










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 no.3 Madrid may./jun. 2016
https://dx.doi.org/10.20960/nh.257
TRABAJO ORIGINAL / Pediatría
Association of body composition indices with insulin resistance in European adolescents: the HELENA study
Asociación de índices de composición corporal con resistencia a la insulina en adolescentes europeos: el estudio HELENA
María Sese1,2, Luis A. Moreno1,2, Laura Censi3, Cristina Bresidenassel4, Marcela González-Gross5, Michael Sjöström6, Yannis Manios7, Molnár Dénes8, Jean Dallongeville9, Kurt Widhalm10, Frederic Gottrand11, Steffan De-Henauw12, Ascensión Marcos13, Manuel Castillo-Garzón14 and David Jiménez-Pavón15
1GENUD Research Group
2Department of Psychiatry and Nursing. Facultad de Ciencias de la Salud. Universidad de Zaragoza. Zaragoza, Spain.
3Council for Agricultural Research and Economics. Research Center for Food and Nutrition. Rome, Italy.
4Institut für Ernährungs- und Lebensmittelwissenschaften-Humanernährung. Rheinische Friedrich-Wilhelms Universität. Bonn, Germany.
5ImFINE Research Group. Department of Health and Human Performance. Facultad de Ciencias de la Actividad Física y del Deporte (INEF). Universidad Politécnica de Madrid. Madrid, Spain.
6Unit for Preventive Nutrition. Department of Biosciences and Nutrition. Karolinska Institutet. Sweden.
7Department of Nutrition and Dietetics. Harokopio University. Greece.
8Department of Pediatrics. University of Pécs. Pécs, Hungary.
9Research Institute of Child Nutrition Dortmund. Dortmund, Germany.
10Division of Clinical Nutrition and Prevention. Department of Pediatrics. Medical University of Vienna. Vienna, Austria.
11Faculté de Médecine. Université de Lille. France.
12Department of Public Health. Ghent University. Ghent, Belgium.
13Immunonutrition Research Group. Department of Metabolism and Nutrition. Instituto de Ciencia y Tecnología de Alimentos y Nutrición. Madrid, Spain.
14Department of Medical Physiology. Facultad de Medicina. Universidad de Granada. Granada, Spain.
15GALENO Research Group. Department of Physical Education. School of Education. Universidad de Cádiz. Puerto Real, Cádiz. Spain
The HELENA study takes place with the financial support of the European Community Sixth RTD Framework Programme (Contract FOOD-CT-2005- 007034). This study was also supported by the Spanish Ministry of Health: Maternal, Child Health and Development Network (number RD08/0072) (LMA) and (CIBERobn CB12/03/30038), and co-financed by the European Regional Development Fund (MICINN-FEDER).
Dr. Jiménez-Pavón was supported by a grant from the Spanish Ministry of Economy and Competiveness (MINECO) (grant no:RYC-2014-16938).
ABSTRACT
Background: The different body components may contribute to the development of insulin resistance and type 2 diabetes mellitus. The aim of the present study was to examine the association of fat mass and fat free mass indices with markers of insulin resistance, independently of each other and giving, at the same time, gender-specific information in a wide cohort of European adolescents.
Methods: A cross-sectional study in a school setting was conducted in 925 (430 males) adolescents (14.9 ± 1.2 years). Weight, height, anthropometric, bioimpedance and blood parameters were measured. Indices for fat mass and fat free mass, and homeostatic model assessment (HOMA) were calculated. Multiple regression analyses were performed adjusting for several confounders including fat free mass and fat mass when possible.
Results: Indices of fat mass were positively associated with HOMA (all p < 0.01) after adjusting for all the confounders including fat free mass indices, in both sexes. Fat free mass indices were associated with HOMA, in both males and females, after adjusting for center, pubertal status, socioeconomic status and cardiorespiratory fitness, but the associations disappear when including fat mass indices in the adjustment's model.
Conclusion: Fat mass indices derived from different methods are positively associated with insulin resistance independently of several confounders including fat free mass indices. In addition, the relationship of fat free mass with insulin resistance is influenced by the amount of fat mass in European adolescents. Nevertheless, future studies should focus not only on the role of fat mass, but also on other body components such as fat free mass because its role could vary depending of the level and distribution of fat mass.
Key words: Insulin resistance. Adolescent. Body fat. Obesity.
RESUMEN
Antecedentes: los diferentes componentes corporales pueden contribuir al desarrollo de resistencia a la insulina y diabetes mellitus de tipo 2. El objetivo del presente estudio fue examinar la asociación entre la masa grasa y la masa libre de grasa con marcadores de resistencia a la insulina, valorando de forma independiente cada uno de ellos y aportando información específica por sexo, en una amplia cohorte de adolescentes europeos.
Métodos: se realizó un estudio transversal en el ámbito escolar en 925 (430 varones) adolescentes (14,9 ± 1,2 años). Se midieron peso, talla, pliegues cutáneos e impedancia bioeléctrica. Se calcularon índices de masa grasa y libre de grasa y se calculó el índice HOMA. Se realizaron análisis de regresión múltiple ajustándolos según varios factores de confusión, incluyendo la masa libre de grasa y masa grasa cuando fue posible.
Resultados: los índices de masa grasa se asociaron positivamente con HOMA (todos p < 0,01) después de ajustarlos según todos los factores de confusión, incluidos los marcadores de masa libre de grasa, en ambos sexos. Los índices de masa libre de grasa se asociaron con HOMA, tanto en hombres como en mujeres, después de ajustar por país, estadio puberal, nivel socio-económico y capacidad cardiorrespiratoria, pero las asociaciones desaparecieron al incluir marcadores de masa grasa en el modelo de ajuste.
Conclusión: índices de masa grasa obtenidos según diferentes métodos se asocian con la resistencia a la insulina, independientemente de varios factores de confusión, incluyendo los índices de masa libre de grasa. Además, la cantidad de masa grasa influye en la relación de la masa libre de grasa con resistencia a la insulina en adolescentes europeos. Los estudios futuros deberían centrarse no solo en el papel de la masa grasa, sino también en el de otros componentes corporales como la masa libre de grasa, ya que su papel podría variar dependiendo del nivel y distribución de masa grasa.
Palabras clave: Resistencia a la insulina. Adolescente. Grasa corporal. Obesidad.
Abbreviations
BIA: Bioelectrical impedance or bioimpedance.
BMI: Body mass index.
CRF: Cardiorespiratory fitness.
HELENA-CSS: Healthy Lifestyle in Europe by Nutrition in Adolescence Cross-Sectional Study.
HOMA: Homeostatic model assessment.
FAS: Family affluence scale.
FM: Fat mass.
FMS: Fat mass calculated by Slaughter.
FMSI: Fat mass calculated by Slaughter index.
FFM: Fat-free mass.
FFMB: Fat-free mass estimated from BIA.
FFMBI: Fat-free mass estimated from BIA index.
FFMS: Fat-free mass calculated by Slaughter.
FFMSI: Fat-free mass calculated by Slaughter index.
QUICKI: Quantitative insulin sensitivity check index.
T2DM: Type 2 diabetes mellitus.
Introduction
Insulin resistance is considered as a precursor of Type 2 diabetes mellitus (T2DM), being an emerging problem among children and adolescents (1), and leading to long-term serious health consequences (2). The main risk factor for insulin resistance and T2DM is obesity, as defined by an excess of body fat (3). In adolescents, the most frequently identified features are diabetes precursors, as impaired glucose tolerance, and especially insulin resistance.
In the literature, a positive association between adiposity and insulin resistance in adolescents has been frequently described. However, in most cases simple methods to assess total body fat, such as the body mass index (BMI), have been used (4-6). Other studies used different anthropometric measurements/indices like sum of skinfold thickness (4,7), waist circumference (8) or waist-hip ratio (3). However, in adolescents, there is limited information on the role of different body components (fat and fat free mass) on insulin resistance as these indices require specific measurement methods, such as bioelectrical impedance analysis (BIA) (5,9).
The majority of the studies observed a positive association between total and abdominal body fat with insulin resistance (10). However, there are limited studies assessing the effect of other body composition compartments as fat-free mass. Fat-free mass is an indicator of muscle amount which is an important organ in insulin metabolism and action (11).
The purpose of this study was to examine the association between different body components, assessed through anthropometric and BIA methods, and insulin resistance after adjusting for several confounders, in a cohort of European adolescents.
Methods
The HELENA-cross sectional study (HELENA-CSS) is a multi-centre study performed in ten European cities from nine countries: Heraklion and Athens (Greece), Dortmund (Germany), Ghent (Belgium), Lille (France), Pécs (Hungary), Rome (Italy), Stockholm (Sweden), Vienna (Austria) and Zaragoza (Spain). This study was designed to obtain reliable and comparable data on the nutritional status of urban European adolescents (12.5-17.5 years). The total sample of the HELENA-CSS fulfilling all the inclusion criteria was 3,528 adolescents. It was decided to obtain blood samples in one third of the total HELENA-CSS sample. The total sample size in which we obtained blood samples was 1,089. From the total number of adolescents with blood samples, 925 (430 males) had valid data for BMI, fat mass (FM)/fat-free mass (FFM) indices and homeostatic model assessment (HOMA) index, constituting the overall sample included in the current study. The sample size varied through the different variables used for the analysis (the specific sample sizes are defined in the corresponding tables). Data collection took place from 2006 to 2007 at school setting. Detailed description of the HELENA-CSS sampling and recruitment approaches, standardization and harmonization processes, data collection, analysis strategies, quality control activities, and inclusion criteria have been published elsewhere, with a complete description of ethical issues and good clinical practice (12,13).
ETHICS STATEMENT
The study protocol was approved by the Ethics Committee at each study centre following the ethical guidelines of the Declaration of Helsinki 1964, the Good Clinical Practice, and the legislation about clinical research in humans. The original names of the ten ethics committees/institutional review boards were: 1) Ethics Committee of the Harokopio University from Athens; 2) Ethics Committee of the Medicine's University from Dortmund; 3) Ethics Committee from Ghent University Hospital; 4) Ethics Committee of the University of Crete School of Medicine from Heraklion; 5) Protection committees people from Lille; 6) A Pecsi Orvostudomanyi és Egészségtudomanyi Központ Regionalis Kutatas-Etikai Bizottsaga from Pècs; 7) Ethics Committee of Medical Activities of the University of Naples Federico II, Naples; 8) Regional Ethics Committee from Stockholm; 9) Ethics Committee of the Medicine's University from Vienne, and 10) Ethics Committee of clinic research of Aragón from Zaragoza. Written informed consent was obtained from the parents (or guardian) and adolescents participating in the study.
COVARIATES
Socioeconomic status was stablished by using the Family Affluence Scale (FAS), which is based on the concept of material conditions in the family to base the selection of items. Currie et al. (14) chose a set of items which reflected family expenditure and consumption that were relevant to family circumstances. Possessing these items was considered to reflect affluence and their lack, on the other hand, material deprivation. The FAS has been previously used in the HELENA-CSS as an index of socioeconomic status (15). Pubertal status was evaluated by experienced physicians according to the criteria of Tanner and Whitehouse (16).
Cardiorespiratory fitness (CRF) was measured by the progressive 20 m shuttle run test. This test required the subjects to run back and forth between two lines set 20 m apart following a running pace determined by audio signals and with an initial speed of 8.5 km/h, increasing by 0.5 km/h every minute (1 minute equals one stage). The test was finished when the adolescent failed to reach the end lines concurrent with the audio signals on two consecutive occasions and the final score was computed as the number of stages completed (precision of 0.5 stages).
BODY COMPOSITION
Anthropometry
The anthropometric method followed in the HELENA-CSS has been described in detail by Nagy et al. (17). In brief, body height was measured to the nearest 0.1 cm with a stadiometer (SECA 225; SECA, Hamburg, Germany) while adolescents were standing barefoot. Body mass was determined to the nearest 0.05 kg using a balance scale (SECA 861; SECA, Hamburg, Germany) with the subject in their underwear. BMI was calculated as body mass (kg) divided by height (m) squared. A set of six skinfold thicknesses (biceps, triceps, subscapular, suprailiac, thigh and medial calf) were measured three consecutive times on the left side of the body, with a Holtain caliper (Holtain, Ltd., Wales, UK) to the nearest 0.2 mm. The waist circumference was measured using a non-elastic tape (SECA 200; SECA, Hamburg, Germany) to the nearest 0.1 cm, according to Lohman's anthropometric standardization reference manual (18). In every city, the same trained investigator made all skinfold thickness measurements. For all the skinfold thickness measurements, intra-observer technical errors of measurement were smaller than 1 mm and reliability, greater than 95%. Inter-observer reliability for skinfolds was higher than 90% (17).
We calculated FM percentage (% FM) from skinfold thickness measurements using the Slaughter's equations (19) which have shown to be a valid equation in adolescents (20). FFM Slaughter (FFMS) in kilograms was derived by subtracting fat mass from total body weight.
Bioelectrical impedance analysis
For BIA measurements, a classical tetra-polar bioelectrical device was used by means of a 50 KHz BIA 101 AKERN (Akern Srl., Firenze, Italy). Standard instructions for BIA measurements were followed (21). FFM was estimated from BIA (FFMB) as marker of muscle mass using validated formulas and, consequently, FM from BIA (FMB) was calculated by subtraction.
Fat mass and fat-free mass indices
FM and FFM indices were calculated by dividing FM or FFM by the square of height in meters as proposed in previous studies (22).
BLOOD SAMPLES
Detailed blood handling procedures have been described elsewhere (23). Serum concentrations of glucose and insulin were measured after an overnight fast. The HOMA index was calculated as: (fasting insulin [pmol/l]/6·945) x (fasting glucose [mmol/l]/22·5] (24). A quantitative insulin sensitivity check index (QUICKI) was calculated as QUICKI = 1/(log insulin [μIU/mL] + logglucose [mg/dl]) (25).
STATISTICAL ANALISYS
The data are presented as mean ± standard deviation, unless otherwise stated. To achieve normality in the residuals, sum of six skinfold thickness,% FM, FM Slaughter (FMS), FMS index (FMSI) and FMB index (FMBI) were transformed to the natural logarithm and HOMA was raised to the power of ⅓.
Multiple linear regression models were used to study the associations of both indices of FM and FFM with HOMA (outcome), after adjusting for pubertal status, socioeconomic status, country, indices of FM or FFM and cardiorespiratory fitness. Regression analysis was performed for different models in table II. Model I included pubertal status, socioeconomic status and country (entered as dummy variable) as confounders. Model II included model I plus the corresponding FFM index. Model III included model II plus cardiorespiratory fitness. In table III model I was similar to table II and model II included model I plus the corresponding FM index. Model III included model I plus cardiorespiratory fitness and model IV included model III plus the corresponding FM index. Sensitivity analyses were performed using QUICKI instead of HOMA and the results did not change (data not shown).


The analyses were performed using the Predictive Analytics SoftWare (PASW, version 20; SPSS Inc., Chicago, IL, USA) and the level of significance was set to 0.05.
Results
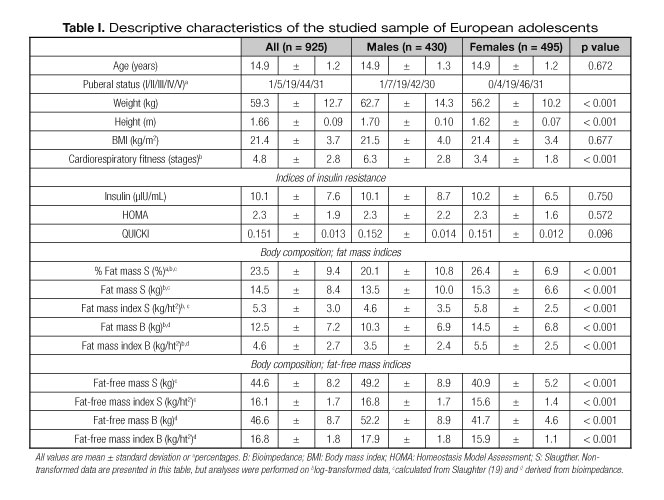
Table I shows the descriptive characteristics of the study sample. All fat mass indicators were significantly higher in females than in males. At the opposite all fat-free mass indicators were higher in males than in females.
The results of the multiple linear regression models showing the association of indices of body fat with HOMA after adjusting for country, pubertal status and socioeconomic status (model I), FFM indicators (model II: model I plus corresponding FFM indicators) and cardiorespiratory fitness (model III: model II plus cardiorespiratory fitness) are presented in table II for males and females. In males, all indicators of FM were positively associated with HOMA (all p < 0.01) in model I, II and III. In females, all indicators of FM were positively associated with HOMA in model I and II (all p < 0.001) but only FMS and FMSI were associated with HOMA in model III (p < 0.01).
Table III shows the association of indicators of FFM with HOMA after adjusting for country, pubertal status and socioeconomic status (model I), FM indicators (model II: model I plus corresponding FM indicator) or cardiorespiratory fitness (model III: model I plus cardiorespiratory fitness) and FM indicator and cardiorespiratory fitness simultaneously (model IV: model III plus the corresponding FM indicator) for males and females. In males, FFMB was positively associated with HOMA in models I and III (both p < 0.001), but not in models including adjustments by FM indicators (models II and IV). FFMBI was significantly associated with HOMA in all the models of adjustment (all p < 0.001). In females, all the FFM indices were significantly associated with HOMA in model I (all p < 0.05); while FFMB and FFMBI were associated with HOMA in model III. No FFM indicator was associated with HOMA in models including adjustment by FM indicators (models II and IV).
Discussion
The main finding of our study indicates that all the FM indices derived from different methods are positively associated with indices of insulin resistance independently of several confounders including FFM as index of muscle mass in both genders. Moreover, FFM seem to be related with insulin resistance in some cases but this association is mainly mediated by FM component, and when the relationship is adjusted by FM significance disappeared and the direction of this turned on negative (without significance).
Our results concur with recent published data in which the relationship between adiposity (triceps and subscapular skinfold thickness) and total body fat from dual energy X-ray absorptiometry in their associations with insulin resistance (HOMA) was analyzed for a large sample of US adolescents (26). They found that triceps and subscapular skinfold thicknesses estimate insulin resistance and identify those at highest risk for insulin resistance. Skinfold thickness provides an inexpensive and widely applicable measure of fatness that is appropriate for studies of insulin resistance and perhaps other metabolic variables in adolescents. Moreover, Carneiro et al. (2014) showed in 148 adolescents how several anthropometric indices were statistically and positively correlated to HOMA, however, any index of FFM was considered in this study (27). Weding VK et al. described in 1,298 adolescents that one of the best predictor of HOMA was percentage of body fat (BIA) suggesting that this can be attributed partly to the ability of percentage body fat to model HOMA among leaner participants (28). However, it is of importance to highlight that none of the cited studies studied the role of muscle mass neither accounted in their analyses for indices of muscle mass derived from Slaughter or BIA, which in some cases could affect these kinds of relationships. In this regard, our findings indicate the positive association between indices of fat mass and insulin resistance remains significant after adjusting for several confounders including muscle components in both genders.
On the other hand, the specific role of muscle components on insulin resistance has been little studied. Lee et al. (2013) studied the relationship of insulin sensitivity with intermusular adipose tissue, skeletal muscle mass (whole-body magnetic resonance imaging) and quality in 40 obese adolescents boys (29). They reported intermusular adipose tissue and skeletal muscle quality, but not muscle mass, were associated with insulin sensitivity in obese adolescent boys after adjusting for pubertal status and race. However, Unni et al. (2009) analyzed the association of muscle mass (apendicular lean soft tissue) and body fat percentage (dual-energy X-ray absorptiometry) with insulin sensitivity in 51 young Indian men. They showed body fat percentage, BMI and muscle mass correlated with insulin resistance. Moreover, in the stepwise multiple linear regression model only BMI and muscle mass enter in the model and explained 49% of the variance in insulin sensitivity (30). Despite using precise methods to assess muscle mass, these studies did not concluded in the same direction regarding the role of muscle mass on insulin resistance/sensitivity. Some aspects that could contribute to the controversy results between studies are the lack of a strong statistical adjustment model and the sample size of the studies. However, our study showed in an initial model that muscle mass was positively associated with insulin resistance in 925 European adolescents after adjusting for pubertal status, socioeconomic status, country and cardiorespiratory fitness. Moreover, when FM was included in the adjustment's model the association disappeared and the direction of association was inverted. These findings indicated that FM is a mediation factor in the role of muscle mass on insulin resistance in European adolescents.
Despite the fact that muscle is an important location for glucose disposal and insulin sensitivity, it is plausible that a low muscle mass and reduced muscle oxidation capacity (31) may act as determinant of whole-body fat oxidation and therefore, fat balance (32), thereby creating an interaction between fat and muscle mass as underlying mechanism related with insulin resistance.
The overall findings from this research could be useful for future studies in considering the different body components and adjustments when studying the relationship of body composition with insulin resistance. Although the study is not representative enough to recommend the generalization of its results to the population, it is plausible to suggest that the interaction between body components and insulin resistance could have a similar pattern in other adolescent populations, making these findings more interesting.
The present study has several limitations. Due to its cross-sectional design, the observed associations cannot be interpreted to reflect causal relationships. In addition, body composition has been measured with indirect methods (Slaughter equation and an estimating formula from BIA). However, several studies considered these methods as valid and accurate tools (18,19,33). Although FFM may be considered as an index of muscle mass, the way it was measured could include some bias as FFM also includes bone and residual mass. An important strength is the large and heterogeneous sample with gender-specific information, to control for several confounders including indices of fat mass and muscle.
Fat mass indices derived from different methods are positivity associated with insulin resistance independently of several confounders including fat free mass indices. In addition, the relationship of fat-free mass with insulin resistance is mediated by the amount of fat mass in European adolescents. Nevertheless, future studies should focus not only on the role of fat mass, but also in other body components such as fat free mass because its role could vary depending of the level and distribution of fat mass in adolescents.
Acknowledgements
We gratefully acknowledge all participating children and adolescents, and their parents and teachers for their collaboration. We also acknowledge all the members involved in the field work for their efforts and great enthusiasm.
There are no relationships with industry. Authors have (none) no conflicts of interest. All the authors are independent of commercial funding agencies. All authors had full access to all of the data (including statistical reports and tables) and take responsibility for the integrity and accuracy of the data and their analyses. Many thanks to Petra Pickert and Anke Carstensen for their contribution to laboratory work.
References
1. Mizokami-Stout K, Cree-Green M, Nadeau KJ. Insulin resistance in type 2 diabetic youth. Curr Opin Endocrinol Diabetes Obes 2012;19(4):255-62. [ Links ]
2. Cizza G, Brown RJ, Rother KI. Rising incidence and challenges of childhood diabetes. A mini review. J Endocrinol Invest 2012;35(5):541-6. [ Links ]
3. Faria ER, Franceschini Sdo C, Peluzio Mdo C, Sant'ana LF, Priore SE. Correlation between metabolic and body composition variables in female adolescents. Arq Bras Cardiol 2009;93(2):119-27. [ Links ]
4. Addo OY, Himes JH. Are field measures of adiposity sufficient to establish fatness-related linkages with metabolic outcomes in adolescents? Eur J Clin Nutr 2014;68(6):671-6. [ Links ]
5. Carneiro IB, Sampaio HA, Carioca AA, Pinto FJ, Damasceno NR. Old and new anthropometric indices as insulin resistance predictors in adolescents. Arq Bras Endocrinol Metabol 2014;58(8):838-43. [ Links ]
6. Correia-Costa L, Santos AC, Severo M, Guerra A, Schaefer F, Caldas Afonso A, et al. Sex-specific mediating role of insulin resistance and inflammation in the effect of adiposity on blood pressure of prepubertal children. PLoS One 2015;10(6):e0132097. [ Links ]
7. Nisanci Kilinc F, Cagdas DN. Diet and physical activity interventions do have effects on body composition and metabolic syndrome parameters in overweight and obese adolescents and their mothers. Turk J Pediatr 2013;55(3):292-9. [ Links ]
8. Silva F, Ferreira E, Goncalves R, Cavaco A. Pediatric obesity: The reality of one consultation. Acta Med Port 2012;25(2):91-6. [ Links ]
9. Tang Q, Ruan H, Tao Y, Zheng X, Shen X, Cai W. Effects of a summer program for weight management in obese children and adolescents in Shanghai. Asia Pac J Clin Nutr;23(3):459-64. [ Links ]
10. Gobato AO, Vasques AC, Zambon MP, Barros Filho A de A, Hessel G. Metabolic syndrome and insulin resistance in obese adolescents. Rev Paul Pediatr 2014;32(1):55-62. [ Links ]
11. DeFronzo RA, Tripathy D. Skeletal muscle insulin resistance is the primary defect in type 2 diabetes. Diabetes Care 2009;32(Suppl2):S157-63. [ Links ]
12. Beghin L, Castera M, Manios Y, Gilbert CC, Kersting M, De Henauw S, et al. Quality assurance of ethical issues and regulatory aspects relating to good clinical practices in the HELENA Cross-Sectional Study. Int J Obes (Lond) 2008;32(Suppl5):S12-S18. [ Links ]
13. Moreno LA, González-Gross M, Kersting M, Molnar D, De Henauw S, Beghin L, et al. Assessing, understanding and modifying nutritional status, eating habits and physical activity in European adolescents: The HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Health Nutr 2008;11(3):288-9. [ Links ]
14. Currie CE, Elton RA, Todd J, Platt S. Indicators of socioeconomic status for adolescents: The WHO Health Behaviour in School-aged Children Survey. Health Educ Res 1997;12(3):385-97. [ Links ]
15. Jiménez-Pavón D, Ortega FP, Ruiz JR, Espana-Romero V, García-Artero E, Moliner-Urdiales D, et al. Socioeconomic status influences physical fitness in European adolescents independently of body fat and physical activity: The HELENA study. Nutr Hosp 2010;25(2):311-6. [ Links ]
16. Tanner JM, Whitehouse RH. Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child 1976;51(3):170-9. [ Links ]
17. Nagy E, Vicente-Rodríguez G, Manios Y, Beghin L, Iliescu C, Censi L, et al. Harmonization process and reliability assessment of anthropometric measurements in a multicenter study in adolescents. Int J Obes (Lond) 2008;32(Suppl5):S58-65. [ Links ]
18. Lohman TG, Roche AF, Martorell R. Anthropometric Standardization Reference Manual. Human Kinetics Books. Champaign, Illinois; 1988:183. [ Links ]
19. Slaughter MH, Lohman TG, Boileau RA, Horswill CA, Stillman RJ, Van Loan MD, et al. Skinfold equations for estimation of body fatness in children and youth. Hum Biol 1988;60(5):709-23. [ Links ]
20. Rodríguez G, Moreno LA, Blay MG, Blay VA, Fleta J, Sarria A, et al. Body fat measurement in adolescents: Comparison of skinfold thickness equations with dual-energy X-ray absorptiometry. Eur J Clin Nutr 2005;59(10):1158-66. [ Links ]
21. Vicente-Rodríguez G, Rey-López JP, Mesana MI, Poortvliet E, Ortega FB, Polito A, et al. Reliability and intermethod agreement for body fat assessment among two field and two laboratory methods in adolescents. Obesity (Silver Spring) 2012;20(1):221-8. [ Links ]
22. Wells JC, Williams JE, Chomtho S, Darch T, Grijalva-Eternod C, Kennedy K, et al. Body-composition reference data for simple and reference techniques and a 4-component model: A new UK reference child. Am J Clin Nutr 2012;96(6):1316-26. [ Links ]
23. González-Gross M, Breidenassel C, Gómez-Martínez S, Ferrari M, Beghin L, Spinneker A, et al. Sampling and processing of fresh blood samples within a European multicenter nutritional study: Evaluation of biomarker stability during transport and storage. Int J Obes (Lond) 2008;32(Suppl5):S66-75. [ Links ]
24. Matthews DR, Hosker JP, Rudenski AS, et al. (1985) Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia; 28:412-9. [ Links ]
25. Katz A, Nambi SS, Mather K, et al. (2000) Quantitative insulin sensitivity check index: A simple, accurate method for assessing insulin sensitivity in humans. J Clin Endocrinol Metab;85:2402-10. [ Links ]
26. Addo OY, Himes JH. Are field measures of adiposity sufficient to establish fatness-related linkages with metabolic outcomes in adolescents? Eur J Clin Nutr 2014;68(6):671-6. [ Links ]
27. Carneiro IB, Sampaio HA, Carioca AA, Pinto FJ, Damasceno NR. Old and new anthropometric indices as insulin resistance predictors in adolescents. Arq Bras Endocrinol Metabol 2014;58(8):838-43. [ Links ]
28. Wedin WK, Díaz-Giménez L, Convit AJ. Prediction of insulin resistance with anthropometric measures: Lessons from a large adolescent population. Diabetes Metab Syndr Obes 2012;5:219-25. [ Links ]
29. Lee S, Kim Y, White DA, Kuk JL, Arslanian S. Relationships between insulin sensitivity, skeletal muscle mass and muscle quality in obese adolescent boys. Eur J Clin Nutr 2012;66(12):1366-8. [ Links ]
30. Unni US, Ramakrishnan G, Raj T, Kishore RP, Thomas T, Vaz M, et al. Muscle mass and functional correlates of insulin sensitivity in lean young Indian men. Eur J Clin Nutr 2009 Oct;63(10):1206-12. [ Links ]
31. Oberbach A, Bossenz Y, Lehmann S, Niebauer J, Adams V, Paschke R, et al. Altered fiber distribution and fiber-specific glycolytic and oxidative enzyme activity in skeletal muscle of patients with type 2 diabetes. Diabetes Care 2006;29(4):895-900. [ Links ]
32. Morio B, Hocquette J-F, Montaurier C, Boirie Y, Bouteloup-Demange C, McCormack C, et al. Muscle fatty acid oxidative capacity is a determinant of whole body fat oxidation in elderly people. Am J Physiol 2001;280:E143-E149. [ Links ]
33. Sun SS, Chumlea WC, Heymsfield SB, Lukaski HC, Schoeller D, Friedl K, et al. Development of bioelectrical impedance analysis prediction equations for body composition with the use of a multicomponent model for use in epidemiologic surveys. Am J Clin Nutr 2003;77(2):331-40. [ Links ]
![]() Correspondence:
Correspondence:
David Jiménez-Pavón.
GALENO Research Group.
Department of Physical Education.
School of Education.
Universidad de Cádiz.
Puerto Real, Cádiz. Spain
e-mail: david.jimenez@uca.es
Received: 04/10/1015
Accepted: 21/10/2015
