










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 no.5 Madrid sep./oct. 2016
https://dx.doi.org/10.20960/nh.588
Eating attitudes, body image and risk for eating disorders in a group of Spanish dancers
Actitudes alimentarias, imagen corporal y riesgo de trastornos alimentarios en un grupo de bailarines españoles
Ignacio Jáuregui-Lobera1,2, Patricia Bolaños-Ríos2, Eva Valero-Blanco1 and Ángeles Ortega-de-la-Torre1,3
1Area of Nutrition and Food Sciences. Department of Molecular Biology and Biochemical Engineering. Universidad Pablo de Olavide. Sevilla, Spain.
2Behavioural Sciences Institute. Sevilla, Spain.
3CIBERDEM, Spanish Biomedical Research Centre in Diabetes and Associated Metabolic Disorders. Madrid, Spain
ABSTRACT
Introduction: Prevalence of eating disorders (ED) and discrepancies between actual weight and weight perception seem much higher in dancers. The aims analysed in 77 dancers were: risk for ED; relationship between eating attitudes and psychological variables; dieting and self-weighing, and body image distortion.
Method: Weight- and body image-related variables, dieting, self-reported physical fitness, specific ED-related variables and other psychological variables were assessed. The robust Huber's model was applied in order to test the influence of the variables analysed on the Eating Attitudes Test (EAT-40) scores. In case of categorical variables, the Chi-square (χ2-test) or the Fisher's exact test were applied.
Results: Higher risk of ED was not obtained. Despite the relationship between EAT-40 and BMI, body appreciation and drive for thinness, scores on EAT-40 and BMI do not suggest higher risk in dancers. Dancers had a similar weight perception than other populations and body dissatisfaction seems not to be worse than the reported in other types of participants.
Conclusions: Despite some limitations, our study adds some data in this field of study bearing in mind the use of a cluster of variables previously not taken into account as a whole.
Key words: Dancers. Eating disorders. Weight misperception. Self-weighing. Body dissatisfaction. Body image distortion. Body appreciation.
RESUMEN
Introducción: la prevalencia de trastornos de la conducta alimentaria (TCA) y las diferencias entre el peso corporal real y el percibido parecen más elevadas en bailarines. Los objetivos analizados en 77 bailarines fueron: riesgo de TCA; relación entre actitudes alimentarias y variables psicológicas; conducta de dieta y autocontrol de peso, y distorsión de la imagen corporal.
Método: se estudiaron variables relacionadas con el peso y la imagen corporal, conducta de dieta, percepción de la propia forma física, variables específicas relacionadas con los TCA y otras variables psicológicas. El modelo estadístico robusto de Huber fue utilizado para probar la influencia de las variables analizadas en las puntuaciones del Eating Attitudes Test (EAT-40). Para las variables categóricas se usaron la prueba de Chi-cuadrado o el test de Fisher.
Resultados: no se encontró un mayor riesgo de TCA. Aun existiendo correlación entre el EAT-40 y el índice de masa corporal (IMC), aprecio corporal e impulso a adelgazar, las puntuaciones del EAT-40 y el IMC no sugieren un mayor riesgo en este grupo de bailarines. Por otro lado, estos bailarines tienen una percepción del propio peso similar a la de otras poblaciones y su insatisfacción corporal no parece ser peor que la expresada en otros tipos de población.
Conclusiones: a pesar de algunas limitaciones, este estudio añade algunos datos en este campo, teniendo en cuenta el grupo de variables analizadas, previamente no consideradas en conjunto.
Palabras clave: Bailarines. Trastornos de la conducta alimentaria. Percepción errónea del peso. Autocontrol de peso. Insatisfacción corporal. Distorsión de la imagen corporal. Aprecio corporal.
Introduction
The prevalence of eating disorders (ED) seems to be much higher for specific groups such as models, athletes and dancers (1-4). The reasons for these higher rates have been focused (among other elements) on personality factors, specifically some traits such as perfectionism, low self-esteem and high self-standards (2,5-7). Sociocultural influences encourage the development of both body image disorders and ED through two mechanisms: reinforcement -for example comments, which support the maintenance of an ideal of thinness- and modelling -imitation of observed behaviours- (8). The existence of specific personality traits along with sociocultural influences may explain, to some extent, the high prevalence of ED among high-risk occupations (9). Some authors have mentioned that perfectionism and low self-esteem, usually found among dancers, might explain why ED appear to be more prevalent among this group of people (9,10). Nevertheless, this statement remains controversial taking into account the disparity of results, probably due to methodological differences among studies (7). With respect to dancers there are different studies comparing all dancers vs. non-dancers as well as comparing ballet dancers vs. non-dancers. The overall prevalence of ED in all dancers was found to be 12%, which was slightly lower than the prevalence found in ballet dancers -16.4%- (7). These studies were mainly based on instruments such as the Eating Attitudes Test (both versions 26 and 40 items), the Eating Disorders Inventory (EDI), the Bulimia Investigation Test Edinburgh (BITE) and several clinical interviews (11-14). When studies have focused on all dancers vs. non-dancers it must be noted that the population of dancers is usually too diverse (ballet, modern dance, jazz, national dance, etc.) to reach clear conclusions. It is generally admitted that general dancers have more than twice the risk of developing an eating disorder and more than three times of developing anorexia nervosa (AN) and eating disorders not otherwise specified (EDNOS) than non-dancers (7).
With respect to body image and weight self-perception, it has been reported that many more dancers and models than control girls, show discrepancies between their actual weight and their weight perception, assessing their weight as normal or above average while actually being underweight (9). This has been explained by the nature of these activities, which imply that less body weight means success. In addition, their professional and cultural surrounding creates an aversion towards gaining weight, and strongly supports the attitude that a skinny body and body image are normal (9).
Generally, body appreciation and body image quality of life seem to be negatively related to body dissatisfaction and drive for thinness, and positively related to self-esteem. In the case of body image quality of life, the relationship with drive for thinness/body dissatisfaction seems to be only clearly significant in women (15,16). On the other hand, body mass index (BMI) is positively correlated to disordered eating attitudes and body dissatisfaction (17,18). In previous studies it has been reported that self-esteem and BMI are related to positive body image (19). In order to detect the risk for ED the Eating Attitudes Test (EAT) has been the most used psychometric instrument. When using the version of 40 items the cut-off point is usually established at 30. With this cut-off point the percentages of people at risk in Spain range between 0.6-8.3 and 7.3-17.3 for males and females, respectively. Recently, some authors have concluded that a cut-off point of 21 yields the best diagnostic prediction with a sensibility and specificity of 88.2% and 62.1% respectively, and positive and negative prediction values of 17.7% and 62.1% respectively (20).
According to the reviewed literature: a) it is expected a positive relationship between dance and higher prevalence of risk for ED; b) it is expected a relationship between eating attitudes and psychological variables such as self-esteem, mental health, specific EDI subscales, body appreciation and body image quality of life; c) considering the dancers group, it is expected a higher prevalence of going on diet and/or more self-weighing frequency and more discrepancies between actual weight and weight perception, assessing weight as normal or above average while actually being underweight; and d) dancers have an increased body image distortion.
Method
SAMPLE
The sample comprised 77 dancers from the Centro Andaluz de Danza (CAD; Junta de Andalucía, Seville, Spain) with a mean age of 21.22 (SD = 3.06) and an age range between 18 and 32. 20 were males and 57 were females. The mean BMI was 21.01 (SD = 1.85). All of them voluntarily agreed to participate in the study. The CAD is not a "professional Centre of dance" so the attendants practice dance as a semi-professional activity.
MEASURE AND INSTRUMENTS
According with the main instruments (questionnaires, inventories, scales) used in previous research on this field of study, the following were applied.
Weight- and body image-related factors
Anthropometric measurements: BMI was calculated as the relationship between weight (in kg) and height squared (in m). Weight and height were taken in individual sessions, with the participants in standing position, barefoot, and in light garments. An estadiometer "Añó-Sayol Atlántida S13" model (Barcelona, Spain) was used.
Weight perception: Considering weight perception, participants responded to this question: What do you think of yourself in terms of weight? Possible responses were: "very overweight", "slightly overweight", "about the right weight", "slightly underweight" and "very underweight".
Self-weighing frequency: Participants were asked about their self-weighing frequency: "several times per day", "daily", "several times per week", "weekly", "occasionally".
Body shape: Participants were asked to choose, based on the standard figural stimuli developed by Stunkard and Stellar (21). Which silhouette is closest to your usual appearance? There are 6 silhouettes corresponding (from 1 to 6) to BMI of 17, 19, 21, 23, 25 and 27 approximately.
Dieting
Participants were asked whether they were dieting at the moment or not (yes/no), the reason or reasons for going on that diet (aesthetic reasons, healthy reasons -others than losing weight- or only with the specific objective of losing weight) and the intention of keeping on dieting or being about to do it (yes/no).
Self-reported physical fitness
Participants were asked about their physical fitness perception ("How do you consider your current physical fitness looks like"?) and they were classified as perceiving themselves as possessing a "poor", "fair", "average", "good" or "excellent" physical fitness.
Specific ED-related variables
Eating Attitudes Test-40 (EAT-40) (11,22): The EAT-40 has 40 items related to eating attitudes, which are rated on a six-point Likert scale (from never to always). Of these response options, three are scored with 1, 2 or 3 and the rest with 0. The maximum possible score is therefore 120, and a higher score corresponds to greater severity of disorder. The clinical cut-off point is usually considered to be 30. Factors that group together different items are bulimic behaviours, body image with a tendency toward thinness, laxative use or abuse, induced vomiting, restricted eating, eating in secret and perceived social pressure when weight increases. The EAT is the most widely-used self-report questionnaire for detecting disordered eating behaviours and its test-retest reliability ranges between 77% and 95%, with its positive and negative prediction values being 82% and 93%, respectively.
Eating Disorders Inventory-3 (EDI-3) (23,24): This inventory assesses three risk variables related to ED (in addition to nine psychological variables), and it is applicable in non-clinical samples from ten years on, both individually and collectively. For the present study there were taken those items related to specific ED variables (i.e., drive for thinness -DT-, bulimia -B-, and body dissatisfaction -BD-). The Spanish version of these scales has adequate internal consistency (Cronbach's α coefficients between 0.87 and 0.95).
The Spanish version of Body Image Quality of Life Inventory (BIQLI-SP) (16,25): The BIQLI is a self-reported questionnaire, which comprises 19 items. In order to avoid pathology-oriented biases, those items are evaluated on a 7-point bipolar scale, from +3 (very positive effect) to 0 (no impact) to -3 (very negative effect). The Spanish version (BIQLI-SP) was used for the current study. BIQLI-SP has shown high internal consistency (Cronbach's α coefficient = 0.95) and high stability over a 3-week period (test-retest reliability = 0.84). The validity of the BIQLI-SP has been evidenced by its significant relationships with different variables, both psychological and psychopathological, as well as with eating disorder-related variables.
Other psychological variables
Body Appreciation Scale (BAS) (15,26): This 13-item instrument comprises a single dimension and shows adequate internal consistency (Cronbach's α coefficient = 0.94) and construct validity. It seems to be useful for studying the positive aspects of body image. BAS items are rated along a 5-point scale (i.e., 1 = never, 2 = seldom, 3 = sometimes, 4 = often, 5 = always) and are averaged to obtain an overall body appreciation score. When giving the BAS to men item 12 is revised to: "I do not allow unrealistically muscular images of men presented in the media to affect my attitudes toward my body". Again the Spanish version of the BAS was used here, which has shown adequate psychometric properties (Cronbach's α coefficient = 0.91).
Self-esteem scale (SES) (27,28): The Spanish version of this scale was used. It comprises 10 items that are scored with a Likert format (from strongly agree to strongly disagree; the higher the score, the higher the degree of self-esteem). Reliability in the Spanish population has been shown to be adequate (Cronbach's α coefficient = 0.87), with test-retest correlation of 0.72.
General Health Questionnaire-28 (GHQ-28) (29,30): For this study we used the Spanish version of this screening instrument of general psychopathology which, taking into account a cut-off point of 6-7, shows a sensitivity of 76.9% and a specificity of 90.2%. With a cut-off point of 5-6 the questionnaire shows a sensitivity of 84.6% and a specificity of 82%. Anyhow, it shows an adequate discriminative power (psychiatric case-no case) and it is easy to be administered. The questionnaire was designed to detect the presence of psychiatric cases in community and non-psychiatric clinical settings and comprises four 7-item scales: somatic symptoms, anxiety and insomnia, social dysfunction and depression. Each item is accompanied by four possible responses: Not at all, No more than usual, Rather more than usual, and Much more than usual. As usual, GHQ-28 was scored with a binary method where Not at all, and No more than usual score 0, and Rather more than usual and Much more than usual score 1. By means of this scale of 0,0,1,1, the results are utilised to identify psychiatric cases. A higher final score indicates a greater psychopathology. Since there have been handled different cut-off points, only the total score has been considered in the present study. The GHQ has been suggested as a tool for identifying emerging problems as well as to identify chronic problems.
SETTING AND PROCEDURE
All participants attended the CAD regularly and they were practising one of the following three modalities of dance: -Spanish-flamenco dance (40.26%), contemporary dance (32.47%) or neoclassic dance (27.27%). After having obtained the CAD Director's permission and the students' informed consent, participants fulfilled the questionnaires and scales individually and without time limits. Measurements were taken individually. The procedure was supervised by a nutritionist, instructing the participants about how to complete the questionnaires and scales until they were completely sure about their fully understanding of the instructions. That nutritionist was also in charge to resolve any doubts about the tasks when carrying them out. The participants developed their task in a suitable setting. As we noted above, all the participants volunteered to take part in the study, none of them received any kind of reward after fulfilling the task and anonymity was guaranteed. Some nutritionists with experience in this type of studies were in charge to take anthropometric measures (weight and height). None of the participants left the study after inclusion. After the Director's permission and the ethics approval from Junta de Andalucía (Regional Government of Andalusia) were obtained, a timetable was established to collect the data during a week, avoiding evaluation periods in which possible distress could have influenced the study. In order not to alter the classes routine in the CAD, the questionnaires were filled in during the periods assigned by the Director and the anthropometric measures were collected in hours devoted to some other activities different from dancing. All students were invited to participate.
STATISTICAL ANALYSES
Conventional descriptive statistics (M, SD) were used to describe continuous variables and percentages for the categorical ones (n, %). Shapiro-Wilk normality test was used to determine whether the data fitted a normal distribution or not. As result, the robust Huber's model was applied in order to test the influence of the variables analysed (IV) on the EAT scores (DV). In case of categorical variables, the χ2-test or the Fisher's exact test were applied. All analyses were performed using R software, version 3.2.2.
Results
DESCRIPTIVE STATISTICS
As it was mentioned above, the sample comprised 77 dancers (20 males and 57 females) with a mean age of 21.22 (SD = 3.06) and the mean BMI was 21.01 (SD = 1.85).
Table I shows data considering: the fact of dieting, intention to go on a diet in the future and the aesthetic motivation for that proposal. Weight self-perception, self-reported physical fitness, self-weighing frequency and the reasons for that control are also showed.

Regarding the continuous variables (BAS, GHQ, specific subscales of EDI, BIQLI and SES), descriptives are represented in Table II.

Weight misperception and relations among weight self-perception, self-reported physical fitness and self-weighing
With respect to weight misperception, 8.45% of participants at normal weight perceived themselves as underweight and 33.80% of them perceived themselves as overweight. Among those who were under or overweight there was not any type of weight misperception. Overall 42.25% of participants misperceived their weight.
There seems to be a relationship between weight self-perception and self-reported physical fitness (χ216= 92.00; p < 0.001). Most of the participants (95,3%) who reported average, good or excellent physical fitness perceived themselves as on their weight. On the contrary, those participants who reported fair or poor physical fitness considered themselves as being slightly overweight (64.28%) and very overweight (100%) respectively. With respect to the self-weighing frequency, no significant differences were found considering self-reported physical fitness or about the reasons to do it (self control, maintenance/avoid gaining weight, feeling better).
BODY IMAGE
Referring to the actual weight status, 93.24% had a normal BMI (between 18.5 and 24.9). With respect to the silhouettes, the participants chose the numbers 1-5 with the following frequencies: 9 (11.68%), 24 (31.16%), 22 (28.57%), 20 (25.97%) and 2 (2.59%). None of the participants chose the silhouette number 6. The figural stimuli (Stunkard and Stellar, 1990) revealed than among the participants with a normal BMI, 5.79% identified themselves with the silhouette number 1 (which corresponds to a BMI about 17) and 2.89% with the silhouette number 5 (BMI = 25). On the other hand, those participants with an actual BMI < 18 and BMI ≥ 25 chose the silhouettes number 1 (BMI = 17) and 4 (BMI = 23) respectively.
GENDER DIFFERENCES
Considering sex, no significant differences were found with regards to self-reported physical fitness and the fact of dieting. Nevertheless, a significant difference was found with respect to weight self-perception (Fisher's Exact Test, p < 0.05). While the proportion of males and females who perceived themselves on their weight was similar (55.55% vs. 54.38%), 38.59% of females considered as being slightly or very overweight vs. 16.66% of males. Finally, 27.77% of males perceived themselves as being slightly or very underweight vs. 7.01% of females.
RELATIONS AMONG WEIGHT SELF-PERCEPTION, SELF-REPORTED PHYSICAL FITNESS, SELF-WEIGHING AND DIET
A significant relationship was found between weight self-perception and dieting (χ24 = 9.77; p < 0.05) as well as between weight self-perception and going on diet in the future (χ²4 = 13.94; p < 0.01). All participants who perceived themselves as very underweight or very overweight planned to go on a diet in the future. Among those who described themselves as being on their weight, slightly overweight or slightly underweight, 80%, 50% and 83.33% planned to diet respectively. A similar result was found with regards to the relation between diet for aesthetic reasons and weight self-perception (χ²4 = 14.48; p < 0.01). None of the participants who perceived themselves as slightly or very underweight planned to go on diet for aesthetic reasons, while all of those who felt to be very overweight and 69.56% among the participants who felt to be slightly overweight planned to do it.
No significant relations were found between self-reported physical fitness and dieting.
With respect to self-weighing, while the percentage of those who self-weighed weekly or several times per week was 29.16% among those who went on diet, this proportion was 7.68% in the case of participants who denied dieting (χ22 = 6.13; p < 0.05).
POSITIVE CASES RESPECTING EAT-40
Considering the traditional cut-off point (EAT-40 ≥ 30), 4 positive cases were found (5.19%). After applying the cut-off point of EAT-40 ≥ 21, proposed by Peláez-Fernández, et al. (20), which seems to give the best diagnostic prediction in our context, the number of positive cases was 14 (18.18%).
PREDICTION OF EAT SCORES (DC) BASED ON THE DIFFERENT VARIABLES ANALYZED (IV)
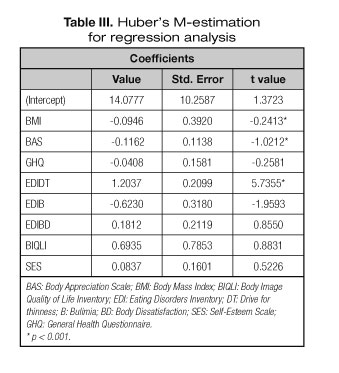
Mean, standard deviation and skew of EDI specific subscales suggested that these variables did not fit a normal distribution (Table II) as it was confirmed by means of the Shapiro-Wilk normality test. This is a trouble to perform a linear regression model so the robust Huber's model was applied in order to test the influence of the variables analysed (IV) on the EAT scores (DV). Linear least-squares estimates can behave badly when the error distribution is not normal, particularly when the errors are heavy-tailed. One remedy is to remove influential observations from the least squares fit. Another approach, robust regression, is to employ a fitting criterion that is not as vulnerable as least squares to unusual data (31). In this case the potential influential observations (outliers) are not data entry errors, neither are they from a different population than the data. So we had no compelling reasons to exclude them from the analysis. In this regards robust regression is a good strategy since it is a compromise between excluding these influential observations entirely from the analysis and including all the data points and treating all them equally (32). The results of the Huber's M-estimator are shown in table III. BMI, BAS and EDIDT have significant influence on the EAT-40 scores, this influence being no significant for the rest of variables. Despite having observed sex differences, these differences did not reach statistical signification (Figs. 1-3).



Discussion
With respect to our first hypothesis (a positive relationship between dance and higher prevalence of risk for ED), it must be noted that ED in dancers are thought to be common but the exact rates remain to be clarified (7). The dancer group has an overall prevalence of 16.4% with higher mean scores on the EAT-26 and the EDI subscales, so dancers seem to have a higher risk of suffering from ED as it has been reported recently (7). In the current study it is possible to note that there is a high risk of ED, considering the cut-off point of 21 for the EAT-40 (18.18%). This risk is higher than the one found in students (5.95%-9.43%) but in this case the cut-off point of the EAT-40 was 30 (17,18,33). In the current study, when the cut-off point was 30, the percentage of positive cases was clearly lower (5.19%). Previous studies have shown that the prevalence of AN in ballerinas ranges from 2% to 7% (34). In our study the positive cases were not confirmed by means of a clinical interview, our aim being to study the risk for ED in the specific group of dancers. According to the World Health Organization, the majority of ballerinas have below body weight (a risk factor for ED) (9), which was not found in the current study (only 7.79% of our sample had a BMI ≤ 18.5). The prevalence of risk for ED is not clear with our results because it seems to depend directly of the cut-off point applied for the EAT-40. Considering the BMI, the majority of the dancers were at normal weight. In this regards our results do not confirm that dancers are more similar to eating-disordered individuals than to control individuals on measures of eating pathology (2). With respect to the BMI, Wyon et al. (35) have reported that professional dancers had significantly greater BMI than student dancers, so a low BMI as risk factor for ED among dancers seems to remain controversial. Apart from the different cut-off point there is a factor, which could have influenced on our results. As it was noted previously, the CAD is not a "professional Centre of dance" so the attendants practice dance as a semi-professional activity or hobby. In addition, previous research has been focused on ballet dancers while this study includes other very different disciplines. These facts, along with a bit different mean age with respect to the reported in other articles must be taken into account for future studies: in our case 21.22 while other studies report, for example, 13-20 years old (4) or 25 years old (9). In fact, Wyon et al. (35) reported higher EAT-26 scores for female ballet dancers in years 10 and 12. So our first hypothesis was partially confirmed when we used the cut-off point of 21 with respect to the EAT-40.
Our second hypothesis (it is expected a relationship between eating attitudes and psychological variables such as self-esteem, mental health, specific EDI subscales, body appreciation and body image quality of life) was also partially confirmed. In this regard, BMI, body appreciation and EDI-DT (drive for thinness) significantly predicted the scores on the EAT-40. Higher BMI, lower scores on BAS and higher scores on EDI-DT predict higher scores on EAT-40. In other studies with dance students, low self-esteem, high neuroticism, and high psychological distress have proved to be associated with ED as well as teasing for overweight and body image dissatisfaction (36). These results are not specific because the negative relationship between BMI-BAS and BAS-drive for thinness has been reported in previous studies (15). The relationship between EAT-40 and self-esteem and GHQ scores was negative but not significant statistically.
Comparing with other populations the percentage of participants who went on a diet at the moment of this study (31.57%) was significantly higher (33). In the current study there were no significant gender differences with respect to go on a diet and planning to do it for aesthetic reasons, this being different considering other types of participants. In this regard, among students who go on a diet or plan to do it for aesthetic reasons more than 60% has been reported to be females (33). Self-weighing frequency was also different when compared with other studies based on other types of participants. While in the current study 3.94% self-weighed several times per week this percentage was 2.29 in a previous study among secondary school students (37). Considering weight misperception, the percentage of participants who misperceived their weight was significantly higher than the reported in previous studies in our context (23.5%-27.48%) (33,37), and similar to others such as Ruiz-Prieto et al. (41.35%) (38). In some countries, culturally different comparing with Spain (e.g., Ghana), approximately 20-21% of undergraduate students misperceives their weight status (39). The different age ranges and types of participants do not permit to compare these percentages in order to conclude something specific about the weight misperception among dancers. Authors such as Urdapilleta et al. (40) have highlighted that dancers have a more realistic perception of their body weight but bearing in mind the literature, this point remains unclear.
With regards to our third hypothesis (it is expected a more prevalence of going on diet and/or more self-weighing frequency and more discrepancies between the actual weight and the weight perception, assessing the weight as normal or above average while actually being underweight), it has been confirmed. On the one hand dancers seem to diet more frequently than other populations. Considering gender, there is a substantial difference with respect to other people. While generally females diet more frequently than men do, in the case of dancers there are not significant differences between women and men. Another difference must be noted with regards to self-weighing frequency, which in the case of dancers seems to be a bit higher.
Taking into account the silhouettes of Stunkard & Stellar (21), overall 85.13% of dancers chose the silhouettes numbers 2-4, which correspond to normal BMI. The BIQLI showed that the mean was positive, which indicates a positive body image quality of life. In a recent study with students the silhouettes numbers 2-4 were chosen by 75.84% (37) and other study (38) revealed an EDI-BD score of 6.13 among students, which is higher than the one found in the current study (4.75). In this regard body dissatisfaction and body distortion among dancers seem not to be worse than the reported in other populations. In short, our fourth hypothesis was not confirmed.
Summarizing, our results do no confirm that dancers have higher risk of ED at least in this group of participants who attend a specific Centre in Andalusia and when the most strict cut-off point was applied. Scores on EAT-40 and BMI do not suggest higher risk comparing with other populations. The current results show the relationship between EAT-40 scores and variables such as BMI, body appreciation and drive for thinness in this dancers group. A higher BMI, associated to lower body appreciation and higher drive for thinness could be a potential risk cluster for disordered eating attitudes.
There is a point that should be highlighted with respect to the fact of dieting. The concern about weight among dancers might lead to a high frequency of going on a diet as it is observed in our results. Nevertheless, there are not significant gender differences in this regard, which is not the case in other populations in which females are more likely to go on a diet. Dance could be considered as an activity, which implies similar behaviours to control weight in men and women. Something similar occurs when considering self-weighing, a behaviour more frequent among dancers than in other groups. A third element to note, along with dieting and self-weighing, is weight misperception. The probability that dancers have a more realistic perception of their body weight (40) has not been confirmed with our results. While other authors (33,37,38) have been reported a weight misperception ranging between 23.5%-41.35%, in this dancers group the percentage of weight misperception was 42.25%.
Finally, body dissatisfaction and body distortion among dancers are not worse than the reported in other populations taking into account our results referred to the silhouettes of Stunkard and Stellar (21), scores on the body image quality of life and level of body dissatisfaction as measured by the corresponding EDI subscale.
This study has some limitations. First, comparing to other studies this sample would be considered as a small one, so it is difficult to generalize the results. Another trouble to establish comparisons refers to the fact that while in our study the mean age was 21.22 others have reported mean ages from 14.4 (41) to 20.9 (42). Only one study (43) reported a higher mean age (34.4). Third, the characteristics of the CAD must be taken into account. Students at this Centre could be considered as semi-professionals dancers. Other studies have focused on students who practice dance as their main activity (4). In this regard the profile might be considerably different, this being a possible objection to establish comparisons with other studies. Another limitation could be highlighted considering that our work does not have considered a control group. In this regard we have referred to other similar studies focused on non-dancers students. With respect to our first hypothesis, a higher risk for ED could be mentioned provided that the less strict cut-off point of EAT-40 is applied. With the classical cut-off point these results do not support that hypothesis. Despite these limitations, our study adds some data in this field of study bearing in mind the use of a cluster of variables previously not taken into account as a whole.
References
1. Sundgot-Borgen J, Torstveit MK. Prevalence of eating disorders in elite athletes is higher than in the general population. Clin J Sport Med 2004;14:25-32. Disponible en: http://dx.DOI.org/10.1097/00042752-200401000-00005. [ Links ]
2. Ringham R, Klump K, Kaye W, Stone D, Libman S, Stowe S, et al. Eating disorder symptomatology among ballet dancers. Int J Eat Disord 2006;39:503-8. Disponible en: http://dx.DOI.org/10.1002/eat.20299. [ Links ]
3. Smethurst W, Wales J, Arcelus J. Puff the magic slimmer? Eur Eat Disord Rev 2010;18:431-3. Disponible en: http://dx.DOI.org/10.1002/erv.1059. [ Links ]
4. Herbrich L, Pfeiffer E, Lehmkuhl U, Schneider N. Anorexia athletica in pre-professional ballet dancers. J Sports Sci 2011;29,1115-23. Disponible en: http://dx.DOI.org/10.1080/02640414.2011.578147. [ Links ]
5. Gunnard K, Krug I, Jiménez-Murcia S, et al. Relevance of social and self-standards in eating disorders. Eur Eat Disord Rev 2012;20:271-8. Disponible en: http://dx.DOI.org/10.1002/erv.1148. [ Links ]
6. Penniment KI, Egan SJ. Perfectionism and learning experiences in dance class as risk factors for eating disorders in dancers. Eur Eat Disord Rev 2012;20:13-23. Disponible en: http://dx.DOI.org/10.1002/erv.1089. [ Links ]
7. Arcelus J, Haslam M, Farrow C, Meyer C. The role of interpersonal functioning in the maintenance of eating psychopathology: A systematic review and testable model. Clin Psychol Rev 2013;33:156-67. Disponible en: http://dx.DOI.org/10.1016/j.cpr.2012.10.009. [ Links ]
8. Fairburn CG, Brownell KD. Eating Disorders and Obesity: A Comprehensive Handbook. The Guilford Press: New York; 2002. [ Links ]
9. Zoletić E, Duraković-Belko E. Body image distortion, perfectionism and eating disorder symptoms in risk group of female ballet dancers and models and in control group of female students. Psychiatr Danub 2009;21:302-9. [ Links ]
10. Nordin-Bates SM, Walker IJ, Redding E. Correlates of disordered eating attitudes among male and female Young talented dancers: findings from the UK centres for advanced training. Eat Disord 2011;19:211-33. Disponible en: http://dx.DOI.org/10.1080/10640266.2011.564976. [ Links ]
11. Garner DM, Garfinkel PE. The Eating Attitudes Test: An index of the symptoms of anorexia nervosa. Psychol Med 1979;9:273-9. [ Links ]
12. Garner DM, Olmsted MP, Bohr Y, Garfinkel PE. The eating attitudes test: psychometric features and clinical correlates. Psychol Med. 1982;12:871-8. [ Links ]
13. Garner DM, Olmstead M, Polivy J. Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Int J Eat Disord 1983;2:15-34. Disponible en: http://dx.DOI.org/10.1002/1098-108X(198321)2:23.0.CO;2-6. [ Links ]
14. Henderson M, Freeman CP. A self-rating scale forbulimia. The "BITE". Br J Psychiatry. 1987;150:18-24. Disponible en: http://dx.DOI.org/10.1192/bjp.150.1.18. [ Links ]
15. Jáuregui-Lobera I, Bolaños-Ríos P. Spanish version of the Body Appreciation Scale (BAS) for adolescents. Span J Psychol 2011;14:411-20. Disponible en: http://dx.DOI.org/10.5209/rev_SJOP.2011.v14.n1.37. [ Links ]
16. Jáuregui-Lobera I, Bolaños-Ríos P. Body image and quality of life in a Spanish population. Int J Gen Med 2011;4,63-72. Disponible en: http://dx.DOI.org/10.2147/IJGM.S16201. [ Links ]
17. Jáuregui-Lobera I, Romero-Candau J, Bolaños-Ríos P, et al. Eating behaviour and body image in a sample of adolescents from Sevilla. Nutr Hosp 2009;24:568-73. Disponible en: http://dx.DOI.org/10.3305/nh.2009.24.5.4486. [ Links ]
18. Jáuregui-Lobera I, Romero-Candau J, Montaña-González MT, Morales-Millán MT, Vargas-Sánchez N, León-Lozano P. Analysis of eating attitudes in a sample of adolescents from Sevilla. Med Clin (Barc) 2009;132:83-8. Disponible en: http://dx.DOI.org/10.1016/j.medcli.2008.07.001. [ Links ]
19. Jáuregui-Lobera I, Bolaños-Ríos P, Santiago-Fernández MJ, Garrido-Casals O, Sánchez E. Perception of weight and psychological variables in a sample of Spanish adolescents. Diabetes Metab Syndr Obes 2011;4:245-51. Disponible en: http://dx.DOI.org/10.2147/DMSO.S21009. [ Links ]
20. Peláez-Fernández MA, Ruiz-Lázaro PM, Labrador FJ, Raich RM. Validation of the Eating Attitudes Test as a screening instrument for eating disorders in general population. Med Clin (Barc) 2014;142:153-5. Disponible en: http://dx.DOI.org/10.1016/j.medcli.2013.03.018. [ Links ]
21. Stunkard A, Stellar E. Eating and its disorders. In: Cash T, Pruzinsky T, edits. Body Images. New York: Guilford Press; 1990. p. 3-20. [ Links ]
22. Castro J, Toro J, Salamero M, Guimerá E. The Eating Attitudes Test: Validation of the Spanish version. Psychol Assess 1991;7:175-90. [ Links ]
23. Garner DM. Eating Disorder Inventory- 3 Professional manual. Odessa, Fl: Psychological Assessment Resources; 2004. [ Links ]
24. Elosua P, López-Jáuregui A, Sánchez-Sánchez F. Manual técnico con la adaptación al euskera del Eating Disorder Inventory-3. Madrid: TEA Ediciones; 2010. [ Links ]
25. Cash TF, Fleming EC. The impact of body-image experiences: Development of the Body Image Quality of Life Inventory. Int J Eat Disord 2002;31:455-60. Disponible en: http://dx.DOI.org/10.1002/eat.10033. [ Links ]
26. Avalos L, Tylka TL, Wood-Barcalow N. The Body Appreciation Scale: Development and psychometric evaluation. Body Image 2005;2:285-97. Disponible en: http://dx.DOI.org/10.1016/j.bodyim.2005.06.002. [ Links ]
27. Rosenberg M. Society and the adolescent self-image. Princeton, NJ: Princeton University Press; 1965. [ Links ]
28. Vázquez AJ, Jiménez R, Vázquez-Morejón R. The Rosenberg Self- Esteem Scale: Reliability and validity in clinical samples of Spanish population. Apuntes de Psicología 2004;22:247-55. [ Links ]
29. Goldberg P, Hillier VF. A scaled version of the General Health Questionnaire. Psychol Med 1979;9:139-45. Disponible en: http://dx.DOI.org/10.1017/S0033291700021644. [ Links ]
30. Lobo A, Pérez-Echevarría MJ, Artal J. Validity of the scaled version of the General Health Questionnaire (GHQ-28) in a Spanish population. Psychol Med 1986;16:135-40. Disponible en: http://dx.DOI.org/10.1017/S0033291700002579. [ Links ]
31. Fox J, Weisberg S. Robust regression in R. In: Fox J, Weisberg S (eds). An R Companion to Applied Regression. 2.a ed. Thousand Oaks: Sage publications; 2011. [ Links ]
32. Fox J. Applied regression analysis, linear models, and related models. Thousand Oaks: Sage publications; 1997. [ Links ]
33. Jáuregui-Lobera I, Ezquerra-Cabrera M, Carbonero-Carreño R, Ruiz-Prieto I. Weight misperception, self-reported physical fitness, dieting and some psychological variables as risk factors for eating disorders. Nutrients 2013;5:4486-502. Disponible en: http://dx.DOI.org/10.3390/nu5114486. [ Links ]
34. Szmukler GI, Eisler I, Gillies C, Hayward ME. The implication of anorexia nervosa on a ballet school. J Psychiatr Res 1985;17,177-81. Disponible en: http://dx.DOI.org/10.1016/0022-3956(85)90015-9. [ Links ]
35. Wyon MA, Hutchings KM, Wells A, Nevill AM. Body mass index, nutritional knowledge, and eating behaviors in elite student and professional ballet dancers. Clin J Sport Med 2014;24:390-6. Disponible en: http://dx.DOI.org/10.1097/JSM.0000000000000054. [ Links ]
36. Liu CY, Tseng MC, Chang CH, Fang D, Lee MB. Comorbid psychiatric diagnosis and psychological correlates of eating disorders in dance students. J Formos Med Assoc 2015;115:113-20. Disponible en: http://dx.DOI.org/10.1016/j.jfma.2015.01.019. [ Links ]
37. Hernández-Camacho JD, Rodríguez-Lazo M, Bolaños-Ríos P, Ruiz-Prieto I, Jáuregui-Lobera I. Eating habits, excess weight and weight self-perception at school. Nutr Hosp 2015;32:1334-43. Disponible en: http://dx.DOI.org/10.3305/nh.2015.32.3.9351. [ Links ]
38. Ruiz-Prieto I, Carbonero-Carreño R, Jáuregui-Lobera I. Weight misperception and physical fitness perception in relation to the physical activity level, dietary behaviour and psychosocial well-being. Nutr Hosp 2014;31:203-16. Disponible en: http://dx.DOI.org/10.3305/nh.2015.31.1.8119. [ Links ]
39. Mogre V, Aleyira S, Nyaba R. Misperception of weight status and associated factors among undergraduate students. Obes Res Clin Pract 2015;9:466-74. Disponible en: http://dx.DOI.org/ 10.1016/j.orcp.2015.03.002. [ Links ]
40. Urdapilleta I, Cheneau C, Masse L, Blanchet A. Comparative study of body image among dancers and anorexic girls. Eat Weight Disord 2007;12:140-6. [ Links ]
41. Toro J, Guerrero M, Sentis J, Castro J, Puertolas C. Eating disorders in ballet dancing students: problems and risk factors. Eur Eat Disord Rev 2009;17:40-9. Disponible en: http://dx.DOI.org/10.1002/erv.888. [ Links ]
42. Holderness CC, Brooks-Gunn J, Warren MP. Eating disorders and substance use: a dancing vs a nondancing population. Med Sci Sports Exerc 1994;26:297-302. Disponible en: http://dx.DOI.org/10.1249/00005768-199403000-00005. [ Links ]
43. Nascimento AL, Luna JV, Fontenelle LF. Body dysmorphic disorder and eating disorders in elite professional female ballet dancers. Ann Clin Psychiatry 2012;24,191-4. [ Links ]
![]() Correspondence:
Correspondence:
Ignacio Jáuregui-Lobera.
Behavioural Sciences Institute,
Calle Fernando IV, 24-26.
41011 Sevilla, Spain
e-mail: ignacio-ja@telefonica.net
Received: 16/04/2016
Accepted: 10/05/2016
