










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Acute pancreatitis is a reversible inflammation of the pancreas. It is histologically characterized by the presence of pancreatic edema, acute inflammatory infiltration, and pancreatic necrosis or hemorrhage in the acinar cells of the pancreas. The diagnosis of childhood acute pancreatitis is made according to the INSPPIRE criteria. According to these criteria, acute pancreatitis is diagnosed by abdominal pain consistent with acute pancreatitis and suggesting pancreatitis, serum amylase or lipase levels 3 times the upper limit of normal, and the presence of two of the characteristic imaging findings consistent with acute pancreatitis (1-3).
Childhood acute pancreatitis has been increasing over the last 20 years. Its incidence is known to be 3-13/100,000. Although risk factors vary depending on age group in childhood pancreatitis, the factors of biliary disease, drug use, abdominal trauma, and metabolic diseases come to the fore. In recent years, genetic risk factors have also been identified in acute recurrent pancreatitis with an increasing frequency (4,5).
The Mediterranean diet is a diet type typically including high consumption of fruits and vegetables, dried legumes, dried fruits and nuts, cereals, olive oil, and fish; moderate consumption of dairy products; and low consumption of red and processed meat. The beneficial effect of this diet, which is followed in communities close to the Mediterranean region, against cardiovascular, metabolic, and mental diseases has been reported in many studies. In a study investigating the adherence to the Mediterranean diet of children and young people living in the Mediterranean region, the prevalence of adherence to the Mediterranean diet was 4.2 % in Spain, 14.9 % in children and 27 % in adolescents in Greece, and 23 % in children and 33 % in adolescents in Italy (6-9).
It has been reported that the prevalence of high adherence to the Mediterranean diet is 13 %, and the prevalence of moderate adherence is 48 % in European countries without a Mediterranean coast. In a study evaluating Mediterranean diet adherence of adolescents in the USA, 81.4 % of adolescents had poor adherence, 17.8 % had moderate adherence, and 0.75 % had good adherence (10,11).
In the literature, there is limited information on how diet affects the pathogenesis of pancreatitis. In the comprehensive multi-ethnic cohort study by Setiawan et al., dietary factors were shown to be effective especially in patients with pancreatitis associated with the gallbladder. In the same study, the consumption of red meat and eggs, rich in saturated fat and cholesterol, was associated positively with biliary pancreatitis, while the use of vitamin D and dietary fiber decreased the formation of biliary pancreatitis. Also the consumption of coffee decreased non-biliary acute and recurrent pancreatitis. In addition, dietary fiber was reported to be protective against pancreatitis. However, Yadav et al. could not show any relationship of diet with the etiology of pancreatitis other than high alcohol consumption (12,13).
There are a limited number of studies showing the relationship between childhood acute pancreatitis and diet. The aim of this study was to investigate compliance with the Mediterranean diet in children with acute pancreatitis.
MATERIALS AND METHODS
This study was conducted with children between the ages of 2 and 18 years, who were diagnosed with pancreatitis and followed up in the Afyonkarahisar Health Sciences University, Faculty of Medicine, Child Health and Diseases Outpatient Clinic between January 2014 and January 2019, as well as with healthy volunteers. The study included a total of 100 children, 50 of whom were diagnosed with pancreatitis whereas the remaining 50 were healthy controls. The diagnosis of pancreatitis was made according to the INSPIREE criteria (14). Those under the age of two, those with chronic diseases, and those who did not agree to fill in the questionnaire were excluded from the study. The control group included volunteers who were healthy, did not have any chronic disease, and agreed to fill in the questionnaire. The control group was randomly selected from among healthy children who came to follow-up outpatient clinic The control group was not matched by age or gender.
The anthropometric measurements of all children were performed by the same person, and their body mass indexes were adjusted according to the World Health Organization criteria. Body mass index was calculated by dividing the weight in kilograms by the height in meters squared (body weight (kg) / height2 (m)). In determining nutritional status, Z-scores were used for "height for age", "body weight for age" and "body mass index for age."
In order to determine the dietary habits and diet qualities of children, a KIDMED evaluation, which is an easy and valid method, was performed as an indicator of healthy nutrition. The KIDMED, developed by Serra-Majem et al., is an index consisting of a total of 16 questions including the characteristics of the Mediterranean diet (15). A score of 12 denotes a positive connotation for a healthy diet (questions 1, 2, 3, 4, 5, 7, 8, 9, 10, 11, 13, and 15), while a score of 4 denotes a negative one (questions 6, 12, 14, and 16). A "Yes" answer to positive questions was evaluated as +1 point, and a "No" answer was evaluated as 0 points, whereas a "Yes" answer to a negative question was evaluated as -1 point and a "No" answer was evaluated as 0 points. The highest score that can be obtained is 12.
The ethics committee approval for the study was obtained from the Clinical Research Ethics Committee at Afyonkarahisar Health Sciences University, Faculty of Medicine, with code number 19/09/2018-E.40551. A written consent was obtained from the families of the children participating in the study.
STATISTICAL ANALYSIS
The data obtained were evaluated with descriptive statistics (arithmetic mean, median, standard deviation, percentage distributions). When comparing the intergroup mean, the normality of the data was first evaluated using the Shapiro-Wilk test. When comparing the means of two independent groups, the Mann Whitney U-test was used, since parametric conditions were not met. When comparing the percentage distributions of categorical data between groups, the Chi-squared test was used. Factors affecting the risk of pancreatitis were evaluated using a binary logistic regression analysis. The SPSS, version 20 (IBM, New York, United States of America), software was used to analyze the data, and a p-value of < 0.05 was considered significant.
RESULTS
Table I shows the values for age, gender, and the Z-scores for weight, height, and BMI. There was no significant difference in terms of sociodemographic characteristics between the parents of children diagnosed with pancreatitis (p = 0.45). When parental educational status was compared, of the parents of the children diagnosed with pancreatitis, 8 % were illiterate, 40 % were literate and primary school graduates, 46 % were secondary school or high school graduates, and 6 % were higher school graduates and above; of the parents of the control group, not one was illiterate, 32 % were literate and primary school graduates, 56 % were secondary school and high school graduates, and 12 % were higher higher school graduates and above; there was no statistically significant difference between groups in terms of parental educational status (p = 0.603).
Table I. Comparison of Z scores (weight, height, body mass index [BMI]) between children diagnosed with pancreatitis and children in the control group
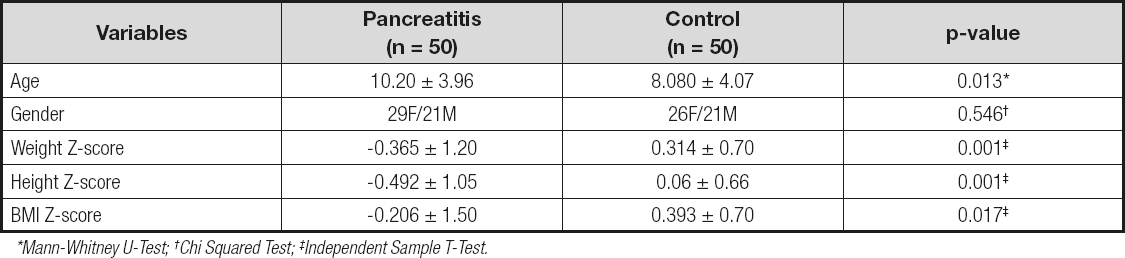
*Mann-Whitney U-Test; †Chi Squared Test; ‡Independent Sample T-Test.
Considering the KIDMED index score of the children diagnosed with pancreatitis, 8 % of the children had high adherence with 8 points, 56 % had moderate adherence with 4-7 points, and 36 % had low adherence with 3 points. In the control group, 28 % of the children had high adherence with 8 points, 54 % had moderate adherence with 4-7 points, and 18 % had low adherence with ≤ 3 points. There was a statistically significant difference between groups in terms of KIDMED index diet quality (χ2 = 8.574, p = 0.014) (Fig. 1).

Figure 1. Distribution of KIDMED Index scores for patients diagnosed with pancreatitis and the control group.
The KIDMED scores (4.48 ± 2.45) of the children diagnosed with pancreatitis were found to be significantly lower than the scores (6.62 ± 2.18) of the control group (u = 638.5; p < 0.001).
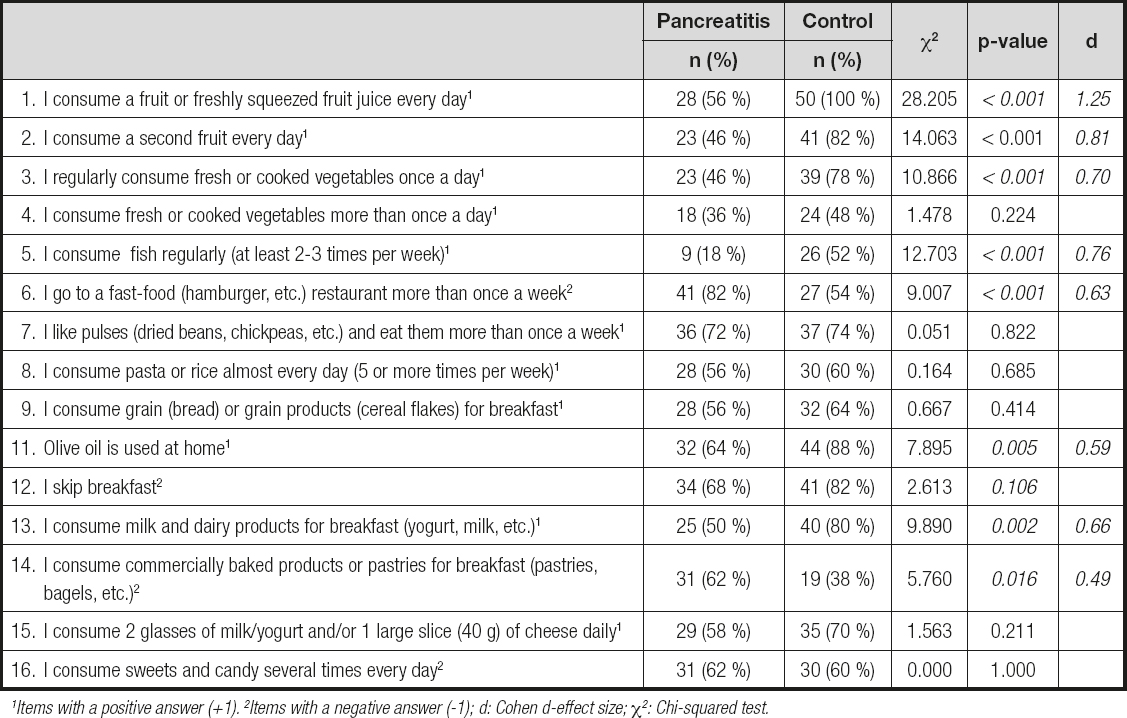
The children with a moderate KIDMED index score (4-7) (OR: 3.734; 95 % CI: 1.068-13.058; p = 0.039) and the children with a poor KIDMED index score (≤ 3) (OR: 6.449; 95 % CI: 1.595-26.075; p = 0.009) were found to have an increased risk of developing pancreatitis. It was found that the risk of pancreatitis increased with age (OR: 1.136; 95 % CI: 1.020-1.266; p = 0.021). Table II shows the rate distribution of the "Yes" answer to the questions in the KIDMED questionnaire.
DISCUSSION
This study is one of the first studies evaluating adherence to the Mediterranean diet in children diagnosed with pancreatitis, and demonstrates that children diagnosed with pancreatitis have a lower adherence to the Mediterranean diet than the control group. In addition, it was found that the risk of developing pancreatitis was increased in patients with a low KIDMED index score.
The relationship of dietary patterns and diet types with pancreatitis is not fully understood. However, it has been demonstrated that there is a relationship between the low-quality Western-style diet and pancreatic cancer (16,17). In a study by Setiawan et al., it was reported that s saturated fat and cholesterol-rich diet was effective in the formation of gallstone pancreatitis, while vitamin D, milk, and fruit consumption reduced this risk. The same study reported a relationship between vitamin D deficiency and chronic pancreatitis (12).
It has been supported by other studies that the Mediterranean diet is of great importance for the prevention of chronic diseases and reduces the risk of cardiovascular disease and cancer (18,19). It has been proven by studies that the high fiber content, low glycemic index and glycemic loads, and both anti-inflammatory and antioxidant effects of foods in the Mediterranean diet have positive effects on health (20-24).
In this study, it was found that the children diagnosed with pancreatitis had a lower daily consumption of vegetables and fruits, milk and dairy products, fish, and olive oil than the control group, while they had a higher consumption of fast food, and commercially baked products or pastries. Aboul-Mahasen et al. reported that the use of olive oil and Nigella sativa seed oil in hyperlipidemic mice had antihyperlipidemic and hypoglycemic properties, and a protective effect on the pancreas (25). Díaz et al. reported that pancreatic secretion flow rate, protein content, and amylase amount were positively affected in mice given olive oil when compared to those using sunflower oil (26).
In a study by Archero et al., investigating adherence to the Mediterranean diet among school children, the adherence found was low in 16.7 % (score ≤ 3), moderate in 63.7 % (score 4-7), and high in 19.6 % of children (score ≥ 8). In our study, it was found that adherence was low in 18 %, moderate in 54 %, and high in 28 % of the healthy children constituting the control group, which was similar to the findings of the study by Archero et al. In the pancreatitis group, adherence was low in 36 %, moderate in 56 %, and high in 8 % of the children, and there was a significant difference when compared to the healthy control group (χ2 = 8.574, p = 0.014) (27).
Dietary factors in the etiology of pancreatitis are not clearly understood. However, there are many studies in the literature that reveal a relationship between pancreatic cancer and diet. These studies have shown that, especially, excessive consumption of meats cooked at high temperatures and processed meats increases the risk of pancreatic cancer, while the Mediterranean diet, along with other factors indicative of a healthy lifestyle, are protective against pancreatic cancer (28-30).
In the meta-analysis by Zhao et al., red and processed meat consumption was shown to be associated with pancreatic cancer. In cohort studies, it has been reported that consumption of red and processed meat causes cancer more commonly in men than in women (31). In our study, children with acute pancreatitis more frequently ate at fast-food restaurants, and/or consumed commercial baked goods or pastries for breakfast than those in the control group. In the meta-analysis by Alsmarra et al., consumption of vegetables and fruits reduced the risk of developing pancreatitis and pancreas cancer (32). In our study, children with pancreatitis consumed fewer vegetables and fruits once a day when compared to healthy children.
Temporary or long-term pancreatic enzyme deficiency is a common complication in pancreatic diseases. Acute pancreatitis is an inflammatory process that affects the peripancreatic tissues and some organs. In a metanalysis, it was reported that the incidence of exocrine pancreatic insufficiency was 25 % after an episode of acute pancreatitis. While abdominal pain occurs in the early phase of pancreatitis, exocrine and endocrine insufficiency occurs as the disease progresses. It has been reported that a fiber-rich diet positively affects the course of pancreatitis by improving gastrointestinal function and affecting pancreatic enzyme activities (33-36). In a study by Setiawan et al., it was reported that dietary fiber had preventive effects on the formation of pancreatitis (12). Olah et al. also showed that the use of fiber-containing food in patients with acute pancreatitis was significantly effective in reducing the length of hospital stay and complications (37). In the treatment of acute pancreatitis, it was recommended to discontinue oral feeding to reduce pancreatic exocrine secretions. However, in the absence of ileus or vomiting, it is more recently recommended to start feeding early, within the first 24 hours in cases where pain and inflammatory markers decrease. Early feeding in pancreatitis not only restores energy balance but also maintains the intestinal barrier function, preventing bacterial translocation and providing immunomodulatory and antioxidant effects (38).
Prizmant et al. reported that the use of total and saturated fat increased the risk of acute pancreatitis (39). Thomas et al. reported that long-term high-fat dietary intake played a trigger role in gallstone formation and acute pancreatitis (40). Dietary fiber has been reported to play a role in the gut microbiota, in improving the frequency of intestinal epithelial junctions, and in the prevention of endotoxin passage into the circulation (41,42). In the studies with experimental animal models of acute pancreatitis, endotoxins support the development and severity of pancreatitis. Tsai et al. reported that a diet containing water-insoluble fiber prevented the development of acute pancreatitis by reducing the formation of gallstones (43). They also reported that high amounts of vegetables and fruits in the diet reduced the formation of gallstones and the risk of cholecystectomy (44).
Oskarson et al. reported that fish consumption provided a reduction in the risk of acute pancreatitis not associated with gallbladder issues through the antiinflammatory and antioxidative properties of long-chain n-3 polyansature fatty acids in fish (45). In experimental pancreatitis models, caffeine has been shown to produce a protective effect by inhibiting the pathological calcium signal in pancreatic acinar cells (46). There are contradictory results regarding the association between coffee consumption and pancreatitis in two separate studies by Morton and Oskarsson (47,48). Alvarino et al. reported that individuals following a high-fat diet were diagnosed with chronic pancreatitis at an earlier age (49). Salem et al. reported that diet and lifestyle were important for pancreatic cancer development; however, extensive studies are needed to confirm this (17). While the Western pattern diet induces pancreatic cancer formation, a healthy diet has been reported to reduce the risk of pancreatic cancer (50).
In our study, we found that children with acute pancreatitis did not have a healthy diet as compared to the control group. Włochal et al. reported that 36 adult patients with pancreatitis (24 with chronic pancretitis, 12 with acute pancreatitis) had insufficient nutritional knowledge (51). Kolonel et al. conducted a multiethnic cohort study by examining the frequency of use of pancreatitis products, to which end they analyzed the hospital records between 1993 and 1996 in Hawaii and Los Angeles. In this study, it was reported that the frequent consumption of red meat and eggs, a diet rich in saturated fat and cholesterol, was positively associated with gallbladder disorders in patients with acute pancreatitis, whereas the consumption of milk and foods rich in fiber and vitamin D was the opposite (52). In our study, the low compliance score with the Mediterranean diet, consisting of olive oil and rich in vegetables and fruits, in fiber and non-saturated fat, seen in children with pancreatitis suggests that diet may have an effect on the development of pancreatitis. In addition, the fact that the weight and height Z-scores of the children with pancreatitis were lower than those of the control group, regardless of age, suggests a deficiency related to an unhealthy diet. However, the findings of our study cannot fully prove a causal relationship between eating habits and the development of pancreatitis. Multicenter, randomized, controlled studies are needed for this.
In addition to being among the pioneering studies in the field, the present research has various limitations. First of all, the fact that the measurements were based on the individuals' own statements, and the results were based on the memory factor, which undermines the reliability of the data. The small sample size of the study group and the data obtained from a single center are additional limitations of our study. However, the fact that the children diagnosed with pancreatitis and control group were similar in terms of age and gender, and the exclusion of individuals with comorbid diseases rendered the inferences about dietary factors more accurate. It is understood that the education of children and their families on healthy nutrition that health professionals may impart is important.
In this study, the pancreatitis and control groups were similar in gender, but there was a difference in age. There was also a difference in terms of KIDMED index scoring. According to the scores obtained from the KIDMED index, the dietary habits of the pancreatitis group were poorer than those of the control group.
Due to the potential protective effects of the Mediterranean diet, it can be considered a possible adjunctive treatment in the future for patients with pancreatitis. Therefore, a healthy lifestyle and nutrition should be encouraged in patients with pancreatitis. However, randomized controlled studies are not yet sufficient to show that the Mediterranean diet, which is a healthy diet, can prevent pancreatitis. There is a need for detailed studies on this subject in the future. Although the relationship between dietary habits and many diseases has been studied in the literature, the relationship between pancreatitis and dietary habits has not been studied sufficiently. Larger, multicenter studies are needed to confirm the relationships we have demonstrated in our study, and to reveal the causal relationships involved.

