










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNefrología (Madrid)
versión On-line ISSN 1989-2284versión impresa ISSN 0211-6995
Nefrología (Madr.) vol.31 no.1 Cantabria 2011
Quality of life in chronic kidney disease
Calidad de vida en la enfermedad renal crónica
M. Rodrigues Fructuoso , R. Castro , I. Oliveira , C. Prata, T. Morgado
Nephrology Department. Centro Hospitalar de Trás-os-Montes e Alto Douro EPE. Vila Real (Portugal)
ABSTRACT
Background: The evaluation of health-related quality of life (QOL) in chronic kidney disease intends to quantify its consequences, according to the patient's subjective perception.
Aim: To evaluate the health-related QOL in four groups of patients followed at our Nephrology Department: chronic kidney disease (CKD) stages 1-4, kidney transplant (KT), haemodialysis (HD) and peritoneal dialysis (PD) patients.
Patients and Methods: Thirty patients with CKD stages 1-4 and 30 KT patients were randomly selected. All patients from our Haemodialysis and Peritoneal Dialysis Units with capacity to answer the inquiry (37 and 14, respectively) were also selected. The instruments applied were the SF-36 and KDQOL-SF 1.3.
Results: The four groups presented better results in the «Social Functioning» scale (77.68 ± 18.46 in PD; 74.17 ± 29.53 in KT; 66.81 ± 31.39 in CKD 1-4; 62.16 ± 32.84 in HD; p = 0.192). The lowest results appeared in the «General Health» scale (39.92 ± 19.12 in CKD; 45.95 ± 21.56 in HD; 47.13 ± 23.15 in KT; 51.79 ± 18.89 in PD; p = 0.321). Peritoneal dialysis patients achieved the best results in the Physical Health Component, but this difference disappeared after adjustment to confounding factors. Age, gender and haemoglobin level were the variables related with QOL. However, PD patients obtained better scores comparing to HD patients in the following KDQOL-SF scales: «Effects of kidney disease», «Burden of kidney disease» and «Patient satisfaction» (p <0.05).
Conclusions: Health-related QOL was better in peritoneal dialysis patients comparing to haemodialysis patients in specific scales of chronic kidney disease. Age, gender and haemoglobin level interfered with health-related QOL.
Key words: Health-related quality of life, Kidney disease.
RESUMEN
Antecedentes: La evaluación de la calidad de vida (CV) relacionada con la salud en la enfermedad renal crónica pretende cuantificar sus consecuencias en función de la percepción subjetiva del paciente.
Objetivo: Evaluar la CV relacionada con la salud en cuatro grupos de pacientes controlados en nuestro servicio de nefrología: pacientes con insuficiencia renal crónica (ERC) en fases 1 - 4, trasplante renal (TR), hemodiálisis (HD) y diálisis peritoneal (DP).
Pacientes y métodos: De forma aleatoria se incluyeron 30 pacientes con ERC en fases 1 - 4 y 30 trasplantados renales. También se incluyeron todos aquellos pacientes de nuestras Unidades de Hemodiálisis y Diálisis Peritoneal que eran capaces de responder los cuestionarios (37 y 14, respectivamente). Los cuestionarios que se utilizaron fueron el SF-36 y el KDQOL-SF 1.3.
Resultados: Los cuatro grupos obtuvieron mejores resultados en la dimensión "Función social" (77,68 ± 18,46 en DP; 74,17 ± 29,53 en TR; 66,81 ± 31,39 en ERC 1-4; 62,16 ± 32,84 en HD; p = 0,192). Las puntuaciones más bajas se obtuvieron en la dimensión "Salud general" (39,92 ± 19,12 en IRC; 45,95 ± 21,56 en HD; 47,13 ± 23,15 en TR; 51,79 ± 18,89 en DP; p = 0,321). Los pacientes con diálisis peritoneal presentaron los mejores resultados en cuanto a la Salud Física, sin que la diferencia se mantuviese tras la corrección de los factores de confusión. La edad, el sexo y la concentración de hemoglobina fueron las variables que se asociaron con la CV. Sin embargo, los pacientes con DP obtuvieron mejores puntuaciones que los pacientes con HD en las siguientes dimensiones del KDQOL-SF: "Efectos de la enfermedad renal", "Carga de la enfermedad renal" y "Satisfacción del paciente" (p < 0,05).
Conclusiones: La CV relacionada con la salud medida mediante dimensiones específicas de la enfermedad renal crónica fue mejor en pacientes con diálisis peritoneal que en pacientes con hemodiálisis. La edad, el sexo y la concentración de hemoglobina afectan la CV relacionada con la salud.
Palabras clave: Calidad de vida relacionada con la salud, Enfermedad renal.
Background
Health-related quality of life (QOL) assumes an increasing importance as a marker of treatment quality in many chronic diseases. Its evaluation allows the quantification of the diseases consequences according to the patient's subjective perception and enables adjustment of medical decisions to their physical, emotional and social needs. It also improves the adhesion to the therapeutic plan, the quality of the health care provided and the patient survival.
The multiple limitations and complications of patients in advanced stages of chronic kidney disease (CKD) or under renal substitution treatment can contribute to this QOL impairment1.
Diverse psychometric tests have been designed and validated to evaluate health-related QOL. Our purpose in this study was to evaluate the health-related QOL in four groups of CKD patients (CKD stages 1-4, kidney recipients, haemodialysis and peritoneal dialysis patients), using validated and applicable instruments.
Population and methods
Thirty of the 821 CKD patients stages 1-4 (CKD 1-4) and 30 of the 117 transplanted patients followed at our Nephrology Department were randomly selected. Patients at our Haemodialysis Unit (37/43) and Peritoneal Dialysis Unit (14/17) with the capacity of answering to the questionnaires were also admitted in the study.
The instruments applied were the SF-36 (Medical Outcomes Study Short-Form 36) and KDQOL-SF 1.3 (Kidney Disease and Quality of Life Short-Form).
The SF-36 is a generic questionnaire translated in more than 40 languages and already validated in Portugal2-5. It consists of 36 items grouped in eight scales that evaluate different areas of health: Physical Functioning, Role Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role Emotional and Mental Health. These scales are grouped in two summary measures: Physical Health and Mental Health. This instrument was applied in the CKD stages 1-4 and kidney transplanted patients (KT).
KDQOL-SF 1.3 is a questionnaire that includes not only the SF-36 scales but also specific dimensions of chronic kidney disease. This dimensions include 43 items that can be summarized in 12 scales: Symptom/problem list, Effects of kidney disease, Burden of kidney disease, Work status, Cognitive function, Quality of social interaction, Sexual function, Sleep, Social support, Dialysis staff encouragement, Overall health and Patient satisfaction. It's a reproducible questionnaire that was validated by the KDQOL Working Group studies6. It was applied in our study to haemodialysis (HD) and peritoneal dialysis (PD) patients.
The two cited instruments have punctuation from zero to 100, directly related with the QOL. In resume, higher punctuations relate to better quality of life. Our data was analyzed in a program produced by the KDQOL Working Group (www.gim.med.ucla.edu/kdqol/). The remaining statistical analysis was performed with the program Statistical Package of Social Sciences (SPSS 18.0). The quantitative variables were expressed as mean ± standard deviation and qualitative variables as absolute numbers and percentages. We studied the association between the groups in qualitative variables by chi-square test or the contingency coefficient, as appropriate. For the quantitative variables, after checking normality with the Kolmogorov-Smirnov test, the T-Student test or Mann-Whitney were used for two groups and the table ANOVA or Kruskal-Wallis for the four groups, as appropriate. Finally, we performed a multivariate linear regression analysis in each of the groups for those variables significant in the univariate analysis or clinically relevant.
Results
The peritoneal dialysis patients were younger than the other patients (38.9 ± 13.3 years in PD, 51.8 ± 10.8 years in transplanted patients, 62.2 ± 18.3 years in CKD 1-4, 67.3 ± 14.9 years in HD; p <0.001). There was no gender predominance in the four groups (43.3% of men in CKD, 50.0% in KT, 56.8% in HD and 57.1% in PD, p = 0.702) (Table 1). The mean time on dialysis was not significantly different in haemodialysis and peritoneal dialysis patients (6.1 ± 6.5 vs 1.9 ± 1.3 years, p = 0.40). The mean time after kidney transplantation was 8.7 ± 5.4 years.
Table 1. Demographic and clinical characteristics 
The majority of haemodialysis patients were treated with on-line hemodiafiltration (56.8%) and all patients in peritoneal dialysis, except one, were in automatic peritoneal dialysis.
Twenty three patients were diabetic (20.7%), but the prevalence of diabetes was not different between the groups (p = 0.175). On the other hand, the prevalence of heart failure was tendencially higher in the haemodialysis group (HD: 40.5%; CKD: 23.3%; PD: 14.3%; KT: 13.3%; p = 0.050).
The dialysis dose was adequate in the two groups under dialytic treatment (HD: spKt/V = 2.08 ± 0.54; PD: weekly urea Kt/V = 2.25 ± 0.48 and weekly creatinine clearance = 85 ± 30 L/1.73 m2/week). The creatinine clearance was 59.3 ± 34.6 ml/min/1.73 m2 in CKD 1-4 and 74.5 ± 42.5 ml/min/1.73 m2 in the transplanted patients (p = 0.132).
All patients presented a similar albuminemia level (CKD: 3.71 ± 0.40 g/dl, KT: 3.56 ± 0.46 g/dl, HD: 3.36 ± 0.44 g/dl, PD: 3.35 ± 0.33; p = 0.231). The mean haemoglobin level of the CKD 1-4 (13.2 ± 1.7 g/dl) and transplanted patients (13.1 ± 1.9 g/dl) was higher than that of the haemodialysis (11.9 ± 1.2 g/dl) and peritoneal dialysis patients (11.5 ± 1.8 g/dl, p <0.001). The majority of haemodialysis (81.1%) and peritoneal dialysis patients (64.3%) were treated with recombinant erythropoietin (EPO). In contrast, only 23.3% of CKD patients and 16.7% of transplanted patients were under that treatment.
The best results of the SF-36 in the four groups were found in the «Social Functioning» scale of the Mental Health Component (PD: 77.68 ± 18.46; KT: 74.17 ± 29.53; CKD: 66.81 ± 31.39; HD: 62.16 ± 32.84; p = 0.192) (Table 2). The worst results were related to the «General Health» scale of the Physical Health Component (CKD: 39.92 ± 19.12; HD: 45.95 ± 21.56; KT: 47.13 ± 23.15; PD: 51.79 ± 18.89; p = 0.321).
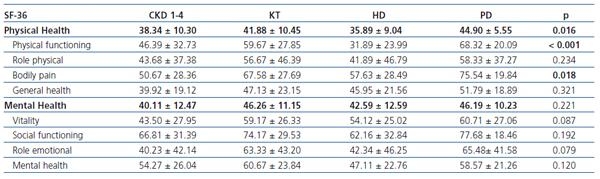
Peritoneal dialysis patients accomplished better results in the Physical Health Component (PD: 44.90 ± 5.55; KT: 41.88 ± 10.45; CKD: 38.34 ± 10.30; HD: 5.89 ± 9.04; p = 0.016). They achieved the best results of this component in the following scales: «Physical Functioning» (PD: 68.32 ± 20.09; KT: 59.67 ± 27.85; CKD: 46.39 ± 32.73; HD: 31.89 ± 23.99; p <0.001) and «Bodily Pain» (PD: 75.54 ± 19.84; KT: 67.58 ± 27.69; HD: 57.63 ± 28.49; CKD 50.67 ± 28.36; p = 0.018). All scales of the Mental Health Component had similar punctuations in the four groups of patients (p = NS).
The second item of the SF-36 questionnaire, that compares health in general relatively to the previous year, was evaluated separately taking in consideration that is not included in the final score. This item is punctuated from one to five according to the patient's answer: 1,much better; 2, a little better; 3, almost the same; 4, a little worse; 5, much worse. The peritoneal dialysis patients were the only ones to indicate an improvement in their health relatively to the previous year (CKD: 3.0 ± 1.1; KT: 3.0 ± 1.1; HD: 2.9 ± 1.0; PD: 2.1 ± 0.8; p <0.05).
In the kidney disease specific dimensions of the KDQOL-SF 1.3 (Table 3), the peritoneal dialysis patients had better results comparing to haemodialysis patients in the following scales: «Effects of kidney disease» (73.83 ± 17.89 vs 59.38 ± 18.76; p = 0.019), «Burden of kidney disease» (58.65 ± 27.31 vs 26.35 ± 18.58; p <0.001), «Work status» (50.00 ± 44.72 vs 19.85 ± 9.46; p = 0.001), «Overall Health» (76.67 ± 19.69 vs 46.49 ± 22.51; p = 0.021) and «Patient satisfaction» (84.72 ± 20.67 vs 70.02 ± 20.43; p <0.001). In the remaining scales, values were similar for both groups.
Table 3. Results of KDQOL-SF 1.3 (specific scales of kidney disease) 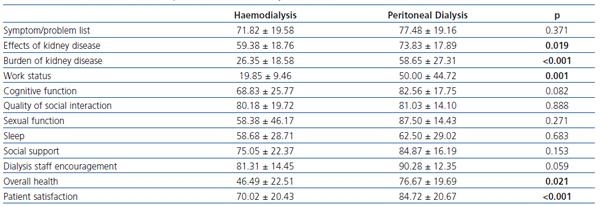
After adjustment in multivariate linear regression analysis for variables like age, gender, heart failure, time on dialysis, haemoglobin level and creatinine clearance, the scales that remained unchanged were «Effects of kidney disease», «Burden of kidney disease» and «Patient satisfaction» of the KDQOL-SF 1.3. Age, gender and haemoglobin level were the variables associated with the remaining scales that presented different results between groups in univariate analysis («Physical Health Component», «Physical functioning», «Bodily pain», «Work status» and «Overall health») (Table 4). Age was inversely related to the punctuation and haemoglobin level presented a direct relation with higher scores. Male patients of the CKD 1-4 group presented worst results than females in the «Bodily pain» scale (p = 0.039).
Table 4. Significant results of the linear regression model after adjustment for age,
gender and haemoglobin level (Hb) 
Finally, we evaluated the association between the Mental Health Component and the treatment with antidepressants. The patients under antidepressant treatment (four patients with CKD stages 1-4, three transplanted patients, seven haemodialysis patients and one patient in peritoneal dialysis) had worst results in the Mental Health Component when compared with the remaining patients, not treated with antidepressants (36.62 ± 10.96 vs 44.17 ± 12.03; p <0.05).
Discussion
The two summary measures of the SF-36 allow a fast evaluation of the health-related QOL, with scarce loss of information when the eight scales are resumed in the two main components, Physical and Mental7,8.
Several studies have already compared the QOL of dialysis patients with the general population, the majority disclosing the negative impact of chronic kidney disease and its treatments9-14. Those results are however, not confirmed in other series15,16. In our view, the present study, even with the limitation of being an observational cross-sectional study with a small number of patients, has the particularity of evaluating the health-related QOL in four groups of patients with CKD in various phases and under different renal replacement treatments (HD, PD and kidney transplant).
The worst results were registered in the scale «General Health» of the Physical Health Component. In other type of diseases, a greater impact in Physical Health comparing to Mental Health was also found17. This situation can be explained by the psychological adaptation of the sick person to the chronic illness, with a declining repercussion of the disease in its Mental Health. In our study, Physical Health was better in peritoneal dialysis patients but these differences disappeared after adjustment to confounding factors such as age and gender. Curiously, the transplanted patients didn´t achieve better results in any scale of the Physical or Mental Health Components, although these patients proved previously in other studies to have a better QOL comparing to dialysis patients18,19. Transplanted patients received their new kidney 8.7 years ago, which implied a gradual adaptation and possibly the disappearance of the health improvement feeling relatively to the pre-transplantation period.
Comparisons of QOL between haemodialysis and peritoneal dialysis patients are not consensual20,21. In our study, the PD group achieved better scores in scales like «Effects of kidney disease», «Burden of kidney disease» and «Patient satisfaction» and these results were maintained after adjustment for confounding factors. Our young peritoneal dialysis patients selected this dialytic technique to keep their active lives and the possibility to study or work. So, they are a more autonomous and motivated group. On the other hand, our haemodialysis patients are integrated in a Hospital Unit that selects older, sicker and more dependent persons. These facts may be a partial explanation for the better results of our PD patients. Another factor that may contribute for the lesser effect of the kidney disease in the QOL and better patient satisfaction may be the continuous treatment of uremia in PD. Individual characteristics of personality are obviously not evaluated in our study, but must also be considered when analysing these results.
Variables like age, gender and haemoglobin level were related with scales like «Physical Health Component», «Physical functioning», «Bodily pain», «Overall health» and «Work status». Although our PD patients had haemoglobin levels adequately corrected according to international guidelines, this modifiable factor was associated with worst results in «Work status». Taking in consideration that this specific group of patients was young and more active, the anemia correction for higher haemoglobin levels may help improve their QOL.
Conclusions
Health related QOL was better in peritoneal dialysis patients comparing to haemodialysis patients in scales such as «Effects of kidney disease», «Burden of kidney disease» and «Patient satisfaction». The worst results in the four groups were found in the Physical Health Component. Variables found to be related with QOL were age, gender and haemoglobin level. Patients under antidepressant treatment had worst results in the Mental Health Component.
The adaptation to a chronic illness is a physical, psychological and social process. The attention of the health team to the patient's subjective perception about his state of health can be determinant in achieving the best medical intervention and improving survival.
Referencias Bibliográficas
1. Sanjeev KM, Lori A, Edith F, John KM, Steven F. Self-assessed physical and mental function of haemodialysis patients. Nephrol Dial Transplant 2001;16:1387-94. [ Links ]
2. Shieley JC, Bayliss MS, Keller SD, et al. SF-36 Health Survey annoted bibliography (1st ed). Boston MA: The Health Institute, New England Medical Center, 1997. [ Links ]
3. Ferreira P. Criação da Versão Portuguesa do MOS SF-36, Parte II. Testes de Validação. Acta Medica Portuguesa 2000;13:119-27. [ Links ]
4. Ferreira P. Criação da Versão Portuguesa do MOS SF-36, Parte I. Adaptação Cultural e Linguística. Acta Medica Portuguesa 2000;13:55-66. [ Links ]
5. Severo M, Santos AC, Lopes C, Barros H. Fiabilidade e Validade dos conceitos teóricos das dimensões de saúde física e mental da versão portuguesa do MOS SF-36. Acta Medica Portuguesa 2006;19:281-8. [ Links ]
6. Kusumota L. Evaluation of Health-Related Quality of Life in hemodialysis patients, Doctoral Dissertation. University of São Paulo at Ribeirão Preto College of Nursing, 2005. [ Links ]
7. Ware JE, Kosinki M, Keller SD. SF-36 physical and mental health summary scales: a user's manual (4th printing, revised). Boston, MA: Health Institute, 1994. [ Links ]
8. Ware JE, Kosinki M , Bayliss MS, Mchorney CA, Rogers WH, Raczek A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the Medical Outcome Study. Med Care 1995;33:AS264-AS279. [ Links ]
9. Kurtin PS, Davies AR, Meyers KB, DeGiacomo JM, Kantz ME. Patients-based health status measures in out-patient dialysis: early experiences in developing an outcome assessment program. Med Care 1992;30:MS136-MS149. [ Links ]
10. Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life: a conceptual model of patients outcomes. JAMA 1995;273:59-65. [ Links ]
11. Khan IH, Garratt AM, Kumar A, et al. Patient's perception of health on renal replacement therapy: evaluation using a new instrument. Nephrol Dial Transpl 1995;10:684-9. [ Links ]
12. Kimmel PL, Peterson RA, Wheis LK, et al. Behavioral compliance in hemodialysis patients. J Am Soc Nephrol 1995;5:1826-34. [ Links ]
13. Merkus MP, Jager KJ, Dekker FW, Boeschoten EW, Stevens P, Krediet RT, NECOSAD Study Group. Quality of life in patients on chronic dialysis: self-assessment 3 months after the start of treatment. Am J Kid Dis 1997;29:584-92. [ Links ]
14. DeOreo PB. Hemodialysis patient-assessed functional health status predicts continued survival, hospitalization and dialysis-attendance compliance. Am J Kid Dis 1997;30:204-12. [ Links ]
15. Auer J, Gokal R, Stout JP, et al. The Oxford/Manchester Study of dialysis patients. Scand J Urol Nephrol 1990;131:31-7. [ Links ]
16. Tarlov AR, Ware JE, Greenfield S, Nelson EC, Perrin E, Zubkoff M. The medical outcome study: an application of methods for monitoring the results of medical care. JAMA 1989;262:907-13. [ Links ]
17. Hayes RD, Wells KB, Sherbourne CD, Rogers W, Spritzer K. Functional and well-being outcomes of patients with depression compared with chronic general medical illness. Arch Gen Psychiatry 1995;52:11-9. [ Links ]
18. Evans RW, Manninen DL, Garrison PL, et al. The quality of life of patients with end stage renal disease. N Engl J Med 312;553-9. [ Links ]
19. Kutner NG, Brogan D, Kutner MH. End stage renal disease treatment modality and patient's quality of life. Am J Nephrol 1986;6:396-402. [ Links ]
20. Fox E, Peace K, Neale TJ, Morrison RBI, Hatfield PJ, Mellsop G. Quality of life for patients with end-stage renal failure. Renal Failure 1991;13:31-5. [ Links ]
21. Wolcott DL, Nissenson AR. Quality of life in chronic dialysis patients: a critical comparison of continuous ambulatory peritoneal dialysis (CAPD) and hemodialysis. Am J Kid Dis 1988;11:402-12. [ Links ]
![]() Correspondence:
Correspondence:
Mónica Rodrigues Fructuoso,
Nephrology Department,
Centro Hospitalar de Trás-os-Montes e Alto Douro EPE,
Avenida da Noruega, 5000-508, Vila Real, Portugal
monicafructuoso@portugalmail.pt
Sent to: 17 Jun. 2010
Accepted: 1 Jul. 2010

