










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Elderly living in nursing homes (NHs) seem to be more vulnerable to specific nutritional deficiencies, since these institutions may have many factors influencing over their alimentation. Namely, the process of institutionalization itself can influence dietary acceptance 1. Besides, the lack of individual nutritional recommendations, the lack of a team specialized in nutritional care and attention, as well as the inadequacy of a physical structure and human resources in many unities of food and nutrition of NHs may render those institutions into a proper environment for food insecurity on the resident population of elderly 2) (3.
The concern with food insecurity in NHs is of importance, considering that the elderly, specially, constitute a population group more vulnerable to nutritional deficiencies of micronutrients by means of several variables, such as morphophysiological changes, presence of chronic diseases and psychosocial influences 4) (5) (6.
Investigations performed aiming to evaluate the ingestion of micronutrients in elderly and, mainly, on those living in NHs are scarce on the scientific literature. Risk of vitamins and minerals deficiencies, such as B vitamins, vitamins C and D and minerals such as calcium, zinc and magnesium, have been reported by few studies involving elderly on Brazilian ILPs 7) (8) (9. Deficiencies of micronutrients are associated with important health problems in elderly, such as the increase of risk for cardiovascular diseases (CVD), more predisposition to weight loss, especially the reduction of muscular mass and strength, and lower tolerance to support chronic or infectious pathological processes 10) (11.
In face of the demographic context characterized by the increasing population aging and the new challenges that are being installed on the field of nutritional research coming from that reality, the need for studies in this area becomes relevant. Thus, the aim of this study was to evaluate the ingestion of micronutrients in elderly living in NHs on the city of Salvador-Bahia, Brazil.
METHODS
This is a cross-sectional study of population base, performed in the city of Salvador-BA, with individuals from both sexes aged 60 or more years and living in public and private NHs, at the urban part of the city.
SAMPLING
The ingestion of micronutrients by 216 institutionalized elderly was evaluated. They were randomly selected from 29 NHs located in ten sanitary districts on the city of Salvador/Ba. In order to perform the intrapersonal variance of consumption and adjustment of nutrients distribution, two dietary measurements were made with an interval of three months between them. The first dietary measurement was made considering all the elderly in the study. For performing the second measurement, the sample was determined considering 40% of the elderly that participated in the initial food intake (n = 216), with a margin of error of 5%. Elderly using enteral, parenteral nutrition and/or specific diet for some medical procedure were not included in the study.
DATA COLLECTION
Food intake data were collected by trainees of nutrition and nutritionist using the total direct food weighing method, with subsequent weighing of the remains. The collection of dietetic measurements was performed considering one day of food intake for each elderly randomly selected to take part in the study. The selected elderly had no previous knowledge about the evaluation. Thus, the collection covered all days of the week (from Monday until Friday) and, mandatorily, one day of the weekend. Food weighing was performed with a portable digital electronic scale Low Range-MBL 2000 BEL, with capacity for 2.0 kg and sensibility of 0.5 grams. Liquids were measured with measuring cylinders of polyethylene with capacities for 500 ml and 100 ml and graduation intervals of 5 ml and 1 ml.
ETHICAL ASPECTS
This project was approved by the Committee of Ethics of the School of Nutrition (CEPNUT) of the Universidade Federal da Bahia, recorded with number 11/2012. After authorization from the NHs by their respective directors or management responsible, the participation of the elderly was voluntary, by signature or fingerprint on the term of informed consent. All data were returned for the institutions by reports and the elderly identified in situations of severe health were forwarded for specialized clinics.
DATA ANALYSIS
Data of individual food intake obtained by the direct food weighing method were calculated with the DietPro version 4.0 software. Foods and preparations which were not in the program were added using nutritional information from the tables of nutritional composition of the aliments, specific for the Brazilian population 12. Without information about those preparations in the tables, standard recipes were used, besides using the labels of the food. Posteriorly, data were added to the program Statistical Package for the Social Science (SPSS), version 16.0 for statistical analyses. In order to estimate the distribution of the usual intake of the elderly and, subsequently, the prevalence of the inadequacy of micronutrients consumption, the software Multiple Source Method (MSM) was used, developed by the European Prospective Investigation Cancer and Nutrition (EPIC), due to its capacity in estimating the usual intake of nutrients, foods and groups of aliments, eliminating the intrapersonal variance of consumption. Besides, this method enables to estimate the usual intake both at the population and individual levels 13) (14. The prevalence of inadequacy of micronutrients was calculated as the percentage of individuals with intake under the estimated average requirement (EAR) value, in other words, with an intake below the estimated average need of the nutrient for each sex, allowing to estimate the percentage of population under risk of adverse health effects 15.
RESULTS
Figure 1 shows the prevalence of inadequacy of micronutrients intake of the elderly (≥ 60 years) living in NHs. High prevalences of inadequate intake of vitamin E (100%), folate (98.6%), pyridoxine (90.7%) and calcium (91.7%) are highlighted. Prevalence of inadequate intake near 80% was observed for ingestion of zinc. The elderly had inadequate ingestion of thiamine, around 66%. Inadequate intakes under 50% were observed for micronutrients selenium, retinol, riboflavin, cyanocobalamin and vitamin C.
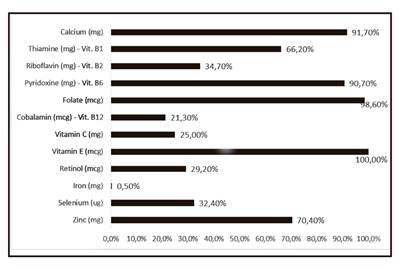
Figure 1 Prevalence of inadequate intake of micronutrients from the general population of elderly living in nursing homes in Salvador, Bahia, Brazil (n = 216).
Data of vitamin and mineral intake for male elderly are expressed in Table I in values of means and percentages. High prevalences of inadequacy (over 90%) were observed for vitamin E, B vitamins such as folate and pyridoxine, as well as for calcium (only of elderly males over 70 years of age).
Table I Means and percentiles of vitamin and mineral intakes in male elderly living in nursing homes in Salvador, Bahia, Brazil
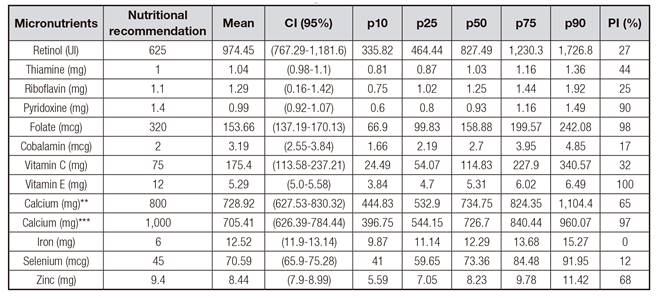
*According to the estimated average requirement (EAR) values, IOM (2000). **Ages reference value 51-70 years. ***Age reference value over 70 years. PI: inadequacy prevalence (%); CI: 95%; n = 59.
Elderly males with ages between 51 and 70 years had prevalence of inadequacy for calcium intake. Prevalences of inadequacy of intake under 50% were observed for micro-nutrients retinol (vitamin A), riboflavin (vitamin B2), vitamin C and cyanocobalamin (vitamin B12).
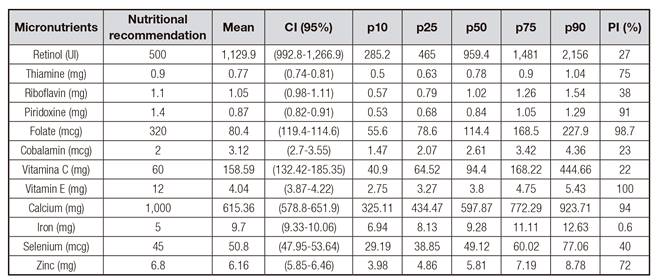
Values of vitamin and mineral intake for the population of female elderly are expressed in Table II. High prevalences of inadequacy were observed, over 90% for vitamin E, folate, pyridoxine and calcium. Prevalences of inadequacy were between 50 and 75% when considering thiamine and zinc. Elderly still have inadequacy of selenium and riboflavin intake, with prevalence values near 50%. It is noteworthy that for nutrients retinal, vitamin C and cyanocobalamin prevalences of inadequacy between 25 and 50% were observed by means of the percentile values.
DISCUSSION
Nutritional deficiencies do not express clinical manifestations during their initial stages, thus individuals may have deficits of nutrient intake without, however, developing immediate manifestation of clinical signs. In this context, early knowledge of the deficits of micronutrients intake may contribute to preventing severe deficiencies.
A positive aspect of this work is the use of two dietary measurements of dietary survey, a criterion that allows to reduce the biases and effects of the variations of individual intake, bringing better results regarding the knowledge of the participants' usual intake. Besides, it is noteworthy that the method of food investigation used in this study, that is, direct food weighing, allows to know more safely the food being consumed by the public being studied. In addition, by means of the direct food weighing method food intake and remains can be recorded and the portion consumed by the individual can be estimated more accurately, thus improving the reliability of the investigation. It is worth considering that direct weighing has been recommended in the validation of other methods of food survey for epidemiological studies 16.
The high prevalence of dietary inadequacy and the risk of micronutrient deficiencies in institutionalized elderly population has been confirmed by some exploratory studies 2) (6) (7. This study showed high results of the prevalence of inadequacy of micronutrients intake, mainly for vitamins E, B6, B9 and for calcium, corroborating the trend found in the literature in other investigations where the ingestion of those, and also of other nutrients, was below the recommendation for age and sex in elderly living in NHs 6) (7) (17. In the study by Fisberg et al. (2013), based on data from the Research of Family Budget (RFB 2008-2009), the prevalence of inadequacy in the diet of non-institutionalized Brazilian elderly was similar to the one found in this study (more than 50% for vitamins A, D and E, calcium, magnesium and pyridoxine) 18.
Berner et al. (2002), evaluating a group of 50 elderly living in one NH, observed ingestion below the recommendation for calcium, magnesium, zinc, copper, vitamins D and E, thiamine, folic acid and vitamin B6 17. Posteriorly, Wendland et al. (2003), who studied another group of elderly living in three NHs, found risk of deficiency for calcium, B vitamins, thiamine, riboflavin and niacin, using the 24-hour recall as the food survey method 2. Another cross-sectional study performed by De Lima et al. (2012) with 55 elderly living in one NH located in Belo Horizonte, Minas Gerais, revealed significantly insufficient ingestion of zinc (82.7%) and niacin (65.4%) 7. There are not many researches performed in a multicenter character; however, the result of a cross-sectional study recently performed by Iuliano et al. (2013) in 18 institutions found inadequate ingestion under the recommendation for calcium, zinc and folate for both sexes, such as the ones observed in our study 19.
Scientific literature, by means of clinical and experimental studies, shows that B vitamins perform important functions regarding energy metabolism, anabolism and cognitive function, being essential for maintaining the health of the elderly 20.
Serum deficiencies of folic acid and cyanocobalamin are proven to be associated with the rise of homocysteine levels, a relevant marker of vascular lesion and predictor of cardiovascular diseases 21) (22. Also, several studies on the elderly have shown the relationship between pyridoxine, folate and cyanocobalamin deficiencies with a high risk of neurodegenerative diseases, with Alzheimer's dementia and depression among them 23) (24) (25.
Several studies have evidenced the low ingestion of calcium on the elderly population and the repercussions of this deficit, which are associated with higher risks of falls and fractures, as well as diseases of inflammatory condition such as osteoporosis and osteopenia, relevant on the elderly population 26) (27. The low consumption of calcium, associated with a low efficiency of its absorption, condition precipitated by achlorhydria, which is common on senile individuals, may contribute to the reduction of the reserves of this mineral, precipitating bone diseases 28. Other metabolic factors are important for maintaining bone health. One of them has stood out during the last years due to its relevance: the normal circulating levels of 1.25 dihydroxy D vitamin, a hormone involved in the proper absorption and metabolism of calcium 29.
Calcium is a micronutrient of special relevance in the elderly, since it also has importance over the activation of cellular proteins, namely, troponin C (which regulates muscular contraction), protein kinase C (acting on the bonding of hormones with cellular proteins), as well as digestive enzymes, required for the digestion of carbohydrates, and lipids (alpha-amylase and lipase), being fundamental for the proper digestion in elderly, a factor already affected by the morphophysiological alterations common to the natural aging 30.
Corroborating the result found in this research, other studies reveal deficits in relation to the intake of antioxidant micronutrients in institutionalized elderly 3) (7) (8) (17) (19. Antioxidant micronutrients, such as vitamins A and C, zinc and selenium, are particularly important since individuals have a physiological condition at senescence characterized by an increase in the production of reactive species of the oxidative metabolism (RSOM), associated with a reduction of the antioxidant defense systems propitiating an environment of oxidative stress 10) (31) (32) (33. This conditions seems to contribute to the occurrence of neurological damage, risk of dementia, depression and chronic diseases associated with aging, among them diabetes mellitus, hypertension, dyslipidemia and atherosclerosis 34.
Thus, in a special way, antioxidants have also been considered as possible mediators of sarcopenia given the catabolic effect that the oxidative stress exerts on the skeletal muscle 35. Few studies are available when the objective is to relate antioxidants consumption and sarcopenia. However, a study conducted by Samba et al. (2007), in a group of non-institutionalized elderly, showed that smaller plasma concentrations of carotenoids and vitamin E were associated with less force on hips and knees 11. Similarly, a cross-sectional study of more than 1,000 residents in the elderly community identified that the serum concentration of serum magnesium was significantly associated with improvement rates of muscle strength 36. In addition, another study aimed to verify the association between ingestion of micronutrients and muscle strength showed that nutrients with selenium, beta-carotene and vitamin C were positively associated with handgrip strength 37.
In this context, it is highlighted that other nutrients such as iron, magnesium, phosphorus and zinc are directly associated in the multifactorial dynamic of muscle anabolism, either by directly participating in the formation of muscle mass, or by contributing to the normal activity of anabolic hormones, ensuring muscle health 38) (39) (40.
It is worth to consider that this study has methodological characteristics that must be weighted. The method of analyzing the adequacy of micronutrients intake uses EAR, model based on the average need of nutrient estimated for populations. Besides, the lack of food composition tables estimating the intake of micronutrients such as magnesium and of microelements such as copper, chromium, manganese, boron, molybdenum and vanadium may mask more specific and equally important nutritional deficiencies, considering that such nutrients are fundamental on the homeostatic regulation.
CONCLUSION
In face of the information exposed, the conclusion is that there is a high prevalence of inadequacy regarding vitamin E, folate, pyridoxine and calcium intake in elderly population living in nursing homes. This emphasizes the importance of new studies with this population, considering that elderly, especially, are a group more vulnerable to nutritional deficiencies of micronutrients, by means of several variables, such as morphophysiological changes (on the processes of mastication, swallowing, digestion, absorption and utilization of nutrients), presence of chronic diseases and influences of social, psychological and emotional character.
Providing the adequate food intake for the elderly in NHs may contribute to ensure that those institutions may warrant quality of life as well as food and nutrition security for those elderly.

