










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
Among the general population, mental health problems tend to be more common among women than men (Guimaraes et al., 2019). Furthermore, certain stages in the life cycle of women can facilitate the appearance of psychological problems, particularly the perinatal stage (Dunkel-Schetter, 2011). The perinatal stage encompasses the process of pregnancy and the year following birth (Yu et al., 2021). A period is characterised by a multitude of changes: physical, mental, social, cultural and established gender roles (Hoekzema et al., 2020).
Although the experience of maternity is usually associated with positive emotions, the perinatal stage may be extremely stressful (Geller, 2004). The most common symptomologies among pregnant women or new mothers are depression (10%-20%) and anxiety (25%-45%) (Viveiros & Darling, 2018). Other common symptoms during this period include excessive worry, uncertainty, and stress.
Although women in the perinatal stage generally receive regular care and attention from healthcare professionals, psychological problems during this stage remain underdiagnosed and undertreated in comparison to other stages in women's lives (Bina & Glasser, 2019). The lack of time, the associated stigma, or the lack of knowledge about perinatal depression and its consequences prevent these women from seeking help (Grissette et al., 2018). Also, there are several institutional barriers that can restrict access to health services, such as lack of human resources or inadequate training, lack of time for consultations, or simply lack of recognition of the problem by the health system (Prevatt & Desmasaris, 2018). Thus, identifying early indicators of perinatal depression is a crucial public health issue (NICE, 2014). Furthermore, beyond merely identifying psychological symptoms, promoting maternal well-being has become a key issue in perinatal mental health (NICE, 2014). In this line, the WHO (2019) has called for action to ensure a positive maternal experience that satisfies the expectations, personal beliefs, and sociocultural circumstances of women. This proposal would imply knowing and assessing not only psychological symptoms, but also well-being and life satisfaction during this stage.
Psychological Consequences of COVID-19
The global pandemic of SARS-CoV-2 (COVID-19) beginning in late 2019 has brought dramatic changes to ordinary life. Although COVID-19 is a physical illness, the mental health consequences can be very significant (Parrish, 2020) and there is no doubt the changes wrought by the pandemic caused a great deal of anxiety and insecurity among the general public (Usher et al., 2020).
In Spain, the psychological consequences of the pandemic have been evident. A study conducted during the first wave of COVID found that 22.1% of people surveyed experienced symptoms of depression and 19.6% symptoms of anxiety (Valiente et al., 2020). Within these percentages it was observed that women rather than men and the young rather than the elderly experienced greater psychological distress (Valiente et al., 2020). This study also found high levels of well-being during the pandemic. This underscores the fact that distress and well-being are relatively independent dimensions and should be evaluated separately (Keyes, 2007).
Ongoing safety measures, such as social distancing and intermittent confinement, had a negative impact on mental health in general (Chaves de Lima et al., 2020). These measures increased the likelihood of symptoms of psychological distress, such as substance abuse, depression and anxiety, intrafamily and/or domestic violence, insomnia, loneliness, and suicide (Chaves de Lima et al., 2020; Parrish, 2020). Furthermore, the absence of clear information and constant uncertainty gave rise to feelings of panic, confusion, discrimination, and anger (Usher et al., 2020).
Thus, symptomologies must be evaluated over time in order to understand the long-term impact on psychological well-being and to identify risk and protection factors among the general population. Wang et al. (2020) conducted a longitudinal study in China during the first wave (end of January 2020) and the second wave (end of February 2020) of the pandemic. The study found that rates of anxiety and depression remained stable. The results also showed that symptoms of post-traumatic stress, while slightly lower, continued to be significant.
Perinatal Mental Health during COVID-19
The experience of stress may increase certain mental health problems during the perinatal stage (WHO, 2020) and it is highly probable that the pandemic has had an impact on the perinatal mental health (Motrico et al., 2022). High rates of anxiety and depression have been found in women in the perinatal stage in various countries and cultures (e.g., United Kingdom, China, Canada, Australia, India) (Caparrós-González et al., 2020). In Spain, high levels of perinatal mental distress have also been identified. A study by Chaves et al. (2022) of 724 women in the perinatal stage found high levels of symptoms of depression and anxiety (58.7% and 51.2% respectively). Despite these high rates of psychological distress, the levels of well-being were also high. Factors such as being married, being a health worker, the perception of their own or their baby's good health, healthy eating, and sleeping habits were all associated with greater life satisfaction during the first wave of the pandemic (Chaves et al., 2022).
Psychological distress experienced during the public health emergency may be related to the various measures imposed to bring the pandemic under control. Firstly, restrictions on mobility and social relations made it difficult to establish a normal routine and social support was significantly diminished (Caparrós-González et al., 2020). Secondly, misinformation about the real risks of infection led to the imposition of procedures and protocols which were potentially harmful to women's mental health, such as restrictions on hospital visits or support during childbirth (Matvienko-Skikar et al., 2020). Recent studies have found that the risk of transmission of COVID-19 from an infected mother to their baby through breastfeeding is low and the WHO highly recommends skin-to-skin contact between mothers and newborns to establish an affective connection (Matvienko-Sikar et al., 2020). However, despite the evidence, the protocols and organisation of neonatal units have been significantly modified, possibly impacting the psychological well-being of mothers and babies.
The public health crisis caused by COVID-19 has posed a serious challenge to perinatal health. There are some Spanish studies examining the psychological impact of the pandemic during the perinatal period (e.g., Awad-Sirhan et al., 2022; Caparrós-González et al., 2020; Chaves et al., 2022; Motrico et al., 2022; Puertas-González et al., 2021), but their long-term consequences are yet unknown. Hence, it is necessary to conduct longitudinal studies which can shed light on the evolution of symptoms of depression and anxiety and perinatal well-being during the pandemic.
The aim of the present study is to evaluate the longitudinal changes experienced in perinatal mental health 6 months after the onset of the COVID-19 pandemic in Spain. The specific objectives are: 1) to analyse the changes in psychological distress (i.e., symptoms of depression and anxiety) during the perinatal stage after 6 months of pandemic; 2) to evaluate the changes in psychological well-being (life satisfaction and affective balance); 3) to identify the variables regarding the physical health of the baby and mother which may influence these changes; and 4) to explore the changes after 6 months depending on the perinatal situation (i.e., women who remained in the same perinatal stage vs. women who have passed from the pregnancy stage in the first wave to the postpartum stage in the second wave).
Method
Participants
The sample consisted of 176 women (> 18), who were pregnant or who had a baby (postnatal period up to a maximum of 6 months) at the moment of the initial evaluation at the start of the first confinement period for COVID-19 in Spain (April, 2020; for details, see Chaves et al., 2022)1. In the first wave, 59.1% of the women were pregnant (average months of pregnancy = 6.9, SD = 1.59) and the 40.9% were in the postnatal period (average months from birth = 2.2, SD = 1.55). In the second wave, 1.7% of the women were pregnant (average month of pregnancy = 7.5, SD = .9) and 98.3% were in the postnatal period (average months from birth = 6.56, SD = 3.36).
The mean age of participants was 33.80 years of age (SD = 3.89). The majority of participants were university graduates (79.4%), followed by those with vocational training (14.3%), secondary education (5.1%), and primary education (1.1%). Regarding civil status, 92.6% of participants were married or lived with their partner, 6.9% were single, and only 0.6% were separated or divorced. As for employment, 41.7% were on maternity leave, followed by 39.4% who were working, some 12% were unemployed, 6.3% were working domestically, and 0.6% were students.
Measures
Sociodemographic Information
The participants provided information on their age, civil status, education and current employment situation, and perinatal stage (i.e., prenatal/postnatal).
Information regarding their Health and the Health of the Baby
Women answered one question regarding their health (i.e., “My physical health is…/My physical health in the last 6 months has been…”) and three questions regarding the health of their baby: 1) “The health of the baby (or foetus) is/The health of the baby (or foetus) in the last 6 months has been…”; 2) “The baby's feeding is/The baby's feeding during the last 6 months has been…”; 3) “The sleep of the baby is/The sleep of the baby during the last 6 months has been…”. The last two items (i.e., feeding and sleep) were presented only to women who had given birth. These four items were answered using a Likert-type scale from 1 (poor) to 5 (excellent).
Information on the Pandemic
Two questions were included on worries associated with COVID (i.e., “Have you been worried about the possibility your baby/foetus will catch COVID-19? and “Did you worry hospitals would be overwhelmed because of COVID at the time of giving birth?”). These two questions were answered on a 6-point Likert-type scale ranging from 0 (very slightly or not at all) and 5 (extremely).
Edinburgh Postnatal Depression Scale (EPDS; García-Esteve et al., 2003).
The Edinburgh Postnatal Depression Scale (EPDS) is a self-reporting questionnaire consisting of 10 questions designed to measure the symptoms of depression during the perinatal stage. The questionnaire has a Likert-type scale with a range of 4 points, with answers from 0 (never) to 3 (very often). The reliability obtained in this study was α = .87. The optimum cut-off score on EPDS is 11 or more (Terren et al., 2003). Moreover, the cut-off score on the anxiety subscale (i.e., items 3, 4 and 5) is six or more (Matthey, 2008).
Satisfaction with Life Scale (SWLS; Vázquez et al., 2013)
This is a questionnaire consisting of 5 questions to evaluate the level of life satisfaction using a global score of the responses. The questionnaire uses a Likert-type scale with a range of 7 points, with answers from 1 (strongly disagree) to 7 (strongly agree). The reliability obtained in this study was α = .84.
Positive and Negative Affect Schedule (PANAS; López-Gómez et al., 2015)
This is a self-reporting questionnaire consisting of 20 items, 10 of which refer to the positive affect subscale and 10 to the negative affect subscale. The questionnaire uses a Likert-type scale of 5 points, from 1 (very slightly or not at all) and 5 (extremely). The reliability for this study was α = .88 and α = .89, for the positive and negative subscales respectively.
Procedure
The study was conducted using the Qualtrics platform (https://www.qualiatrics.com) and distributed through social media using snowball sampling. The initial evaluation was made during the first confinement in Spain (April, 2020) and the results have already been published (Chaves et al., 2022). The second evaluation was made in October 2020, a period when the restrictions imposed for COVID-19 were looser and more selective (i.e., according to incidence). This second wave only included participants of the first study who agreed to participate in the follow-up study. In both waves participants provided their informed consent prior to completing an online form. The same assessment protocol was completed at time 1 and time 2. Participation was voluntary and participants did not receive any reward. This study was approved by the University Ethics Committee (reference 2019/20-033) and was conducted in compliance with the Declaration of Helsinki.
Data Analysis
In order to analyse the changes to psychological well-being and distress after 6 months of pandemic, a series of Students' t tests were conducted for repeated measurements (i.e., time 1 vs. time 2). Also, differences between pregnant women and women during postpartum in both waves were also analysed using Students' t. A chi-square independence test was conducted to analyse the difference in prevalence of symptoms in both waves using the cut-offs indicated above for the EPDS.
To identify the possible variables related to the changes a series of bivariate correlations were made between the variables on the baby's and mother's health at T1 and residual scores between T1 and T2 of the variables for the symptoms and well-being. Residualised scores were obtained by removing from the T2 score the portion that can be linearly predicted by the T1 score (Castro-Schilo & Grimm, 2018).
Finally, to analyse the influence of the perinatal situation on the symptomologies and well-being, the sample was divided into two groups: 1) women who remained in the same perinatal stage (i.e., pregnant or in the postpartum stage for both waves) and 2) women who had changed their perinatal stage between the first and second wave (from pregnancy to postpartum). To analyse the main effects of time and group interaction, a series of mixed 2 x 2 ANOVA tests were conducted. All the statistical tests were parametric, since the sample size allowed assuming normality in the distribution (Pardo et al., 2009).
The data obtained in the study was analysed using the Statistical Package for the Social Sciences 25.0 (SPSS) for Windows.
Results
Analysis of Changes in Psychological Distress and Well-being
Table 1 provides the descriptive statistics for waves 1 and 2. Regarding psychological distress, a statistically significant decrease in the prevalence of symptoms of depression, t(174) = 2.58, p = .01, d = 0.02, was found over the 6-month period. Differences were also found in the proportion of women who reported symptoms of perinatal depression (EPDS ≥ 11) in October compared to April, χ2(1)= 16.21, p < .001, phi = .30. The prevalence of depression in the second wave (October) was 54.3%, compared to 60% in the first wave (April). Of this percentage, 14.3% were new cases (n = 25). Some 20% of participants (n = 35) stopped experiencing symptoms of depression in the second wave while 40% (n = 70) continued to experience depressive symptoms from the first wave and 25.7% (n = 44) remained without any symptoms.
Table 1. Descriptive Statistics and analysis of the Differences between Waves 1 and 2.
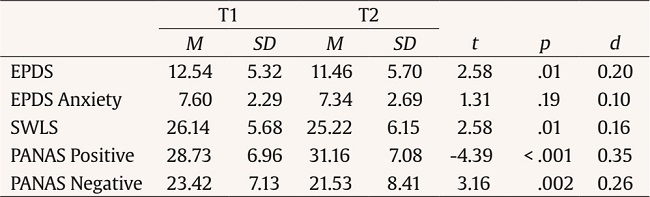
Note.EPDS = Edinburgh Postnatal Depression Scale; SWLS = Satisfaction With Life Scale; PANAS = Positive and Negative Affect Schedule.
Symptoms of anxiety remained stable over the 6 month period without any statistically significant differences, t(174) = 1.31, p = .19. The prevalence of anxiety in the second wave (October) was 53.4%, similar to the 54,6% in the first wave (April). Of this percentage, 17.7% were new cases (n = 31). Some 18.9% of participants (n = 33) stopped experiencing anxiety in the second wave while 35.4% (n = 62) continued to experience symptoms of anxiety since the first wave and 28% (n = 49) had no symptoms.
In relation to symptoms of anxiety, it should be noted that 47.5% of participants reported being worried about the possibility of their baby/foetus becoming infected with COVID-19. Furthermore, 61% reported being worried about hospitals being overwhelmed at the time of giving birth.
Regarding psychological well-being, statistically significant differences were found in life satisfaction, t(175) = 2.58, p = .011, d = 0.16, with lower levels after 6 months. Statistically significant differences were also observed in the two subscales of affective balance, with an increase in positive affect, t(175) = -4.45, p < .001, d = 0.35, and a decrease in negative affect, t(175) = 3.15, p = .002, d = 0.26, after 6 months.
Differences between the pregnant women and women during postpartum in both waves were also tested. No significant differences were found in any of the variables included, except for SWLS were women in postpartum phase showed higher levels of satisfaction with life in the first wave (Table 2).

Effect of the Physical Health of Mother and Baby on Changes in Symptoms and Psychological Well-being
A series of bivariate correlations were performed to explore the effect of the physical health of the mother and baby at time 1 on changes in symptomology and psychological well-being (Table 3). The results show that the quality of the baby's sleep is associated with lower levels of depression (r = -16, p =.03) and negative emotions (r = -20, p = .01), and an increase in positive emotions (r = 15, p = .04). The baby's health is also associated with an increase in positive emotions of the mother (r = .17, p =.02). Finally, the mother's health is associated with a reduction in depression levels (r = -.22, p = .003) and negative emotions (r = -.25, p =.001), and increased positive emotions (r = .20, p =.007).

Effect of the Change in Perinatal Stage on Psychological Well-being and Distress
To analyse the influence of the perinatal stage on symptomologies and well-being, the sample was divided into two groups: 1) women who remained in the same perinatal stage (i.e., pregnant or in the postpartum stage for both waves) and 2) women who changed perinatal stage between the first and second wave (from pregnancy to postpartum). First, the differences between the two groups in the first evaluation (April) were analysed. No significant initial differences were found between the groups for any of the analysed variables: depression (t = -4.53, p = .651), anxiety (t = .087, p = .931), positive emotions (t = 1.353, p = .178), negative emotions (t =1.842, p = .067), and life satisfaction (t = .371, p = .711).
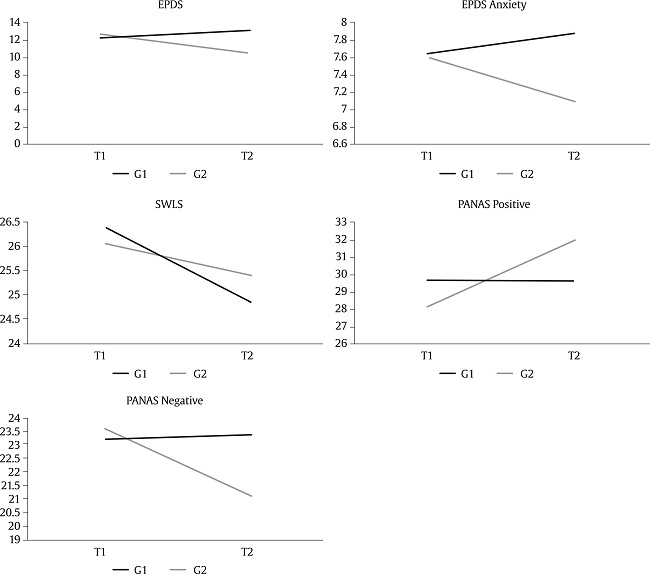
Table 4 shows descriptive statistics and the results of the ANOVA test of the repeated measures for psychological well-being and distress variables according to the perinatal stage. The results show significant interactions between group and time for depression, anxiety, and positive and negative emotions. The interaction effects can be observed in Figure 1. The group experiencing a change in perinatal stage (from pregnancy to postpartum) showed lower levels of depression, anxiety, and negative emotions and higher levels of positive emotions in the second wave (October). This interaction was not observed in life satisfaction, that showed a significant decline for both groups from the first wave (April).
Table 4. Descriptive Statistics and ANOVA of the Repeated Measures for Variables in Psychological Well-being and Distress in Both Groups.

Note.Group 1 = remaining in the same perinatal stage (n = 59); group 2 = change in perinatal stage (n = 117); T1 = first wave; T2 = second wave.
Discussion
The aim of this study was to evaluate the changes in perinatal mental health over the course of 6 months from the onset of the COVID-19 pandemic in Spain. Regarding the first specific objective (to analyse the changes in psychological distress), it was found that symptoms of depression decreased 6 months from the start of the pandemic, where some 20% of participants stopped experiencing perinatal depression. The results show that the high rates of symptoms of depression at the onset of the pandemic may have been a normal reaction to the stress generated by a public health crisis which was unprecedented for most of the population (Fernández-Theoduloz et al., 2022). Furthermore, the end of the strict confinement in Spain and the lifting of many restrictions may explain the decrease in depressive symptoms (Ramírez-Ortiz et al., 2020). A study on the types of psychological responses to situations of pandemic found that 55.3% of people showed resilience in the face of traumatic events, a more common response than any other (Valiente et al., 2020). This may explain the high percentage of mothers who stopped experiencing perinatal depression six months after the first wave. It is important to note that 54.3% of participants showed symptoms of perinatal depression in October, of whom 40% were women whose symptoms of depression persisted until April. These high rates of perinatal depression coincide with the findings of a study conducted in Poland, which showed an increase in rates of perinatal depression compared to before the pandemic (Chrzan-Dętkoś et al., 2020). These results underscore the importance of conducting psychological evaluation of women during the perinatal stage.
Also of note is that 14% of women without symptoms of depression in the initial evaluation reported these symptoms six months later. These results show the existence of different patterns of response to the pandemic, with some women responding with a delayed depression. It would be interesting to further study the factors associated with these different patterns of response.
With regard to symptoms of anxiety, it was found that rates remained stable over the six month period. The findings on levels of psychological distress are in line with the results of a longitudinal study on the psychological impact of COVID-19 among the general population in Spain which showed a slight decrease in symptoms of depression and stable levels of anxiety 4 months from the start of the pandemic (González-Sanguino et al., 2021). The authors indicated that, although the symptoms of depression began to decrease when the confinement was lifted, concerns about contagion and health persisted over time. Additionally, it was also found that a higher percentage of women were worried about the possibility of their baby catching COVID-19 (47.5%) or that hospitals would be overwhelmed at the time of giving birth (61%). These figures reveal the high degree of uncertainty among women due to the pandemic. The SARS-CoV-2 pandemic also caused changes in the protocols and organisation of neonatal units, such as the reduction of hospital stays and restrictions on accompaniment during childbirth (Arnáez et al., 2020). These changes can accentuate the uncertainty and anxiety of mothers, as was found in research into previous public health crises. Research on the SARS outbreak of 2003 shows that pregnant women were very worried about the risk of infection, transmitting the virus to the foetus or catching SARS during childbirth or when at the hospital. Two thirds of women were afraid to go to the hospital and one third adopted strategies to reduce their risk of infection (for example, self-confinement) (Lee et al., 2007). It would be interesting to further research the psychological consequences of circumstances such as self-confinement, living with an infected person, limited access to healthcare during pregnancy, and/or worry about overwhelmed hospital services.
Regarding the second specific objective of the study (i.e., to evaluate the changes in psychological well-being of women in the perinatal stage), it was found that life satisfaction decreased significantly over the 6-month period. These findings are in line with those of the previous study (Contra el Estigma, 2020), which observed a decrease in psychological well-being 4 months from the onset of the pandemic. Life satisfaction is a global self-evaluation of a person's life and reflects, in part, their perception of their quality of life (Veenhoven, 2009). Given the changes to normal life which took place during these six months (i.e., numerous restrictions on mobility, interpersonal distancing, uncertainty, changes in work, etc.), a decrease in life satisfaction could be expected, as seen during previous times of social or economic crisis in Spain (Bartoll et al., 2014).
It was found, however, that levels of positive affect increased and negative affect decreased in comparison to the first wave. Note that PANAS is a measurement which is highly sensitive to changes in hedonic tone (Watson et al., 1988). These results may confirm the concept of hedonic adaptation (Lyubomirsky, 2011), defined as the capacity for people to adapt to positive or negative circumstances in life. Thus, after a brief period of adaptation, people return to their baseline state of well-being even after suffering severely negative events (Godoy-Izquierdo et al., 2008).
The drop in life satisfaction and the improvement of affective balance after six months of pandemic shows that well-being is a complex and multidimensional construct (Ryan & Deci, 2001). Life satisfaction is often considered the cognitive component of well-being while affect is the emotional aspect (Vázquez et al., 2009). The emotional component refers to pleasant or unpleasant experiences, moods or states measured in a specific time. However, life satisfaction refers to the degree to which an individual subjectively perceives that his/her aspirations are attained or satisfied (Diener et al., 2003), considering quality of life, environment, and real living conditions. This study shows that the different components of mental health evolved differently during the pandemic and thus it is important to evaluate them independently.
With regards to the third specific objective (i.e., to identify the variables which may influence these changes), it was found that the quality of sleep and physical health of the baby and mother are important factors in the improvement of symptoms and the well-being of mothers during the pandemic. The decrease in symptoms of depression and negative emotions was associated with the baby's better quality of sleep and better physical health of the mother while the increase in positive emotions was associated with the baby's better sleep and better perceived health of the baby and mother. These proved to be important factors in explaining symptoms of depression in the first wave (Chaves et al, 2022). Sleep disturbances and perceived physical health are variables traditionally associated with depression during the perinatal stage (Ross et al., 2005).
As for the fourth specific objective (i.e., to explore the changes after 6 months depending on the perinatal situation), it was found that women who changed their perinatal stage (from pregnancy to postpartum) had lower levels of depression, anxiety, and negative emotions and higher levels of positive emotions six months after the start of the pandemic as compared to women who remained in the same perinatal stage. This may indicate that symptoms of depression tend to decrease after childbirth with a simultaneous increase in positive emotions. Despite the fact the pandemic and the new situation of being a mother are potentially stressful (Geller, 2004), the birth of the baby may result in a relief of symptoms and the general improvement of well-being among the participants. Additionally, no significant differences were found in terms of life satisfaction according to the perinatal situation – both groups showed a significant decrease compared to the first wave (April). These results reaffirm that the different components that make up well-being can function relatively independently from each other (Veenhoven, 2009).
In conclusion, this study represents an advance in the understanding of perinatal mental health both in general and in situations of crisis such as that caused by COVID-19. A better understanding of psychological distress and well-being can help prevent the appearance of mental health problems in the event of subsequent waves of the pandemic (Thombs et al, 2020).
This study presents certain limitations. Firstly, due to the characteristics of the research (i.e., online survey, probabilistic snowball sampling), it is possible that the most vulnerable families did not participate in the study and the results only reflect the view of those families in better circumstances. Thus, it is necessary to carry out further studies which include all socioeconomic levels of the population. Secondly, there are some factors that were not examined in the current study but may have also contributed to the decrease in symptoms over time, such as the recovery of social support or the economic activity after the lifting of lock-down, or the change in perinatal status (from pregnant to postpartum). In the future, it is important to consider this last factor since previous research has shown that there are variations during the perinatal period in terms of symptoms of depression and anxiety (Teixeira et al., 2009). Furthermore, a longer time frame is necessary to follow-up the changes of this pandemic. Thirdly, using a more robust measure of anxiety would help draw stronger conclusions regarding this dimension.
Despite these limitations, this work contributes to a better understanding of perinatal mental health during the COVID-19 pandemic and may serve as the basis for future research. Some contributions can be highlighted. First, this is the first longitudinal study on the consequences of COVID-19 on perinatal mental health in Spain. It provides information on the mental health of a relatively large sample of pregnant and postpartum women at different times of the COVID-19 pandemic. Second, this is also the first study on COVID-19 on perinatal mental health in Spain that incorporates measures of both symptoms and well-being. Research on the architecture of mental health has consistently found that well-being and symptoms can be considered as two dimensions that are relatively independent of each other (Watson, 2016). Although most of the extant research on perinatal mental health has focused on the study of negative symptoms, the results of this study support the need to evaluate these dimensions separately. A model of human functioning which considers both positive and negative aspects offers a more complex perspective on human nature (Keyes, 2007). It is expected that this study may lay the foundations for the design of interventions aimed at preventing psychological distress, especially anxiety, and the promotion of life satisfaction, in the perinatal stage when facing stressful circumstances. In the future, it would be helpful to identify those variables which facilitate the remission of symptoms and to study the factors which promote psychological well-being in the long term. It would also be interesting to continue delving into the psychological consequences of specific aspects of the public health crisis. The COVID-19 pandemic is an evolving situation, bringing new uncertainties, fears, and consequences both globally and on an individual level, particularly changes in economic circumstances, healthcare, interpersonal relationships, etc. which may have an impact on multiple psychological dimensions. It is therefore essential to take a broader view of the psychological aspects of the perinatal stage, considering the causes of both clinical disorders and psychological well-being.

