










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 no.5 Madrid sep./oct. 2016
https://dx.doi.org/10.20960/nh.570
TRABAJO ORIGINAL / Obesidad y síndrome metabólico
Acantosis nigricans is associated with risk factors related to cardiovascular disease in Mexican children with obesity
La Acantosis nigricans se asocia con factores de riesgo para enfermedades cardiovasculares en niños mexicanos con obesidad
Hugo Martínez-Rojano1,2, María Luisa Pizano-Zárate3,4, Bernarda Sánchez-Jiménez3, Reyna Sámano3 and Armando López-Portillo5
1Escuela Superior de Medicina del Instituto Politécnico Nacional.
2Instituto de Diagnóstico y Referencia Epidemiológicos (InDRE) "Dr. Manuel Martínez Báez". Secretaría de Salud.
3Department of Nutrition and Bioprogrammation. Instituto Nacional de Perinatología. Secretaría de Salud.
4Familiar Medicine Unit No. 4. Instituto Mexicano del Seguro Social.
5Familiar Medicine Unit No. 193. Estado de México. Instituto Mexicano del Seguro Social. Mexico
The present study was financed by the researchers of the Instituto Mexicano del Seguro Social. The authors declare that they have no conflict of interest in regard to the methods or products employed in the present study.
ABSTRACT
Introduction: The prevalence of obesity in Mexican children has increased during the last decade, as has the risk of early onset metabolic disorders and cardiovascular disease.
Objective: To determine the association of Acantosis nigricans (AN) with dyslipidemia, high blood pressure, body mass index (BMI), and risk factors related to eating behavior in overweight and obese children.
Patients and methods: This transverse analytical study, conducted in two Mexico City primary schools, included 300 boys and girls. Information was gathered on hereditary and perinatal background. A physical examination provided data on the presence/absence of AN, blood pressure, weight and height. The BMI and Z-score were calculated. The serum concentration of glucose, cholesterol and triglycerides was quantified and the lipoprotein profile determined.
Results: The prevalence of AN was 41.7%. An association was found between AN and risk factors for cardiovascular disease, including BMI (rS 0.432; p < 0.0001), systolic and diastolic blood pressure above the 90th percentile (rS 0.231, p < 0.0001; rS 0.128, p = 0.026; respectively), hypertriglyceridemia (rS 0.156; p = 0.007), and low levels of cHDL (rS -0.160; p = 0.006). AN was also associated with risk eating behavior, including dieting to lose weight (p = 0.004), losing control over eating (p = 0.023), and body fat percentage above the 90th percentile (χ2= 35.1; p = 0.0001). No association was observed between AN and serum glucose concentration (rS -0.018; p = 0.759). Logistic regression analysis demonstrated an association of AN with a low concentration of cHDL (RM: 1.726; p = 0.041) and a high percentage of body fat (> 48%) (RM: 3.591; p = 0.001).
Conclusion: A high prevalence of AN was found in overweight and obese children. There was an association between AN and risk factors of cardiovascular disease, including Z-score, BMI, dyslipidemia, and high blood pressure.
Key words: Acantosis nigricans. Dyslipidemia. Body mass index. Overweight. Obesity, Mexico.
RESUMEN
Introducción: la mayor prevalencia de obesidad en la población infantil mexicana durante la última década incrementa el riesgo de presentar trastornos metabólicos y enfermedades cardiovasculares a edades cada vez más tempranas.
Objetivo: determinar la asociación entre Acantosis nigricans (AN) con dislipidemia, hipertensión arterial, índice de masa corporal (IMC) y conductas alimentarias de riesgo en niños con sobrepeso y obesidad.
Pacientes y métodos: estudio transversal analítico realizado en dos escuelas públicas de la zona metropolitana de la ciudad de México donde participaron 300 niños, de ambos sexos, obteniéndose información de los antecedentes heredofamiliares y perinatales. Con la exploración física se valoró la presencia o ausencia de AN y presión sanguínea. Se pesó y midió a los escolares, se calculó el IMC y se estimó su puntaje Z. Se cuantificó la concentración sérica de glucosa, colesterol, triglicéridos y perfil de lipoproteínas.
Resultados: la prevalencia de AN fue 41,7%, al determinar la asociación entre la AN y los factores de riesgo cardiovascular, se identificó una asociación con el IMC (rS 0.432; p < 0.0001), entre las cifras de presión arterial sistólica y diastólica por encima del percentil 90 (rS 0.231; p < 0.0001) y (rS 0.128; p = 0,026) respectivamente, la hipertrigliceridemia (rS 0.156; p = 0.007), las bajas concentraciones de colesterol de lipoproteínas de alta densidad (cHDL) (rS -0,160; p = 0,006), así como la existencia de los trastornos de la conducta alimenticia; haber realizado dietas p = 0.004, ha perdido el control de lo que come p = 0,023 y cuando el porcentaje de grasa corporal fue superior al percentil 90, χ2 = 35.1; p = 0.0001, no se observó asociación con la concentración sérica de glucosa (rS -0.018; p = 0,759). En el análisis de regresión logística se observó que la presencia de AN mostró una asociación con las menores concentraciones de cHDL (RM: 1.726; p = 0,041) y con el porcentaje de grasa corporal (> 48%) (RM: 3.591; p = 0,001).
Conclusión: se observó una alta prevalencia de AN en niños con sobrepeso u obesidad y su asociación con factores de riesgo cardiovascular: puntaje Z del IMC, dislipidemia y las cifras tensionales elevadas.
Palabras clave: Acantosis nigricans. Dislipidemia. Índice de masa corporal. Sobrepeso. Obesidad. México.
Introduction
Overweight and obesity are defined as an abnormal or excessive accumulation of fat that implies a health risk. This phenomenon affects children as well as adults and is associated with the premature onset of chronic uninfectious diseases. In fact, some diseases before found only in adults, such as diabetes mellitus type 2 (DM-2) and high blood pressure, in some cases now appear very early in life (1,2).
Childhood obesity is one of the gravest public health problems of the 21st century, having become an emerging global epidemic that implies immediate and long-term effects. It is estimated that the percentage of obese children and adolescents has increased almost 50% in the last 20-30 years. In 2010 it was calculated that there were approximately 42 million overweight children in the world, of which about 35 million lived in developing countries. The Organization for Economic Cooperation and Development (OECD) classified Mexico as having the first place worldwide in overweight children (3).
This relatively recent, substantial increase in overweight and obese children does not bode well for the future, as these children have an eight-fold greater risk of remaining overweight or obese as adults. Indeed, 50% of children who are obese at 6 years of age and 80% of obese adolescents remain obese in adulthood (4,5). These children and adolescents also have a greater probability of early onset metabolic disorders (e.g., dyslipidemia, insulin resistance, glucose intolerance and DM-2), some types of cancer, degenerative cardiovascular disease, dermatological/neurological/endocrine disorders, as well as alterations in the respiratory system, gastrointestinal tract and locomotor apparatus (6,7). All of these disorders involve, to a greater or lesser extent, a shorter life expectancy and a lower quality of life, and all are for the most part preventable (8). As can be seen, the importance of overweight and obesity go far beyond problems of self-image.
In Mexico the national prevalence of overweight and/or obese children in 2012 was estimated by the World Health Organization (WHO) to be 34.4% (19.8% for overweight and 11.8% for obesity), including 32% for Mexican girls (20.2% for overweight and 14.5% for obesity) and 36.9% for Mexican boys (19.5% for overweight and 17.4% for obesity) (9). This prevalence of obesity in Mexico is very similar to that of the United States and Chile. Furthermore, the rate of increase in childhood obesity in Mexico is greater than that seen in developed countries and other developing countries.
Generally, efforts to prevent and detect risk factors for chronic degenerative diseases, such as hypertension and DM-2, are aimed at adults. Therefore, risk factors tend to be identified once the damage is already done. However, the underlying problems exist in obese children and adolescents, giving rise to a deleterious, progressive and systemic effect that begins as subtle and undetectable changes in individuals with a normal and asymptomatic appearance (10). Hence, early detection of the presence and possibly the development of this series of disorders by non-invasive markers is of utmost importance to be able to intervene at an early stage in the population at risk and thus avoid greater complications later on (11).
In 2000, the American Diabetes Association established Acantosis nigricans (AN) as one criteria for identifying children at risk for DM-2. The increased incidence of AN runs parallel with that of obesity. Moreover, the diagnosis of AN is clinical, being formed by symmetrical, hyperpigmented, hypertrophic and varicose plaques that are in some cases papilloma. These skin areas appear velvety in texture and brownish-black in color, and are most commonly found on the underarm, back of the neck, flexing points of the upper and lower limbs, the naval, groin, breast folds, face, as well as peribuccal and perianal regions. The most common areas to find these skin blotches is on the back or side of the neck. AN is reportedly heavily influenced by genetic factors, being frequently found with Hispanic, Afro-American and Indian people, and infrequently encountered with Caucasians. This dermatological condition is associated with insulin resistance and metabolic disorders, and is known to be a good predictor of hyperinsulinemia, which can lead to DM-2 (12-14).
The prevalence of AN varies according to ethnic origin, with an incidence of 13% in blacks, 5% in Hispanics, and less than 1% in Caucasians. Gender and age are not risk factors. In adolescents with more than 200% of normal body weight, the prevalence of AN is 66% (15). This skin condition is now common in young people, especially in populations with a high prevalence of DM-2. Hence, this clinical condition may constitute a simple, economical and non-invasive technique for detecting hyperinsulinemia and the propensity for DM-2 and/or metabolic syndrome, especially in children. Its simplicity and low cost make it ideal for detection of these disorders in low income or marginalized communities, advantageous in relation to the traditional test for glucose tolerance or the determination of postprandial glucose or serum insulin (15,16).
Eating habits are formed for biological, psychological and cultural reasons, and when these habits alter normal metabolism they can represent a risk factor for obesity. It has been documented that poor eating habits that lead to overweight and obesity in adolescents are related to eating while doing other activities, such as watching TV, playing computer games, doing homework and working, as well as with prolonged fasts and an obsessive preoccupation with getting fat. Although poor eating habits probably begin in childhood, they are more evident in adolescence (19,20).
In spite of the aforementioned evidence, few studies have considered the role of body weight in the development of AN, or the latter as an independent marker of insulin resistance in school-age children (5-11 years old). The increased incidence of AN in the pediatric age parallels the rise in obesity, endocrine pathologies, genetic syndromes, DM-2, dyslipidemia, polycystic ovary syndrome, hypertension, and insulin resistance, the latter not necessarily associated with obesity (16). Consequently, the increase in prevalence of overweight and obesity in Mexican children during the last two decades could possibly be related to the risk of a higher rates of insulin resistance and metabolic syndrome at an ever younger age. On the other hand, it should be pointed out that overweight and obesity have social and emotional implications that are immediate, affecting the quality of life of the child or adolescent in question, independently of the effects on physical health.
The aim of the present study was to determine whether, in a group of Mexican school children that reside in Mexico City, AN is associated with the Z-score of the body mass index (BMI), dyslipidemia, waist circumference, blood pressure and/or risk factors related to eating behavior.
Material and methods
This is a transversal analytical study carried out from October of 2012 to June of 2013, with the participation of the Regional General Hospital (Hospital General Regional #196 of the Instituto Mexicano de Seguro Social), the National Institute of Perinatology (Instituto Nacional de Perinatología de la Secretaría de Salud) and the Superior School of Medicine (Escuela Superior de Medicina del Instituto Politécnico Nacional). After receiving permission from the school authorities, all students of the fourth, fifth and sixth grades on the morning shift of two primary schools were invited to participate in the study. Exclusion criteria included any chronic disease or any child under medication.
SUBJECTS
Based on a table of random numbers, statistical sampling was carried out in order to obtain a subset of the total population with characteristics similar to those found in each school grade. For this purpose, we used a list of students enrolled in the two schools involved in the present study, with a substitution technique in case a selected student did not want to participate. The sample had the following distribution: 79 (4th grade), 110 (5th grade) and 111 (6th grade), with 133 boys and 167 girls from 9-11 years old. Informed consent was obtained from the parents or tutor, with the informed approval of the participating child. The protocol was approved by the Ethics in Research Committee of the Instituto Mexicano del Seguro Social. A clinical history was recorded for each child, with emphasis on hereditary family background as well as prenatal and pathological information.
Medical personnel carried out a physical examination. A family doctor and a pediatrician evaluated the presence/absence of AN in five distinct anatomical regions: on the back of the neck, underarms, the internal flexing areas of the elbows and knees, and the naval. The children were then divided into those with and without AN (AN+ and AN-).
ANTHROPOMETRIC MEASUREMENTS
Evaluation of body weight (kg) was done with a portable digital scale (SECA, model 803, with precision of 100 g). Height measurements (m) were made to 0.1 cm accuracy with a stadiometer (SECA, model 0123). Anthropometric measurements included the circumference of the waist and hip (cm), made with a medical tape measure (SECA, model 200), according to the criteria proposed by the WHO (17). The BMI was calculated with the Quetelet formula (weight in kilograms divided by the height in meters squared). The Z-score for age was also calculated according to the WHO standard, classifying the school children as normal (≤ 1) overweight (> 1 and ≤ 2) or obese (> 2). Z-scores were considered valid between -5.0 and +5.0.
Body fat was determined by measuring body perimeters by using a tape measure with 1 mm accuracy (Sanny medical). Measurement of fat folds was performed with a Vernier caliper (Harpenden). These non-invasive measurements were taken in the schools, averaging 4-5 minutes for each child. The protocols for these measurements were in accordance with the requirements of the International Society for the Advancement of Kinanthropometry.
CLINICAL EVALUATION
Blood pressure was determined after at least 10 minutes of rest, using a sphygmomanometer, a cuff adequate for the children and their complexion, and a stethoscope (Riester). The method utilized was auscultatory, since the records obtained were evaluated with the tables of the National High Blood Pressure Education Program. The pressure hoses used covered 2/3 of the arm, from the olecranon to the shoulder, and the inflatable cuff covered 80% of the circumference of the arm. Measurements were made in the morning, with the child seated, leaning on the backrest of the chair, feet on the floor and the right arm extended. The systolic and diastolic blood pressure (SBP and DBP) were recorded, utilizing the Korotkoff phases I and V as a reference, respectively. The measurement was taken three times because generally the readings tend to stabilize by adaptation of the child to the method and the corresponding diminishment of his/her anxiety. The latter two readings were averaged for the final value. In case the blood pressure reading was elevated, the parents were informed and it was recommended that they visit their pediatrician or family doctor.
The tables of blood pressure of the National High Blood Pressure Education Program were used as the criterion of classification, adjusting the percentile according to height and gender. Consequently, children with blood pressure below the 90th percentile of the standard were considered to have normal blood pressure, while those from the 90th to 94th percentile were classified as pre-hypertensive and those from the 95th percentile and above as hypertensive (18).
BIOCHEMICAL PROFILE
After a fast of 12 hours, with previous asepsis, blood samples were taken by venipuncture with the system of a Vacutainer vacuum. The tubes with blood were centrifuged for 10 min at 3,500 rpm to obtain serum, which was stored in different aliquots at -70 oC to await processing. In these serum samples, the concentration of glucose (mg/dL), triglycerides (mg/dL) and cholesterol (mg/dL) was quantified with colorimetric enzymatic methods. cHDL (mg/dL) was evaluated by using a kit (HDL-Cholesterin/cholesterol, Roche Diagnostics).
EVALUATION OF RISK FACTORS RELATED TO EATING BEHAVIOR
Risk factors related to eating behavior were determined with the diagnostic criteria for eating disorders proposed by the Diagnostic Manual and Statistics of Mental Disorders IV. The resulting values were evaluated with the scale validated by Unikel et al. in a Mexican population. The results of using this scale have shown a reliability, according to Cronback's alpha, of 0.83 for women in Mexico City and 0.72 for women in the Mexico State (19).
This scale consists of 10 questions that evaluate the preoccupation with getting fat and other risk factors related to eating behavior in the three months prior to the survey. The answers were based on four Likert-type options (never or almost never = 0, sometimes = 1, frequently but less than two times per week = 2, very frequently or more than 2 times per week = 3 points). The degree of risk was scored as follows: less than 7 was considered to be without risk, 7-10 as moderate risk and > 10 high risk (19,20).
SOCIOECONOMIC LEVEL
This factor was determined by an interview with one of the parents or the tutor of each child, according to the standards of the Mexican Association of Market Research and Public Opinion (21). The interview consisted of 10 questions to establish scoring and overall classification in one of 6 levels of the standard of living: A/B = the highest, C+ = slightly above average, C = average, D+ = slightly below average, D = low or austere, and E = the lowest.
STATICAL ANALYSIS
A descriptive analysis was performed, utilizing absolute and relative (percentages) frequencies as well as the mean and standard deviation of quantitative variables to determine statistical difference and to test the hypothesis. The Shapiro Wild test was used to determine normal distribution of the sample. The Spearman's rank correlation for independent samples was employed to compare the groups. To evaluate the possible association between variables, the χ2 non-parametric test of independence was applied. For non-parametric correlations, multiple logistical regression analysis was used. For analysis of multiple regression, all variables of confusion or modifiers of effect were included. Statistical significance was considered with p < 0.05. The information was recorded in the Microsoft EXCEL program and analysis was carried out in the SPSS version 15 for the Windows statistical program.
ETHICAL ASPECTS
Data gathering and analysis was confidential, taking into account ethical questions related to autonomy, information and security. The findings of the present study were included in a pamphlet given to all participants. The aim of this pamphlet was to provide guidelines for good eating habits in order to help the parents to establish good nutrition for their children. The present study was carried out following the guidelines established by the Official Mexican Norm (NOM-043-SSA2-2005) of the Secretary of Health in Mexico (22).
Results
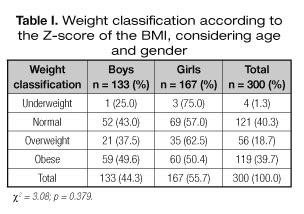
Of the 300 school children that participated in the study, 55.7% (167) were girls and 44.3% (133) were boys. Regarding socioeconomic level, 18 (6%) corresponded to a low or austere standard of living, 160 (53.3%) to an average level and 122 (40.7%) to a level slightly above average. Weight classification of the children was determined with the Z-score of the BMI according to age and gender, as proposed by the WHO, finding a 39.7% prevalence of obesity (119), 18.7% (56) overweight, 40.3% (121) normal and 1.3% (4) underweight. Overweight and obesity was more common among the girls (Table I).
The perinatal background of the children, according to information gathered from the mothers, indicated that at the time of birth the average number of weeks of gestation (WOG) was 38.4 ± 2.3%, with a weight of 3.183 ± 516 g, and a height of 49 ± 4.3 cm. Exclusive breastfeeding lasted an average of 8.5 ± 6.6 months, and for 20.7% (62) it lasted less than 3 months.
The average age of the mothers at the moment of the study was 35.7 ± 5.6 years, while that of the fathers was 35.7 ± 11.4 years, with 62.7% (188/300) of the mothers and 67.5% of the fathers having finished middle school. It was observed that 64.3% (193/300) of the mothers were overweight or obese and 71.2% (200/300) of the fathers, and that 36.7% (110/300) of both parents worked. Regarding the immediate family, there was a background for 53.3% (160/300) of the children of obesity, for 59.3% (178/300) of DM-2, and for 67.3% (202/300) of systemic high blood pressure.
The average values of parameters for the children was the following: age, 10.1 ± 0.7 years; weight, 42.8 ± 10.9 kg; height, 143 ± 8 cm; BMI, 20.5 ± 3.8 kg/m2; waist circumference, 68.8 ± 10.6 cm; hip circumference, 81.1 ± 8.9 cm; serum glucose, 98.5 ± 11.8 mg/dL; and serum cholesterol, 176.4 ± 48 mg/dL. There was glucose intolerance in 6 children and DM-2 in no children.
Regarding gender, there were no significant differences in any of the anthropometric, clinical or biochemical variables. Therefore, all of the children were included in the analysis of the association between variables, without carrying out stratification by gender.
AN was found in 41.7% (125) of the children, of which 37.6% (47/125) were overweight and 54.4% (68/125) obese. With a greater BMI there was a greater frequency of AN, while in the children with normal weight for their height, no AN was found. The children with AN not only had a tendency to higher weight but also lower height compared to the children without AN (see Table II).
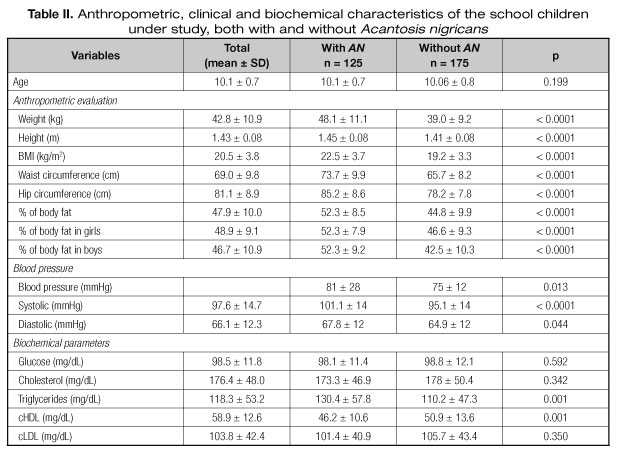
Blood pressure was above the 90th percentile in 10.8% of the children. This high level of blood pressure was found in 6.5% of the children with normal BMI, 9% of those overweight, and 21% of those with obesity.
Serum cholesterol concentration was similar in the children with and without AN, while triglyceride concentration was much higher and cHDL concentration lower in the children with AN (Table II).
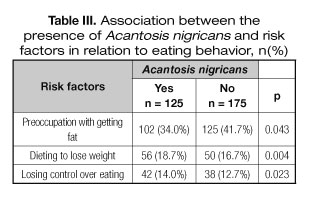
There was an association between AN and the following 2 = 4.09; p = 0.043), dieting to lose weight (χ2= 8.2; p = 0.004), losing control over eating (χ2= 5.13; p=0.023), and a percentage of body fat above the 90th percentile (χ2= 35.1; p = 0.0001) (Table III). No association was observed between AN and the length of breastfeeding, the weight of the parents, if both parents were working, if the parents did regular exercise, or a family background of DM-2, hypertension or obesity.
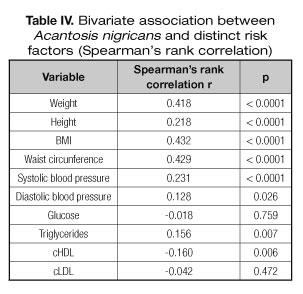
There was an association between AN and the BMI (rS 0.432; p < 0.0001), systolic blood pressure (rS 0.231; p < 0.0001), diastolic blood pressure (rS 0.128; p = 0.026), hypertriglyceridemia (rS 0.156; p = 0.007), and level of cHDL (rS -0.160; p = 0.006). No association was found between AN and the concentration of serum glucose (rS -0.018; p = 0.759) or low-density lipoprotein cholesterol (cLDL) (rS -0.042; p = 0.472) (Table IV).
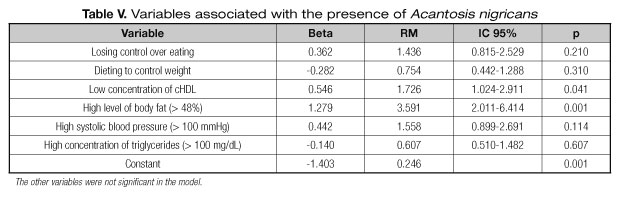
The risk of having AN increased with a lower concentration of cHDL (RM: 1.726; p = 0.041) and a greater percentage of body fat (RM: 3.591; p = 0.001), according to calculations based on logistical regression (Table V).
Discussion
Obesity is a public health problem that has currently become a worldwide epidemic. AN is now frequently found in children and adolescents, especially in populations with a high prevalence of obesity, insulin resistance and DM-2. Therefore, the present study explored the possible association of AN with the latter medical conditions, as well as the possibility of using AN as a marker so that family doctors and general practitioners can identify obesity in school children in a timely manner. This would allow for preventative measures to be implemented against the development of cardiovascular disease and DM-2 in overweight and obese children (23,24).
The incidence of AN in children has increased together with that of obesity and insulin resistance. For this reason, the American Diabetes Association has recommended the early detection of AN as a criterion for identifying children at risk for developing DM-2. The prevalence of AN in the present study was 41.7%, greater than that reported by Stoddart et al., who found 34.2% AN in a Cherokee Indian population (25). Meanwhile, Mukhtar et al. documented an 18.9% prevalence of AN in obese adolescents in New Mexico (26), Nguyen et al. reported 25% of AN in overweight Afro-American children (27), and Stuart et al. found 38% of AN in Native Americans (28). On the other hand, Thivel D and Maisonneuve B have reported the prevalence of AN to be as high as 68 and 69.9%, respectively, in obese children (29,30). These differences in prevalence of AN have been related to the proportion of overweight and obesity in the groups under study.
With the presence of AN associated with obesity, there are important alterations in the metabolism of lipids. A group of children with AN in a previous study showed signs of greater risk for the development of atherosclerosis and cardiovascular disease (31). When comparing the children with and without AN in the present study, there was a lower serum concentration of cHDL (c-HDL 46 ± 10 vs. 50 ± 13 p = 0.001) and a higher serum concentration of triglycerides (129 ± 58 vs. 110 ± 47 p = 0.002). Numerous studies have demonstrated the association between the risk of developing cardiovascular disease and low serum concentrations of cHDL (32) as well as hypertriglyceridemia. The latter condition gives rise to changes in the composition of cLDL, favoring the appearance of phenotype B that is characterized by the presence of small cLDL, which is more susceptible to oxidation and therefore can lead to atherosclerosis (33,34).
One of the most relevant findings of the present study is the early age (10.1 ± 0.7 years) at which a group of children with obesity and AN were found to have hypertriglyceridemia as well as a reduced concentration of serum cHDL and a high concentration of cLDL, which probably will favor the development of cardiovascular disease at a very early age. This observation is in agreement with Fishbein in the United States (35). Additionally, the alterations found in the profile of lipoproteins is also in accordance with Skhonthachit P et al. in Thai children (36) and with Boyd GS et al. (37), who both found a high prevalence of dyslipidemia in overweight and obese children and adolescents.
The existence of dyslipidemia is often reported in the many studies that have provided evidence of the association between obesity and the risk of cardiovascular disease. Within this context, the greatest prevalence found has been hypertriglyceridemia. Almost 1 of 2 children in the present study presented concentrations of triglycerides in the range considered as high risk, while 1 of 3 children showed hypercholesterolemia and 1 of 4 mixed dyslipidemia. This fact should be alarming to the authorities in the area of public health due to the combination of obesity and an alteration in the profile of lipids in a significant percentage of children, leading to a high risk of cardiovascular and metabolic diseases at an early age (38). For this reason, children with obesity should be a target group for the implementation of measures aimed at diminishing the aforementioned metabolic alterations. Such measures should include the modification of eating habits and lifestyle (including more exercise) in order to attain a loss of weight. Additionally, there should be constant monitoring of the lipid profile in obese children and adolescents, especially if they have AN, as recommended by the American Heart Association (39).
On the other hand, there is a widely recognized relation between systemic high blood pressure and obesity caused by poor diet and lack of exercise. A greater percentage of obesity has been found among a population of hypertensive children and adolescents in Cuba. Furthermore, with a reduction in weight, blood pressure was normalized in this population. Nevertheless, there are few studies that take into account the relation between the degree of obesity, time of evolution, the age of appearance, and the distribution of body fat in obese and hypertensive children and adolescents.
Different studies have shown the relation of obesity in children/adolescents with systemic high blood pressure, especially in those with a greater degree of obesity and lipid anomalies. The present study demonstrates higher blood pressure in children with obesity and AN than in children with normal weight. The greatest difference was found in systolic blood pressure, in accordance with the study by Dong B et al. on children and adolescents in China (40), by Chiolero A. on children of the Republic of Seychelles in Africa (41), by Moser on Brazilian children (42), and by Hoog who studied the association between blood pressure and BMI in children from different ethnic groups (43).
In the present study, 10.8% of the children had systolic or diastolic blood pressure above the 90th percentile, a figure slightly less than that reported by Bojórquez Díaz et al. (44), who detected high blood pressure in 12.7% of primary school children in the State of Sonora, Mexico. However, the figure from the present study is higher than the 7.6% reported by Salvadori et al. (45) in a study on rural children in Canada and the 4.2% of children from 5 to 12 years old and 6% of adolescents from 13 to 18 years old found by Díaz (46) in a study in Argentina. Additionally, in Cuba Suárez Cobas et al. (47) reported a group of adolescents with high blood pressure above the 90th percentile, made up of 7.6% boys and 2.4% girls from 15 to 17 years old, while in the city of Merida, Venezuela, there were 6.3% of adolescents from 15 to 17 years old (48) with this condition, and in Spain 1.7% of boys and the 3.05% of girls (49). Hence, the prevalence of obesity in the present study and a previous study in Mexico is higher than that found in children of Canada, Argentina, Venezuela and Spain. Due to the foreboding presence of high blood pressure at such an early age in Mexico, especially when found in overweight and obese children, an early detection of obesity and high blood pressure is of great importance since these conditions increase the risk of health problems in adolescence and early adulthood (50).
On the other hand, the present study confirmed the positive and significant association of AN with obesity (percent of body fat) and dyslipidemia (low cHDL), based on the statistical analysis with the Spearman's rank correlation and multiple logistical regression (RM: 3.591; p = 0.001, RM: 1.726; p = 0.041; respectively). This suggests that AN reflects the increase in obesity in Mexico, which is a risk factor for cardiovascular disease and is associated with dyslipidemia, high blood pressure and a greater risk of developing DM-2 (38,39).
Regarding risk factors in relation to eating behavior, the present study evidences the greater prevalence of AN among those that worry about getting fat, that had dieted to lose weight, and were not able to control what they eat, confirming a study on a group of adolescents (20). However, it should be stated that poor eating habits are often accompanied by an inadequate weight, including overweight and obesity, and that this is in turn associated with the alteration of hormones like insulin that are known to provoke the development of AN (11). The only variables associated with AN in the present study were low cHDL and a high percentage of body fat.
In summary, the results of the present study highlight the high prevalence of AN in overweight and obese children, and its association with two risk factors for cardiovascular disease, the distribution of body fat and dyslipidemia. This suggests that it is necessary to take early preventative measures, such as carrying out a follow-up in relation to the high risk that these children will later develop DM-2, other metabolic disorders, and/or cardiovascular disease. Such measures would represent an improvement in the medical attention and quality of life for Mexican children.
One of the limitations of the present study is that the data do not come from a representative sample of all children of primary schools of Mexico. Nonetheless, the sample is made up of a homogeneous population in a certain age group. Another limitation of this study was the fact that the serum concentration of insulin was not determined, and that information was not gathered in regard to the physical activity of the children.
These limitations could in part be overcome by carrying out a -follow-up prospective cohort study of this population to see if they indeed develop DM-2, atherosclerosis, and/or polycystic ovary syndrome. In spite of the limitations of the present study, one of the main contributions is the association found of AN with obesity, certain risk factors for cardiovascular disease, and metabolic disorders in children, who are one of the most vulnerable groups of the world population.
Conclusion
Acantosis nigricans is easy to evaluate in a clinical setting. The present study found a high prevalence (41.7%) of AN in overweight and obese children. Certain variables were associated with the presence of AN, including a low concentration of cHDL, a high percentage of body fat, and high blood pressure, but not eating behavior disorders.
Acknowledgements
We are grateful to all the parents and children who participated in the present study. We also give thanks to the teachers and principals for facilitating access to and use of the school setting in order to carry out the study.
References
1. Pulgaron ER and Delamater AM. Obesity and type 2 diabetes in children: epidemiology and treatment. Curr Diab Rep 2014;14(8):508. DOI:10.1007/s11892-014-0508-y. [ Links ]
2. Morandi A, Maffeis C. Predictors of metabolic risk in childhood obesity. Horm Res Paediatr 2014;82:3-11. [ Links ]
3. Organization for Economic Co-operation and Development. Key facts-Mexico. Update 2014. http://www-oecd.org/mexico/Obesity-Update-2014-MEXICO_EN.pdf. [ Links ]
4. Deshmukh-Taskar P, Nicklas TA, Morales M, Yang S-J, Zakeri I, Berenson GS. Tracking of overweight status from childhood to young adulthood: the Bogalusa Heart Study. Eur J Clin Nutr 2006;60:48-57. [ Links ]
5. Magarey AM, Daniels LA, Boulton TJ, Cockington RA. Predicting obesity in early adulthood from childhood and parental obesity. Int J Obes 2003;27:505-13. [ Links ]
6. Morandi A, Maffeis C. Predictors of metabolic risk in childhood obesity. Horm Res Paediatr 2014;82:3-11. [ Links ]
7. Reinerhr T. Type 2 diabetes mellitus in children and adolescents. World J Diabetes 2013;4(6):270-81. [ Links ]
8. World Health Organization. Prioritizing areas for action in the field of population-based prevention of childhood obesity. WHO. February 2012. [ Links ]
9. Secretaría de Salud. Encuesta Nacional de Salud y Nutrición 2012. Resultados Nacionales. Cuernavaca, México: Instituto Nacional de Salud Publica, México; 2012. [ Links ]
10. Williams CL, Hayman LL, Daniels SR, Robinson TN, Steinberger J, Paridon S, et al. Cardiovascular Health in Childhood. A statement for health professionals from the committee on atherosclerosis, hypertension, and obesity young (AHOY) of the council on cardiovascular disease in the young, American Heart Association. Circulation 2002;106:143-60. [ Links ]
11. Ng HY, Young JHM, Huen KF, Chan LTW. Acanthosis nigricans in obese Chinese children. Hong Kong Med J 2014;20:290-6. [ Links ]
12. American Diabetes Association. Type 2 diabetes in children and adolescents. Diabetes Care 2000;23(3):381-9. [ Links ]
13. Brown B, Noonan C, Bentley B, Conway K, Corcoran M, FourStar K, et al. Acanthosis nigricans among northern plains American Indian children. J Sch Nurs 2010;26(6):450-60. [ Links ]
14. Kobaissi HA, Weigensberg MJ, Ball GD, Cruz ML, Shaibi GQ, Goran MI. Relation between Acanthosis nigricans and insulin sensitivity in overweight Hispanic children at risk for type 2 diabetes. Diabetes Care 2004;27:1412-6. [ Links ]
15. Urrutia-Rojas X, McConathy W, Willis B, Menchaca J, Luna-Hollen M, Marshall K, et al. Abnormal glucose metabolism in Hispanic parents of children with acanthosis nigricans. ISRN Endocrinology 2011. DOI:10.5402/2011/481371. [ Links ]
16. Dassanayake A, Kasturirate A, Niriella MA, Kalubovila U, Rajindrajith de Silva AP, Kato N, et al. Prevalence of Acanthosis nigricans in an urban population in Sri Lanka and its utility to detect metabolic syndrome. BMC Research Notes 2011;4:25. [ Links ]
17. World Health Organization. Technical report series 854. Physical status: the use and interpretation of anthropometry. Geneva;1995. [ Links ]
18. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004;114:555-76. [ Links ]
19. Unikel-Santocini C, Nuño-Gutiérrez B, Celis-de la Rosa A, Saucedo-Molina TJ, Trujillo-Chi Vacua EM. Garcia-Castro F, et al. Conductas alimentarias de riesgo: prevalencia en estudiantes mexicanas de 15 a 19 años. Rev Invest Clin 2010;62(5):424-32. [ Links ]
20. Sámano R, Zelonka R, Martínez-Rojano H, Sánchez-Jiménez B, Ramírez C, Ovando G. Asociación del índice de masa corporal y conductas de riesgo en el desarrollo de trastornos de la conducta alimentaria en adolescentes mexicanos. Arch Latinoam Nutr 2012;62(2):145-54. [ Links ]
21. Índice de Nivel Socioeconómico de la Asociación Mexicana de Agencias de Investigación de Mercados y Opinión Pública (AMAI) septiembre 2014. Regla AMAI NSE 8X7. www.amai.org/NSE/NivelSocioeconomicoAMAI.pdf. [ Links ]
22. Norma Oficial Mexicana NOM-043-SSA2-2012. Servicios básicos de salud. Promoción y educación para la salud en materia alimentaria. Criterios para brindar orientación. Diario Oficial de la Federación; 2013. [ Links ]
23. Brickman WJ, Huang J, Silverman BL, Metzger BE. Acanthosis nigricans identifies youth at high risk for metabolic abnormalities. J Pediatr 2010;156:87-92. [ Links ]
24. Rafalson L, Pham TH, Willi SM, Marcus M, Jessup A, Baranowski T. The association between acanthosis nigricans and dysglycemia in an ethnically diverse group of eighth grade students. Obesity (Silver Spring); 2013;21(3):E328-33. [ Links ]
25. Stoddart M, Blevins K, Lee E, Wang W, Blackett P. Association of Acanthosis Nigricans with hyperinsulinemia compared with other selected risk factors for type 2 diabetes in Cherokee Indians. Diabetes Care 2002; 25:1009-14. [ Links ]
26. Mukhtar Q, Cleverley G, Voorhees R, Mc Grath J. Prevalence of acanthosis nigricans and its association with hyperinsulinemia in New Mexico adolescents. J Adolesc Health 2001;28:372-6. [ Links ]
27. Nguyen TT, Keil MF, Russell DL, Pathomvanich A, Uwaifo GI, Sebring NG, et al. Relation of acanthosis nigricans to hyperinsulinemia and insulin sensitivity in overweight African American and white children. J Pediatr 2001;138:474-80. [ Links ]
28. Stuart CA, Smith MM, Gilkison CR. Acanthosis nigricans among Native Americans: an indicator of high diabetes risk. Am J Public Health 1994;84:1839-42. [ Links ]
29. Thivel D, Malina RM, Isacco L, Aucouturier J, Meyer M, Duché P. Metabolic syndrome in obese children and adolescents: dichotomous or continuous? Metab Syndr Relat Disord 2009;7:549-55. [ Links ]
30. Maisonneuve B, Auclair C, Ali M, Terral D, Deméocq F, Roszyk L, et al. Metabolic abnormalities in obese French children. Arch Pediatr 2009;16:991-8. [ Links ]
31. Zhu WF, Liang L, Wang CL, Fu JF. Triglyceride and non-high-density lipoprotein cholesterol as predictors of cardiovascular disease risk factors in Chinese Han children. Indian Pediatr 2013;50:394-8. [ Links ]
32. Ayer JG, Sholler GF. Cardiovascular risk factors in Australian children: hypertension and lipid abnormalities. Aust Prescr 2012;35:51-5. [ Links ]
33. McGill HC, McMahan A, Zieske AW, Tracy RE, Malcom GT, Herderick EE, Strong JP. Association of coronary heart disease risk factors with microscopic qualities of coronary atherosclerosis in youth. Circulation 2000;102:374-9. [ Links ]
34. Harchaoui KEL, Visser ME, Kastelein JJP, Stroes ES and Dallinga-Thie GM. Triglycerides and cardiovascular risk. Curr Cardiol Rev 2009;5:216-22. [ Links ]
35. Fishbein MH, Mogren C, Gleason T, Stevens WR. Relationship of hepatic steatosis to adipose tissue distribution in pediatric nonalcoholic fatty liver disease. J Pediatr Gastroenterol Nutr 2006;42(1):83-8. [ Links ]
36. Sukhonthachit P, Aekplakorn W, Hudthagosol C, Sirikulchayanonta C. The association between obesity and blood pressure in Thai public school children. BMC Public Health 2014;14:729. DOI: 10.1186/1471-2458-14-729. [ Links ]
37. Boyd GS, Koeniqsberg J, Falkner B, Gidding S, Hassingk S. Effect of obesity and high blood pressure on plasma lipid levels in children and adolescents. Pediatrics 2005;116(2):442-6. [ Links ]
38. Srinivasan SR, Frontini MG, Xu J, Berenson GS. Utility of childhood non-high-density lipoprotein cholesterol levels in predicting adult dyslipidemia and other cardiovascular risks: The Bogalusa Heart Study. Pediatrics 2006;118(1):201-6. [ Links ]
39. Williams CL, Hayman LL, Daniels SR, Robinson TN, Steinberger J, Paridon S, et al. Cardiovascular Health in Childhood. A statement for health professionals from the committee on atherosclerosis, hypertension, and obesity young (AHOY) of the council on cardiovascular disease in the young, American Heart Association. Circulation 2002;106:143-60. [ Links ]
40. Dong B, Wang Z, Wang H-J, Ma J. Associations between adiposity indicators and elevated blood pressure among Chinese children and adolescents. J Hum Hypertens 2015;29:236-40. [ Links ]
41. Chiolero A, Madeleine G, Gabriel A, Burnier M, Paccaud F, Bovet P. Prevalence of elevated blood pressure and association with overweight in children of a rapidly developing country. J Hum Hypertens 2007;21:120-7. [ Links ]
42. Moser DC, Guiliano IC, Titski AC, Gaya AR, Coelho-e-Silva MJ, Leite N. Anthropometric measures and blood pressure in school children. J Pediatr (Rio J) 2013;89:243-9. [ Links ]
43. Hoog MLA, van Eijsden M, Stronks K, Gemke RJBJ, Vrijkotte TGM. Association between body size and blood pressure in children from different ethnic origins. Cardiovascular Diabetology 2012;11:136. DOI: 10.1186/1475-2840-11-36. [ Links ]
44. Bojórquez DCI, Angulo PCM, Reynoso EL. Factores de riesgo de hipertensión arterial en niños de primaria. Psicología y Salud 2011;21:245-52. [ Links ]
45. Salvadori M, Sontrop JM, Garg AX, Truong J, Suri RS, Mahmud FH, et al. Elevated blood pressure in relation to overweight and obesity among children in a rural Canadian community. Pediatrics 2008;122(4):e821-e827. [ Links ]
46. Díaz A, Tringler M, Molina JD, Díaz MC, Geronim V, Aguera D, et al. Control de la presión arterial y prevalencia de hipertensión arterial en niños y adolescentes de una población rural de Argentina. Datos preliminares del Proyecto Vela. Arch Argent Pediatr 2010;108(1):68-74. [ Links ]
47. Suárez CL, Rodríguez CA, Tamayo VJL, Rodríguez BRP. Prevalencia de hipertensión arterial en adolescentes de 15 a 17 años. MEDISAN 2009;13(6). http://bvs.sld.cu/revistas/san/vol13_6_09/san07609.htm. [ Links ]
48. Blanco LC, Macías TC, López BM. Relación entre la maduración temprana, índice de masa corporal y el comportamiento longitudinal de la presión arterial sistólica. Acta Cient Venez 2000;51:252-6. [ Links ]
49. Marrodán SMD, Cabañas AMD, Carmenate MMM, González-Montero EM, López-Ejeda N, Martínez AJR, et al. Asociación entre adiposidad corporal y presión arterial entre los 6 y los 16 años. Análisis en una población escolar madrileña. Rev Esp Cardiol 2013;66(2):110-5. [ Links ]
50. Flynn JT, Falkner BE. Obesity hypertension in adolescents: epidemiology, evaluation, and management. J Clin Hypertens (Greenwich) 2011;13:323-31. [ Links ]
![]() Correspondence:
Correspondence:
Hugo Martínez-Rojano.
Departamento de posgrado.
Escuela Superior de Medicina del Instituto Politécnico Nacional.
Avenida Salvador Díaz Mirón s/n, esq.
Plan de San Luís, Colonia Casco de Santo Tomás.
Delegación Miguel Hidalgo. 11340, Ciudad de México. México
e-mail: hmartinez_59@yahoo.com.mx, hugomartinezr@salud.gob.mx
Received: 14/01/2016
Accepted: 21/03/2016
