










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 no.6 Madrid nov./dic. 2016
https://dx.doi.org/10.20960/nh.795
TRABAJO ORIGINAL / Valoración nutricional
Difference in fatty acids composition of breast adipose tissue in women with breast cancer and benign breast disease
Diferencia en la composición de ácidos grasos del tejido adiposo de la mama en mujeres con cáncer de mama y enfermedad benigna de la mama
Lisiane Lopes da Conceição1, Mariana de Moura e Dias1, Milene Cristine Pessoa1, Geórgia das Graças Pena2, Maria Carolina Santos Mendes1, Cristiane Vilas Boas Neves2, Helen Hermana Miranda Hermsdorff1, Renata Nascimento de Freitas2 and Maria do Carmo Gouveia Peluzio1
1Department of Nutrition and Health. Laboratory of Nutritional Biochemistry. Universidade Federal de Viçosa. Viçosa, MG. Brazil.
2Center of Biological Sciences Reseach - NUPEB, Molecular Epidemiology Laboratory. Universidade Federal de Ouro Preto. Ouro Preto, MG. Brazil
The authors thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) Brasília, Brazil, Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) Brasília, Brazil, and Fundação de Amparo à Pesquisa de Minas Gerais (FAPEMIG) Belo Horizonte, Brazil for their financial support. M.C.G.P. and H.H.M.H are CNPq fellows. L.L.C. is the recipient of CAPES grant.
ABSTRACT
Introduction: Breast cancer is the second most common cancer in the world, and the most frequent cancer among women. Moreover, there are factors that influence the risk for breast cancer including the age, genetic and endocrine factors, and lifestyle.
Objectives: To evaluate the consumption of fatty acids; compare the fatty acids composition in the breast adipose tissue of women with breast cancer and benign breast disease as well as potential risk factors; and describe the genotypic frequency of the Pro12Ala PPARγ polymorphism.
Material and methods: A hospital-based case-control study was conducted including incident cases (n = 38 breast cancer; n = 75 benign breast disease; n = 166 control). Lifestyle features, socioeconomic issues, dietary intake, anthropometry, and blood and tissue data were assessed.
Results: No differences were observed for fatty acids intake. Interestingly, lauric acid (p = 0.001), myristic acid (p = 0.036), stearic acid (p = 0.031), and total saturated fatty acids (SFAs) (p = 0.048) had lower concentrations in BC than in BBD women, while palmitoleic acid (p = 0.022), erucic acid (p = 0.002), total monounsaturated fatty acids (MUFAs) (p = 0.039) and oleic acid/stearic acid ratio (p = 0.015) increased. There was no significant association between PPARγ polymorphism and studied groups (p = 0.977). The age at first full pregnancy (p = 0.004) was significantly associated with the development BC, whereas BMI (p = 0.005); percentage of body fat (p = 0.024); physical activity (p = 0.036); and age at menarche (p = 0.008), at first full pregnancy (p < 0.001), and of first mammogram (p = 0.018) were significantly associated with the development of BBD.
Conclusion: The results suggest a different fatty acids composition of breast adipose tissue, a biomarker of long-term dietary intake, particularly for SFAs, MUFA and 18: 1 n-9/18: 00 ratio. Our findings also show that are differences in the factors related to the development of BC and BBC.
Key words: Fatty acids. Breast cancer. Benign breast disease. PPARγ. Dietary intake.
RESUMEN
Introducción: el cáncer de mama (CM) es el segundo cáncer más común en el mundo, y el cáncer más frecuente entre las mujeres. Por otra parte, hay factores que influyen en el riesgo de padecer CM, entre los que se encuentran la edad, factores genéticos y endocrinos, y el estilo de vida.
Objetivos: evaluar el consumo de ácidos grasos; comparar la composición de ácidos grasos en el tejido adiposo de mama de las mujeres con CM y enfermedad benigna de mama (EBM), así como los posibles factores de riesgo; y describir la frecuencia genotípica del polimorfismo Pro12Ala PPARγ.
Material y métodos: se llevó a cabo un estudio caso-control basado en hospitales, incluyendo casos incidentes (n = 38 cáncer de mama, n = 75 enfermedad benigna de mama, n = 166 control). Se evaluaron las características del estilo de vida, las cuestiones socioeconómicas, la ingesta dietética, la antropometría y los datos de sangre y tejidos.
Resultados: no se observaron diferencias para la ingesta de ácidos grasos. Curiosamente, ácido láurico (p = 0,001), ácido mirístico (p = 0,036), ácido esteárico (p = 0,031) y los ácidos grasos totales saturados (AGS) (p = 0,048) tenían concentraciones más bajas en CM que en mujeres EBM, mientras ácido palmitoleico (p = 0,022), ácido erúcico (p = 0,002), los ácidos totales grasos monoinsaturados (MUFA) (p = 0,039) y la relación ácido oleico/ácido esteárico (p = 0,015) aumentó. No hubo asociación significativa entre el polimorfismo PPAR gamma y los grupos de estudio (p = 0,977). La edad al primer embarazo (p = 0,004) se asoció de forma significativa con el desarrollo de CM, mientras que el IMC (p = 0,005), porcentaje de grasa corporal (p = 0,024), la actividad física (p = 0,036) y la edad de la menarquia (p = 0,008), al primer embarazo (p < 0,001), y de la primera mamografía (p = 0,018), fueron significativamente asociados con el desarrollo de EBM.
Conclusiones: los resultados sugieren una composición diferente de ácidos grasos del tejido adiposo de la mama, un biomarcador de la ingesta dietética a largo plazo, particularmente para SFA, MUFA y 18: 1 n-9/18: 00. Nuestros hallazgos también muestran que existen diferencias en los factores relacionados con el desarrollo de CM y EBM.
Palabras clave: Acidos grasos. Cancer de mama. Enfermedad benigna de mama. PPARγ. Ingesta dietetica.
Introduction
Breast cancer (BC) is the second most common cancer in the world, and the most frequent cancer among women (1). There are several recognized risk factors for BC, mainly age, genetic and endocrine factors, and lifestyle (2). It is estimated that up to 35% of risk factors are associated with diet (3).
However, the assessment of the association of diet components with BC risk is not an easy task because of the limitations of conventional methods to assess dietary intake, such as memory, difficulty in estimating portion size, day-to-day variability, seasonal eating patterns, and use of the food consumption tables (4,5). In fact, the determination of tissue nutrients may provide a more accurate estimate of dietary intake. The fatty acid (FA) content of the adipose tissue has been proposed as a biomarker of FA intake most appropriate because it reflects the long-term ingestion, up to 2 years previous, when no severe weight loss had occurred (6).
The peroxisome proliferator-activated receptor gamma (PPARγ) has been shown to be important in many biochemical functions such as the adipocyte differentiation and also act as a tumor suppressor gene, inhibiting the growth of several cell types, and induction of apoptosis (7). However, until this moment, studies investigating the association between PPARγ polymorphism and the risk of BC reported inconclusive results (8-14).
Overall, the aims of this study were to evaluate the consumption of fatty acids; to compare the fatty acids composition of the breast adipose tissue of women with BC and benign breast disease (BBD); to identify factors associated with risk of developing of BC and BBD; as well as to describe the genotypic frequency of PPARγ Pro12Ala polymorphism.
Materials and methods
SAMPLE STUDY
This is a double-blind, hospital-based, case-control study conducted with women attending the mastology and/or gynecology service of a public hospital in Belo Horizonte, Brazil. All women attended between January and July 2006 was invited to participate in the study. In this study, we included only women without previous diagnosis of BC or BBD. The volunteers were divided in three groups: case, women with histological diagnosis of malignant breast disease; BBD, women diagnosed with fibrocystic breast changes or other non-proliferative BBD; and Control (C) women who underwent a routine examination or gynecological surgery and had a recent mammogram result. The final sample was composed of 229 women. Written consent was given by all women after they had been informed of the objective and protocol of the study. The study followed principles of the Declaration of Helsinki and was approved by the National Committee of Ethics in Research (protocol number: 1889/2005).
DATA COLLECTION
Information about lifestyle, as well as gynecological and obstetric history, and socioeconomic issues were collected using a previously validated questionnaire for the population of the region studied (15). Dietary intake was assessed using a semiquantitative food frequency questionnaire (SFFQ).
Volunteers who consumed at least 1 dose (10 g of alcohol) of any alcoholic beverage/day or in a frequency of more than 3 days/week were considered alcoholic (16). In the same way, who smoked at least 1 cigarette per day, regardless of the time of use were considered smokers. Physical activity was assessed using the short version of international physical activity questionnaire (IPAQ) (17).
Anthropometric measurements such as weight, height, waist, and hip circumference were obtained from all the participants according to the standard protocol (18-20). The waist to hip ratio (WHR), waist to height ratio (WHtR), and body mass index (BMI in kg/m2) were calculated. Overweight and obesity were defined as BMI ≥ 25.0 to 29.9 kg/m2 and ≥ 29.9 kg/m2, respectively (21).
Moreover, the total body fat (%) was estimated by bioelectrical impedance vertical Tanita® (ModelTBF 531, Tanina Corporation of America, Illinois, USA) and classified by Gallagher et al. (22).
The collection of biological material occurred on the day of surgery after 12 h fasting. Blood and breast adipose tissue samples were collected and immediately protected from light and stored in liquid nitrogen at -80 oC until the time of analysis.
FATTY ACIDS IN BREAST ADIPOSE TISSUE
The lipids of the breast adipose tissue were extracted by Folch (23) methodology and saponified and esterified according to Hartmann and Lago (24). The FA methyl esters were identified by gas chromatography (CG-17A Shimadzu®/Class model) (25). Peak identification was made by comparison of their retention times with that of a mixture of commercial standards (FAME mix, Supelco®, USA). FA composition was expressed as percentage of the lipid fraction relative to the total FA content of the sample.
GENOTYPING
Genomic DNA was obtained from stored buffy coat. Briefly, buffy coats were digested using lysing solution, Madissen (0.1M Tris-HCl pH = 8.0; 0.4 M EDTA; 0.2% SDS; 1M NaCl; pH = 8.0), followed by addition of proteinase K (20 mg/mL) and incubated overnight at 37 oC. Then, the DNA was precipitated with saturated phenol and chloroform:isoamyl alcohol (24:1). Finally, cold isopropyl alcohol was added and homogenized slowly until the precipitation of DNA, which was dried at room temperature.
To detect the presence the proline 12 alanine (Pro12Ala) polymorphism, a 257-bp fragment of the PPARγ gene was selectively amplified by PCR (26). The amplified fragment was digested with the restriction enzyme BstU-I according to manufacturer's instructions (Promega®, Madison, WI, USA), and the products of digestion were analyzed in polyacrylamide gel. The genotyping of patients were determined as follows: a single 257 bp fragment for the CC (Ala12Ala) genotype; two fragments of 223 and 34 bp for the GG (Pro12Pro) genotype; and three fragments of 257, 223, and 34 bp for the CG (Pro12Ala) genotype.
STATISTICAL ANALYSES
Normal distribution of data was determined by Kolmogorov-Smirnov test. The Kruskal-Wallis and analysis of variance (ANOVA) was used to determine the differences in median and mean values, respectively, between the BC, BBD, and C groups. Associations between categorical variables were tested by Pearson's chi-squared test, and when necessary the chi-square partition test with Bonferroni correction was utilized. Odds Ratio and 95% confidence intervals for risk of BC and BBD were examined using multinomial logistic regression. Initially, we applied simple multinomial logistic regression and the independent variables with significance < 0.20 were considered as candidates for the final model. Then, multiple multinomial logistic regressions were conducted in which the variables remained with a final model with significance level of α ≤ 0.05.
The food consumption data were log-transformed before statistical analyses, and the data were adjusted by energy according to the residual model (27).
Hardy-Weinberg Equilibrium was tested to compare the observed with expected genotype frequencies. Frequencies of the genotypes of PPARγ polymorphism between the study groups was performed by the chi-square test. All analyses were conducted in SPSS®software, version 20.
Results
The anthropometric, clinical, sociodemographic and lifestyle characteristics of BC, BBD, and C are described in table I. As it can be seen, the median age was higher in BC group (p < 0.001), and they made less use of oral contraceptives (p = 0.011). Furthermore, when compared to BBD group, women with BC had made ??their first mammogram (p < 0.001) at a later age and presented menopause at an older age too (p = 0.037) suggesting a longer interval between ages at menarche and natural menopause.

.jpg)
However, in control group, women had the first full pregnancy younger (p < 0.001). While women without the disease had breastfed more (p < 0.001), had no family history of breast cancer (p < 0.001), or previous history of benign breast lesion (p < 0.001). The others parameters did not differ between the study groups.
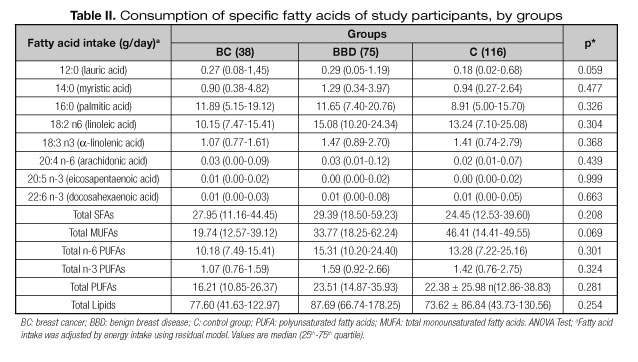
In relation to food consumption, no differences were observed between the three evaluated groups (Table II). However, the composition of fatty acids from the breast adipose tissue was different between groups (Table III). The tissue concentration of lauric acid, myristic acid, stearic acid, and total saturated fatty acids (SFAs) were lower in BC than in BBC, while palmitoleic acid, erucic acid, total MUFAs, and oleic acid/stearic acid ratio were higher in BC than in BBC, reinforcing the hypothesis regarding the necessity of balance in consumption of fatty acids in dietary lipids.

The observed frequency of genotypes was not different from the expected frequency demonstrating to be in Hardy-Weinberg equilibrium in this population. Moreover, no significant association was observed between PPARγ Pro12Ala polymorphism and studied groups (p = 0.977). The percentage of women with the genotype CG or GG was 17.4, 30.4, and 52.2%, in the BC, BBD, and C groups, respectively.
About the risk factors, it was observed that the age at first full pregnancy (p = 0.004) was highlighted in this study as an important factor associated with the development of BC. In addition, for women with BBD, BMI (p = 0.005), total body fat (p = 0.024), physical activity (p = 0.036), and age at menarche (p = 0.008), at first full pregnancy (p < 0.001), and of first mammogram (p = 0.018) were pointed as risk factors for the occurrence of BBD (Table IV).

Discussion
Great efforts have been made in the scientific community to improve our understanding of the factors associated with breast cancer (1). However, few studies assessed the BBD and its risk factors as well the behavior of this disease.
We found that women with BC had the menopause in older age. Recent study reported that women with the longest reproductive lifespan were 1.5-1.7 times more likely to have BC compared with women with the shortest reproductive lifespan (28).
However, in control group, women had the first full pregnancy at younger age, which is according to recent evidence to suggest that pregnancy at an early age has a strong protective effect against BC in humans, through changes in hormonal dynamics and pronounced changes in gene expression (29). In addition, in our study, the oral contraceptive use demonstrated a protective action, different from what has been described in the literature (30,31).
To our knowledge, this is the first case-control study that utilized WHtR as screening tool, and we found the difference between groups and WHtR. Recent evidence suggests that WHtR is a better measure of the health risk such as obesity and cardio-metabolic risk factors, wherein the larger the ratio the greater the risk.
In relation to the profile of fatty acid determined in patients with CA and DBM, our results were contrary to that described in the literature, and this can be possibly due to characteristics significantly different (Table I). Contrary to our results, concentrations of myristic acid were elevated in cancer breast tissue in Greek women (32). Greek patients with BC had significantly higher total MUFA (p < 0.001), lower total SFA (p < 0.01) in breast adipose tissue compared to patients with benign breast tumors, which is consistent with the present study (33). In addition, we suggest that the differences observed in this analysis of FA as biomarker intake (Table III), may occur due to differences in long-term food intake.
Our finding of a higher oleic acid/stearic acid ratio (p = 0.015) in BC women, also be attributed to the novel functions of enzyme stearoyl-CoA desaturase-1 (SCD1), related to cancer and possibly this enzyme may be overexpressed and highly active in women with BC in population. The SCD1 is a key regulator of lipid FA composition in mammalian cells and also responsible for the conversion of stearic acid to oleic acid. However, novel functions have been proposed to this enzyme like modulation of metabolic and signaling processes related to cell proliferation, survival, and malignant transformation to cancer. Thereby, has been proposed a relationship between SCD1 activity and tumor growth. In several types of cancers, elevated SCD1 expression and activity have been detected (34).
Even in relation to the polymorphism, others studies also found no association between PPARγ polymorphism and the risk of BC in different populations such as: Caucasian women (12); Mexican women (14); women living in Hawaii and California recruited in a Multiethnic Cohort study (13). These reinforce that the results are still inconclusive.
In this study, only age at first full pregnancy was significantly associated with the development BC, whereas BMI, total body fat, physical activity, and age at menarche, at first full pregnancy and of first mammogram associated of BBC. Epidemiological evidences show that there are factors associated with an increased risk of BC, such as gender being a woman is the strongest risk factor for BC, increasing age, younger age at menarche, and family history. Other factors are associated with a decreased risk, such as earlier age at first birth, breastfeeding, parity, and physical activity (35).
Conclusion
The findings of the present study strengthen the hypothesis that women with BC and BBD have different sociodemographic, anthropometric, reproductive, gynecological, and lifestyle characteristics. In addition, significant associations between specific breast tissue SFAs, MUFAs, and 18:1 n-9/18:0 ratio were observed and can be supported by a physiological mechanism involving the enzyme SCD1. No association was observed between PPARγ Pro12Ala polymorphism and the studied groups, which reinforces the need for further studies since the literature shows inconclusive results on this polymorphism and breast cancer.
References
1. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer; 2014. [ Links ]
2. McPherson K, Steel CM, Dixon JM. Breast cancer - epidemiology, risk factors and genetics. BMJ 2000;321:624-8. [ Links ]
3. Baena Ruiz R, Salinas Hernández P. Diet and cancer: Risk factors and epidemiological evidence. Maturitas 2014;77(3). [ Links ]
4. Bingham SA. Limitations of the various methods for collecting dietary intake data. Annals of Nutrition and Metabolism 1991;35(3):117-27. [ Links ]
5. Wynder EL, Cohen LA, Winters BL. The challenges of assessing fat intake in cancer research investigations. Journal of the American Dietetic Association 1997;97(Suppl.7)(7):S5-S8. [ Links ]
6. Arab L. Biomarkers of Nutritional Exposure and Nutritional Status. The Journal of Nutrition 2003;133:S925-S32. [ Links ]
7. Meirhaeghe A, Amouyel P. Impact of genetic variation of PPAR in humans. Molecular Genetics and Metabolism 2004;83:93-102. [ Links ]
8. Mao Q, Guo H, Gao L, Wang H, Ma X. Peroxisome proliferator-activated receptor gamma2 Pro12Ala (rs1801282) polymorphism and breast cancer susceptibility: a meta-analysis. Molecular Medicine Reports 2013;8(6):1773-8. [ Links ]
9. Memisoglu A, Hankinson SE, Manson JE, Colditz GA, Hunter DJ. Lack of association of the codon 12 polymorphism of the peroxisome proliferator-activated receptor gamma gene with breast cancer and body mass. Pharmacogenetics 2002;12(8):597-603. [ Links ]
10. Vogel U, Christensen J, Nexø BA, Wallin H, Friis S, Tjønneland A. Peroxisome profilerator-activated receptorgamma2 Pro12Ala, interaction with alcohol intake and NSAID use, in relation to risk of breast cancer in a prospective study of Danes. Carcinogenesis 2006;28(2):427-34. [ Links ]
11. Wang Y, McCullough ML, Stevens VL, Rodriguez C, Jacobs EJ, Teras LR, et al. Nested case-control study of energy regulation candidate gene single nucleotide polymorphisms and breast cancer. Anticancer Research 2007;27(1B):589-93. [ Links ]
12. Gallicchio L, McSorley MA, Newschaffer CJ, Huang H-Y, Thuita LW, Hoffman SC, et al. Body mass, polymorphisms in obesity-related genes, and the risk of developing breast cancer among women with benign breast disease. Cancer Detection and Prevention 2007;31(2):95-101. [ Links ]
13. Chen F, Wilkens LR, Monroe KR, Stram DO, Kolonel LN, Henderson BE, et al. No association of risk variants for diabetes and obesity with breast cancer: the multiethnic cohort and PAGE studies. Cancer Epidemiology, Biomarkers and Prevention 2011;20(5):1039-42. [ Links ]
14. Martínez-Nava GA, Burguete-García AI, López-Carrillo L, Hernández-Ramírez RU, Madrid-Marina V, Cebrián ME. PPARgamma and PPARGC1B polymorphisms modify the association between phthalate metabolites and breast cancer risk. Biomarkers 2013;18(6):493-501. [ Links ]
15. Oliveira RC. Avaliação dos fatores associados a neoplasia maligna da mama em mulheres atendidas no ambulatório de mastologia do Hospital e Maternidade Odette Valadares, Belo Horizonte - Minas Gerais. Viçosa: Universidade Federal de Viçosa; 2004. [ Links ]
16. WHO. Global Status report on alcohol 2004. Geneva: Word Health Organization; 2004. p. 88. [ Links ]
17. CELAFISCS. International Physical Activity Quationnaire - Short Version. São Caetano do Sul: Centro de Estudos do Laboratório de Aptidão Física São Caetano do Sul; 2004. [ Links ]
18. Frisancho AR. Anthropometric standarts for the assessment of growth and nutritional status. United States of America: University of Michigan Press; 1993. [ Links ]
19. Jelliffe DB. The assessment of the nutritional status of the community (with special reference to field surveys in developing regions of the world). Monogr Ser World Health Organ 1966;53:3-271. [ Links ]
20. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the Metabolic Syndrome A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009;120:1640-5. [ Links ]
21. WHO. Physical Status: the use and the interpretation of antropometry. Geneva: World Health Organization; 1995. p. 452. [ Links ]
22. Gallagher D, Heymsfield SB, Heo M, Jebb SA, Murgatroyd PR, Sakamoto Y. Health percentage body fat ranges: an approach for developing guidelines based on body mass index. The American Journal of Clinical Nutrition 2000;72:694-701. [ Links ]
23. Folch J, Lees M, Stanley GHS. A simple method for the isolation and purification of total lipides from animal tissues. The Journal of Biological Chemistry 1957;226(1):497-509. [ Links ]
24. Hartman L, Lago RCA. Rapid preparation of fatty acid methyl esters from lipids. Laboratory Practice 1973;22(6):475-6. [ Links ]
25. Rosa DD, Lourenço FC, Fonseca ACM, Sales RL, Ribeiro SMR, Neves CA, et al. Fish oil improves the lipid profile and reduces inflammatory cytokines in wistar rats with precancerous colon lesions. Nutrition and Cancer 2012;64(4):569-79. [ Links ]
26. Gong Z, Xie D, Deng Z, Bostick RM, Muga SJ, Hurley TG, et al. The PPARg Pro12Ala polymorphism and risk for incident sporadic colorectal adenomas. Carcinogenesis 2005;26(3):579-85. [ Links ]
27. Willett W, Stampfer MJ. Total energy intake: implications for epidemiologic analyses. American Journal of Epidemiology 1986;124(1):17-27. [ Links ]
28. Warren Andersen S, Trentham-Dietz A, Gangnon RE, Hampton JM, Figueroa JD, Skinner HG, et al. Reproductive windows, genetic loci, and breast cancer risk. Annals of Epidemiology 2014;25(4):367-82. [ Links ]
29. Meier-Abt F, Bentires-Alj M. How pregnancy at early age protects against breast cancer. Trends in Molecular Medicine 2014;20(3):143-53. [ Links ]
30. Beaber EF, Malone KE, Tang M-TC, Barlow WE, Porter PL, Daling JR, et al. Oral contraceptives and breast cancer risk overall and by molecular subtype among young women. Cancer Epidemiology Biomarkers and Prevention 2014;23(5):755-64. [ Links ]
31. Beaber EF, Buist DSM, Barlow WE, Malone KE, Reed SD, Li CI. Recent oral contraceptive use by formulation and breast cancer risk among women 20 to 49 years of age. Cancer Research 2014;74:4078-89. [ Links ]
32. Mamalakis G, Hatzis C, Bree E, Sanidas E, Tsiftsis DD, Askoxylakis J, et al. Adipose tissue fatty acids in breast cancer patients versus healthy control women from Crete. Annals of Nutrition and Metabolism 2009;54(4):275-82. [ Links ]
33. De Bree E, Mamalakis G, Sanidas E, Hatzis C, Askoxylakis I, Daskalakis M, et al. Adipose tissue fatty acid composition in Greek patients with breast cancer versus those with benign breast tumors. Anticancer Research 2013;33(4):1667-72. [ Links ]
34. Igal RA. Stearoyl-CoA desaturase-1: a novel key player in the mechanisms of cell proliferation, programmed cell death and transformation to cancer. Carcinogenesis 2010;31(9):1509-15. [ Links ]
35. National Breast and Ovarian Cancer Center. Breast cancer risk factors: a review of the evidence. National Breast and Ovarian Cancer Centre, Surry Hills, NSW; 2009. [ Links ]
![]() Correspondence:
Correspondence:
Lisiane Lopes da Conceição.
Department of Nutrition and Health.
Universidade Federal de Viçosa.
Avenue PH Rolfs, s/n.
Viçosa, Minas Gerais, 36570-900, Brazil
e-mail: lisianelopes@yahoo.com.br
Received: 26/05/2016
Accepted: 10/09/2016
