (OR 1.26 and 1.55 respectively) 7. This discrepancy might be due to the small numbers of children in the present study who actually spent < 2 h per day in this activity.
The prevalence of obesity was lowest among those children who undertook physical activity (boys 11.8%, girls 8.8%), and highest among those who undertook none (boys 24.1%, girls 14.0%). Another paper reported similar results, with obesity more prevalent among those who undertook no physical activity (boys 21.7%, girls 9.8% vs boys 9.7%, girls 4.3% in those who did) 9. Other authors also report children who played sport to be less commonly obese than those who did not (10.3% vs 22.7%) 16. In the present work, children who spent more time in physical activity spent less time using monitors.
Overweight was less common among children who had been breast-fed until three months of age than in those not so fed. Similar results have been reported from Korea 18, and in an earlier systematic review of 300 articles from around the world 19. No significant differences were found for children who were/were not breast-fed until six months of age, perhaps due to the small sample size available for comparison.
Overweight was no less prevalent among children who ate breakfast (no result is available for obesity given the small numbers involved). In contrast, the AVENA study 20 reported that the habit of not taking breakfast was more common among children who were overweight or obese (normal weight children 5.9%, overweight children 11.6%, obese children 13.3%, p < 0.05). The Aladino 2011 study also reported similar results, with 3.1% of normal weight children and 4.2% of obese children not eating breakfast. Not taking breakfast might reflect a wider range of poor food habits, or might leave children hungry later in the day, leading to their eating with poorer control. The discrepancy with the present results is probably due to the low sample size available for those who took no breakfast 17.
CONCLUSIONS
The prevalence of obesity increased in Spain between 1993 and 2011, and was more common among boys than in girls over this study period. Child overweight/obesity was found to be more prevalent in families in which the head of the family had a low level of education. Breastfeeding for three months appears to reduce the prevalence of overweight, while undertaking physical activity reduces the prevalence of obesity.

