










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Muscular strength, one of the five components of health-related physical fitness, is associated with the ability to perform activities that require muscular force. The most commonly performed strength test for assessing this component is the measurement of grip strength with a hand grip dynamometer. The hand grip strength test provides useful and reliable information about overall health 1.
Several external factors are affecting results of the tests such as the angle of the shoulder, elbow, forearm, and wrist 2; the posture of the subject 3, and the grip span 4) (5. The grip span is concretely the most influential among the previous factors because hand and palm lengths 6, and palm width 7 are highly related to the strength performed during the dynamometry.
Different studies have investigated the optimal grip span for determining maximal hand grip strength in different populations such as adults 8, adolescents 4 and children 5. Firstly, Ruiz et al. 4 found that there was an optimal grip span to measure hand grip strength in teenagers. Similar results were found in children some years later by España-Romero et al. 5. However, to our knowledge, no studies on this regard have focused on persons with Down syndrome (DS), despite the relevance that this might have. Muscle hypotonicity and low muscular strength 9 are clinical characteristics among persons with DS. Concerning their hands, individuals with DS have a smaller hand size compared with their counterparts without the condition 10. For these reasons, it would be expected that individuals with DS would have a unique optimal grip span, different from the ones described for non-disabled adolescents. Thus, the aims of the present study were: a) to ascertain whether there is an optimal grip span for determining the maximal hand grip strength in adolescents with DS; and b) to define the specific span values for optimal grip span in this particular population.
MATERIAL AND METHODS
This study has been performed following the methodological considerations published elsewhere 4) (5) (8.
PARTICIPANTS
Two different groups of adolescents with DS were involved in this research. The optimal grip span was determined from the first group (27 adolescents with DS). Then, the usefulness and the reliability of the calculated optimal grip span were confirmed in a new group of 15 adolescents with DS.
PROCEDURES
MEASUREMENT OF HAND SPAN
Right and left hand spans, corresponding to the dominant and non-dominant hands, were measured with the hand widely opened, taking as reference from the tip of the thumb to the tip of the little finger. The precision of the measure was 0.1 cm, but the results of the hand span measurement were rounded to the nearest centimeter.
MEASUREMENT OF HANDGRIP STRENGTH
Hand grip strength was measured using a digital dynamometer (T.K.K. 5401 Grip-D; Takey, Tokyo, Japan), and the scores were recorded in kilograms (precision 0.1 kg). When performing the test, participants were instructed to maintain the standard bipedal position during the entire test with the shoulder in slight abduction, the elbow in complete extension, the forearm in pronation and the wrist in neutral position without touching any part of their body 11. Each subject performed (alternately with both hands) the test twice using different grip spans in random order, allowing a one-minute rest between the measurements 12. Latin square approach was used to avoid an ordering effect in the randomization of the testing. The used grip spans ranged from 3.5 to 7.0 cm. If the hand span was less than 20 cm, the broadest grip span was deleted; if the hand span was more than 20 cm, the thinnest grip span was deleted. For each hand, the best strength result for each grip span was selected.
DETERMINATION OF OPTIMAL GRIP SPAN
The kind of association relating grip span to hand grip strength was determined to establish the individual optimal grip span for each hand of each individual. The type of association could be linear, logarithmic, potential, quadratic, exponential, or polynomial. All functions were considered in the statistical analyses, and the most relevant was retained. The mathematical function was individually determined through the least-squares fit and graphically represented (Fig. 1).
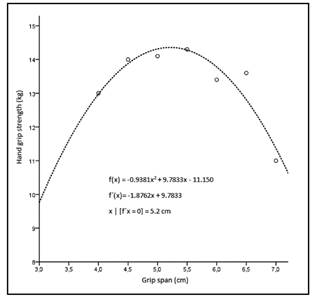
Figure 1 Association relating grip span and hand grip strength for the dominant hand of an adolescent with DS. The maximum of the second-degree polynomial regression equation relating hand grip strength and grip span, f´(x), was the optimal grip span for each hand of each individual.
Once the equation was defined, the optimal grip span was calculated as x|f´(x) = 0, where x corresponds to the optimal grip span (cm), and f´(x) is the handgrip strength (kg). In graphic terms, this corresponds with the maximum of the curves, as seen in figure 1. Only in six cases the association was quadratic (corresponding to a second-degree polynomial equation). For linear associations (n = 11), the optimal grip span was graphically determined. For those adolescents in whom there was no statistically significant association (n = 21 for the dominant hand and n = 17 for the non-dominant hand), the average strength of the chosen grip spans was retained.
DETERMINATION OF THE OPTIMAL GRIP SPAN FOR A GIVEN HAND SPAN
The least-squares approach was used to establish the optimal grip span for a given hand span.
USEFULNESS AND RELIABILITY OF THE OPTIMAL GRIP SPAN
To confirm the usefulness of the optimal grip span when measuring hand grip strength in adolescents with DS, a new group of 15 adolescents with DS (ten boys, five girls) were recruited. The new group of adolescents performed the hand grip strength test at three grip spans using the Latin square design: 1 cm below the optimal grip span, optimal calculated grip span, and 1 cm above the optimal grip span. Each participant performed the test following the same protocol described above. For each hand, the best result at each grip span was retained. To confirm the reliability of measurements of hand grip strength at the optimal grip span, the same participants performed the test at the optimal grip span one hour later. All participants were watching a movie during this time.
STATISTICAL ANALYSES
The hand span, hand grip strength, and the optimal grip span obtained for each hand span by gender was compared with 1-way analysis of variances (ANOVA). Bivariate correlation was performed to evaluate the relationship between optimal grip span and hand span for each hand by gender. In the case of an association, the mathematical function defining the association was calculated through the least-squares fit. ANOVA for repeated measures was used to confirm the usefulness of measuring hand grip strength in three different conditions (optimal grip span, 1 cm below and above). The reliability coefficient of hand grip strength measured at the optimal grip span on two different occasions was compared through 1-way ANOVA for repeated measures, and correlated through parametric bivariate correlation analysis. The SPSS version 19.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. Mean and standard deviations (SD) are given; otherwise, they are stated. The error was fixed at 0.05.
RESULTS
The average hand span was 17.6 ± 1.4 cm for the dominant hand and 17.8 ± 1.5 cm for the non-dominant hand (n = 27). The optimal grip span was not significantly different between dominant and non-dominant hands (all p > 0.05) (Table I). Although no differences were found between hands, the optimal grip span and the span showed higher correlation with the dominant hand (r = 0.660, p < 0.05) than with the non-dominant hand (r = 0.408, p < 0.05), and the subsequent analyses were individually performed for each hand.
Table I Optimal grip span determined in adolescents with Down syndrome (n = 27) for each hand span*

Values are given in mean and standard deviation (SD). *The precision of the hand span measure was 0.5 cm and the value was rounded to the nearest centimetre. †Optimal grip span obtained from the mean of right- and left-hand optimal grip span. ‡Comparison between optimal grip span obtained with right hand versus optimal grip span obtained with left hand for each hand span.
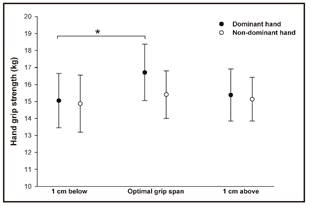
Hand span and optimal grip span showed a significant linear association in the studied adolescents with DS (y = 0.273x + 0.141; r = 0.48, p < 0.05), where x is the hand span (maximal width between first and fifth fingers), and y is the optimal grip span at which the dynamometer should be adjusted before testing. The equation relating grip span as a function of dominant hand span in this group is formulated as y = 0.342x - 1.161 cm (r = 0.63, p < 0.05). In the case of non-dominant hand, the equation is formulated as y = 0,210x + 1.324 cm (r = 0.369, p > 0.05), as seen in figure 2. The optimal grip spans for each hand span calculated from the equations provided are presented in table II. The hand grip strength obtained at the optimal grip span was significantly higher than the strength obtained when the grip was set 1 cm below the optimal grip span for the dominant hand (p < 0.05) (Fig. 3).
The reliability coefficients for the optimal grip were 0.93 and 0.98 for dominant and non-dominant hands respectively. However, the one-way ANOVA for repeated measures showed statistical differences between test and retest (p < 0.05) for non-dominant hand and no differences for dominant hand (p = 0.460). A significant correlation between test and re-test for dominant (r = 0.871, p < 0.01) and non-dominant (r = 0.967, p < 0.01) hands was obtained at the optimal grip span.

Figure 2 Association between optimal grip span and hand span in adolescents with DS (n = 27). Values are means ± standard error of the mean.
Table II Optimal grip span for each hand span calculated from the equations provided*

*For the right hand y = 0.342x - 1.161 cm (r = 0.63, p < 0.05); for the left hand y = 0,210x + 1.324 cm (r = 0.369, p < 0.05); where x is the hand span (maximal width between thumb and little finger, with 0.5-cm precision), and y is the optimal grip span in centimetres. †Optimal grip span obtained from the mean of right- and left-hand optimal grip span.
DISCUSSION
The main finding of the present study is that there is an optimal grip span for the assessment of maximal strength in the dominant hand of adolescents with DS.
As previously recommended by Oppewal et al. 13, for adults with intellectual disabilities, both hands were tested in order to get a valid result of maximal strength.
The results of our study showed that the optimal grip span is more influenced by hand span in the dominant hand in comparison with the non-dominant one, which implies the need of adjusting the grip span of the dynamometer for each hand. For that reason, specific equations for each hand have been developed herein. The level of awareness, attention and their ability to cooperate are factors that make more difficult to measure hand grip strength in adolescents with intellectual disabilities than in those without. At the same time, they may be affecting our results and could explain the discrepancies between both hands. Nonetheless, our findings are in concordance with previous researches in which the optimal grip was influenced by hand span in non-disabled children 5, teenagers 4 and adults 8. Each population has some different physical characteristics; children have smaller hands than teenagers, who in their turn have smaller hands and lower hand grip strength compared with adults. For these reasons, it is possible to think that each specific group may need a specific optimal grip span to assess hand grip strength. This argument can be extrapolated to disabled-population such as adolescents with DS because they have some determined clinical characteristics as smaller hand spans or lower strength levels than those without 14.
The hand grip test has been shown to be a valid tool for measuring muscle strength in persons with some diseases and disabilities 15. This relatively cheap device is associated with many health-related parameters that are especially relevant in a population at risk such as adolescents with DS. On this regard, maximal muscular strength in the dominant arm has been demonstrated to be a good predictor to determine the risk of fracture in adolescents with DS 16. A recent study performed by Izquierdo-Gómez et al. 17 reported information about hand grip strength in adolescents with DS, showing lower hand grip strength compared to those without DS (14.9 vs 26.2 kg). It might be possible that their results were influenced for the use of the ALPHA health-related fitness test battery, which has been established for youth people without disabilities 18. In other populations with intellectual disabilities, similar results were reported by Kern et al. 19, finding that children with an autism spectrum disorder had significantly poorer hand grip strength than control children.
Muscle strength and tone in DS population may play an important role in activities of daily living. Positive improvements in grip strength can be found even after a single exercise session 20. As individuals with premature ageing, sarcopenia appears earlier in life and this is an issue for reduced functional abilities and quality of life for these persons. Several test can be used to measure specific strength, but none of them have been specifically designed for disabled adolescents, neither for those with DS. This study provides key information for therapists or sport scientist on how to better use the hand grip strength test in adolescents with intellectual disabilities.
This study is not exempt of limitations, being the main one the analysis of the sample as a whole, and not by gender. Our limited sample size, due to the intrinsic difficulty on getting a bigger number of participants in this limited age range and with the DS condition made it extremely hard to achieve a larger sample. On the other hand, the rigorous methodology and statistical analyses, together with the validation performed in a sample of 15 participants, ensure the feasibility of the obtained results.
To conclude, the specific grip values stated in this study for dominant hand span are recommended for assessing maximal hand grip strength in adolescents with DS.

