










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Vitamin D status has been studied in all continents and most countries over the world, and there is a global high prevalence of deficiency (1), ranging from 30 to 70 %, constituting a public health problem (2). The aging population in Latin America is characterized by an elevated poverty rate, a high burden of comorbidity, and sub-optimal social conditions contributing to a poor health status, where social and health services are limited (3), which may also contribute to increase the prevalence of vitamin D deficiency (4). Mexico is living the demographic and epidemiological transitions associated with the increase in life expectancy, and a growing number of elders (5), and a high prevalence of vitamin D deficiency (6,7), despite being a country with adequate exposure to sun and ultraviolet B rays (UVB) during the year (8).
Low levels of vitamin D are frequently found in the elderly as a result of changes associated with aging on vitamin D and calcium and metabolism such as decreased calcium absorption, intestinal resistance of calcium absorption to circulating 1,25(OH)2D, decreased vitamin D receptor, decreased renal production of 1,25(OH)2D by the aging kidney, decreased skin production of vitamin D, and substrate deficiency of vitamin D (9).
Low vitamin D levels are associated with several geriatric syndromes, including frailty (10-12), sarcopenia (13), falls, fractures, cognitive impairment, depression, cardiovascular disease, colorectal cancer, diabetes (14), and mortality in general (15-20), and in distinct clinical scenarios, such as institutionalized elderly people (21). Although, the evidence shows that low serum levels of vitamin D are associated with mortality, currently there is no consensus on optimal 25(OH)D concentrations (14,22,23). While there are many recommendations regarding optimal levels of vitamin D (24), a putative threshold in which of vitamin D is associated with higher mortality in Mexican population has not been defined. Our hypothesis is that vitamin D levels below 15 are associated with a higher mortality in Mexican population. Therefore, the objective of this analysis was to determine the association between low levels of vitamin D and mortality in Mexican population, from the database of the Mexican Health and Aging Study (MHAS) (25), a prospective study in Mexicans, as well as their couples, who through a survey on the processes of aging and the burden of disease that occur in this group and recording data in 2001, 2003, 2012, and 2015 (with measurement of mortality).
MATERIAL AND METHODS
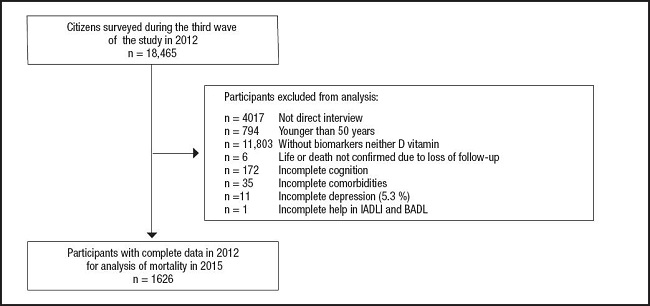
To carry out the present work we used the MHAS database (25). The methodology was conducted by the Center for Population Studies at the University of Pennsylvania, Center for Research on Population at the University of Maryland and the Center for Demography and Ecology, University of Wisconsin, while the National Institute of Statistics, Geography and Informatics (INEGI) of Mexico performed fieldwork. Information related to various aspects, such as dynamics of health, family structure and intergenerational transfers, migratory behaviors and socioeconomic differences by income and property ownership was collected. The sample is representative of the non-institutionalized population component aged 50 years in 2000. Collecting data from the first round was conducted from May to October 2001 and a second round took place from June to September 2003 in which participants were re-interviewed in 2001, and a third and fourth round in the years 2012 and 2015 respectively. For the present analysis all subjects 50 years or older evaluated during the 2012 wave, with serum levels of vitamin D, who underwent a follow-up in 2015 and determined whether they were still living or not were selected. We excluded participants in who we could not determine the status of the studied variables (missing values). The MHAS is partly sponsored by the National Institutes of Health/National Institute on Aging (grant number NIH R01AG018016) and the INEGI in Mexico. Data files and documentation are public use and available at www.MHASweb.org (25).
CATEGORIZATION OF VITAMIN D
Methodological parameters for determining levels of vitamin D can be found in the web page of the MHAS (25) and were described previously by Carrillo Vega et al. (6). Briefly, Biomarkers and vitamin D were obtained between October and November 2012, with trained personnel, who performed the peripheral venipuncture. After the venipuncture, the sample was centrifuged during 15 minutes to separate the serum, and stored in two 2-mL tubes. Serum vitamin D levels was measured with a chemiluminescent microparticle immunoassay (CMIA-Architect Abbott Laboratories. Abbott Park, IL, USA). The measurement interval of this CMIA ranged from 8 to 160 ng/mL, and the intra- and inter-assay coefficients of variation were < 10 %. Serum 25(OH)D levels were categorized into four groups, based on cut-points used in previous studies on vitamin D and frailty: < 15, 15-< 20, 20-< 30 and ≥ 30 ng/ml (10,11).
ANALYZED COVARIATES
We analyzed the following variables: gender, age, self-reported comorbidities such as hypertension or high blood pressure, diabetes or high sugar level in blood, cancer, lung disease, heart disease (heart attack), brain disease (stroke, stroke or transient ischemic attack), arthritis or rheumatism, kidney and/or liver infection, Pneumonia, Herpes Zoster, and Tuberculosis. For these comorbidities, we created the variable number of comorbidities, representing the sum of the latter, and have values ranging from 0 to 12. We also included: quality of vision, and hearing, frequency of smoking, and drinking. Cognitive status was evaluated through the cross-cultural cognitive examination, which has a sensitivity of 100 % and a specificity of 83 % for patients with dementia (26). Depressive symptoms were measured with a validated nine-item questionnaire (27). Functional assessment was obtained by the number of basic or BADL (bathing, dressing, toileting, moving, eating and being continent, score 0-6) and instrumental activities of daily living or IADL (preparing hot food, buy food, taking medications and managing their money, score 0-4) for which require assistance. Mortality was reported in the fourth round of the survey in 2015. Missing values were considered in the case of respondents did not answer or replied, “do not know” on each of the variables analyzed. All subjects who participated in the study gave their informed consent at the time of interview.
STATISTICAL ANALYSIS
The analysis was performed by the method of complete cases (only those subjects without missing values in the variables analyzed) (28). Participants were characterized by using descriptive statistics, and included median, and interquartile range for quantitative variables, and absolute frequencies, and percentages in the case of qualitative variables. Chi square tests were used to determine differences between qualitative variables, and Kruskal Wallis test to demonstrate the difference between quantitative variables. p values lower than 0.05 were considered statistically significant. The variable survival time was calculated from the time in weeks between the date of the clinical evaluation of the third (2012) and the fourth wave (2015) evaluation or by the date of death. The degree of association of variables was measured with hazard ratio through Cox regression model. A minimum of 121 participants in each group was estimated to identify statistically significant difference in proportions between 0.15 and 0.025 through Chi square two-tailed test, power of 0.9 and alpha of 0.05 for mortality variable. All statistical analyses were performed using Stata/SE, version 12 (Stata Corporation, College Station, TX, USA).
RESULTS
GENERAL CHARACTERISTICS OF THE PARTICIPANTS IN THE YEAR 2012
Baseline clinical and demographic characteristics of 1626 selected participants were grouped and analyzed according to vitamin D levels (Table I and Fig. 1). The groups of vitamin D levels < 15, 15-< 20, 20-29, and 30 or more, included 174 (9.3 %), 339 (20.8 %), 772 (47.4 %), and 341 (20.9 %) respectively. With regard to their general characteristics, those with lower levels of vitamin D were older, more often women, required more aid for activities of daily living, reported higher number of chronic diseases, and lower scores on cognition.
Table I. Demographic and health variables of respondents in the Mexican Health and Aging Study, according to serum vitamin D levels in ng/mL.
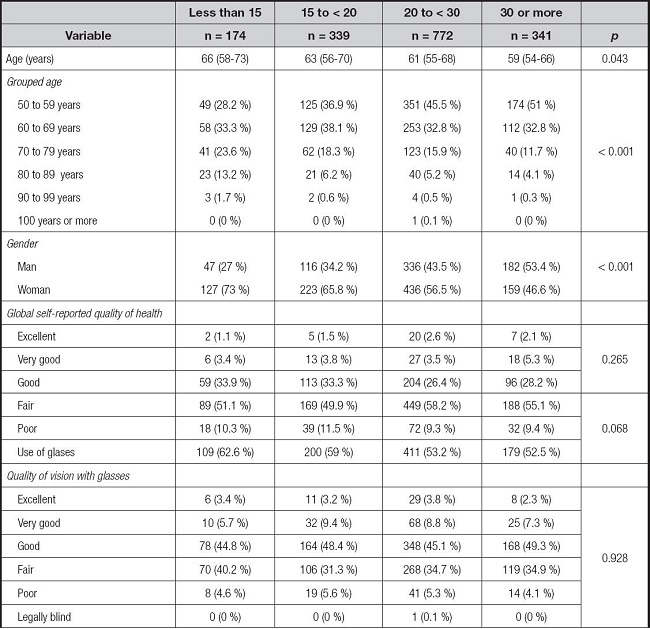
The data represent absolute frequencies and percentages or medians (interquartile range). Data were compared with chi squared or Kruskal Wallis. The number of chronic diseases is the sum of hypertension, diabetes, cancer, respiratory disease, acute myocardial infarction, cerebrovascular disease, rheumatism, kidney infection, liver infection, tuberculosis, pneumonia and herpes zoster.
VITAMIN D LEVELS AND THEIR ASSOCIATION WITH MORTALITY AT THE YEAR 2015
After a mean follow up of 162.1 weeks (95 % CI 161.3-162.9), the number of deaths among participants was 22 (12.6 %), 10 (2.9 %), 24 (3.1 %), and 8 (2.3 %) in those with vitamin D levels < 15, 15-< 20, 20-29, and 30 or more, respectively (p < 0.001). The unadjusted relative risk was 5.421 (95 % CI 2.465-11.92, p < 0.001) and 1.257 (95 % CI 0.5024-3.147 p = 0.8021) and 1.325 (95 % CI 0.6015-2.919 p = 0.4829) for the participants with vitamin D levels < 15, 15-< 20, 20-29, respectively, which after adjusting for covariates, levels of vitamin D lower of 15 remained statistically significant (Table II).

DISCUSSION
The objective of this analysis was to determine the association between low levels of vitamin D and mortality in Mexican population, from the database of the Mexican Health and Aging Study (MHAS).
When reviewing the clinical characteristics of the members of the groups, it was found that levels of vitamin D lower than 15 were associated with older age, female sex, lower scores on cognition, required more aid in BADL, and more chronic diseases, which agrees with the findings of Dobnig et al.(15), and Schottker et al. (17), in German population, as well as by Pilz, and colleagues (16), in Netherland. Consistency was clear in age and comorbidities such as diabetes, but in those studies, neither cognition nor functionality were measured.
We found a striking association of mortality with levels of vitamin D below 15 ng/ml. This association remained even after adjusting for confounding variables such as age, sex, number of chronic diseases, cognition score, and number of basic and instrumental activities of daily living for requiring support, and depression scale score. These results are consistent with findings from other studies that used the similar cut point used in the present study (15-17,29). In the report by Vogt et al. (29), the result is partially explained by frailty status, while in that performed by Dobnig et al. (15), mortality was associated with the groups of participants with median levels of 6 and 13 ng/ml. Mean level of vitamin D was 12 ng/ml in the group of participants with higher mortality in the study of Pilz et al. (16), and below 12 ng/ml in the study of Schottker et al. (17).
Possible explanation for this association, is that the vulnerability could be a marker of another underlying disorder, and is associated with social or environmental factors that may increase the risk of mortality (30). In this case, one possible explanation is frailty syndrome. It has been associated with vitamin D levels below 15 ng/ml found by Ensrud et al. (10) and Pabst et al. (11), while Gutierrez Robledo et al. (12), report it at levels below 12 ng/ml. Frailty is associated with higher mortality (31,32), which could explain the association of the number of deaths found at vitamin D levels below 15.
Both, frailty syndrome and hypovitaminosis D are very common among older persons in Latin America (4,33). Their association has been well established (10-12,29). Although evidence is still limited, several authors have proposed to supplement enough vitamin D (800 to 2000 IU daily) to reach a serum level of 30 ng/ml to help in the prevention and control of frailty (34). A growing number of voices propose to create strategies to improve the status of vitamin D in older adults and the general population to decrease the burden of disease (35) as well as mortality (36,37).
The present study has some limitations. First, the medical conditions of the study population and the activities of daily living are self-reports on the state of health, although several studies have found consistency in self-reports and direct measurements (38). Second, the loss of subjects during follow-up, and analysis of complete cases may have influenced the study results, and produced selection bias (39). It is well known that subjects who do not complete the performance measures in population studies (probably like those not included in the present analysis) are expected to be less healthy, and more likely to die (40), increasing the possibility of survival bias. Despite these limitations, this study has many strengths, including its large sample size of men and women living in the community (which makes it generalizable), its prospective design, the ability to evaluate multiple medical conditions and factors that have been reported previously with an association with adverse outcomes.

