










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Good nutritional status is highly relevant for children with cancer. It enables them to cope better with the intensive cancer treatment regimens 1. The prognosis for childhood cancer has improved in recent decades, with five year survival rates reaching approximately 80% 2. Nonetheless, this improvement in the survival rate in childhood cancer has given rise to a number of treatment-related complications 3. Malnutrition in children with cancer is a significant risk factor for negative outcomes, such as decreased treatment tolerance, increased susceptibility to infections and reduced survival 4. This may occur because the energy intake is diminished, because the energy requirement is increased, or both. Inflammation and alterations in neurotransmitters and neuropeptides 4) (5) (6 are relevant factors for malnutrition. However, in the clinical practice setting, it is difficult to pinpoint which factors operate to cause substantial weight loss and malnutrition in a given patient.
Cancer anorexia-cachexia syndrome is multifactorial in origin. Its etiology is gradually being defined. This syndrome is related to malnutrition. Appetite-related hormones 7, like ghrelin and leptin, are among the possible mediators. Ghrelin is a peptide hormone with a potent orexigenic effect, directly related to food intake, and is mainly produced in the stomach 8. Leptin, an adipocyte-derived protein, was identified as a product of the obesity gene (whose autosomal recessive mutation results in profound hyperphagia and obesity) 9). Both hormones are related to the regulation of food intake and, consequently, body weight control, and can play an important role in the occurrence of obesity and metabolic syndrome in healthy children and adults 3) (7. Increased ghrelin levels and decreased leptin levels were reported in patients with a variety of cancers 10) (11, and were reported in adult cachectic patients compared with non-cachectic cancer patients 12. However, only very few studies have examined the role of these hormones, or other adipocytokines, in pediatric patients with cancer to date.
Chemotherapeutic agents, in the long term, can also result in changes in leptin secretion, leading to increased plasma levels 13. However, the plasma levels of leptin vary substantially in the available studies on childhood cancer. In the study of Park et al. 14, children with pediatric cancer showed higher plasma concentrations of leptin when compared to healthy children, but lower plasma levels of ghrelin. Moschovi et al. 15 followed nine pediatric ALL patients from the diagnosis to the maintenance phase, and no significant decreases in leptin levels were observed in these patients. In another study, the same authors observed an expressive increase in the levels of ghrelin after the eighth cycle of chemotherapy 16. However, very few studies evaluated alterations of ghrelin and leptin during chemotherapy in different types of cancer, and these discrepant results may be due to the different treatments adopted. Thus, the purpose of this study was to systematically review possible changes in the levels of appetite hormones, specially leptin and ghrelin, in pediatric patients with cancer.
METHODS
SEARCH STRATEGY
We systematically reviewed the literature using a protocol suggested by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines to search research databases, screened published studies, applied inclusion and exclusion criteria and selected relevant literature for review 14. An extensive electronic search was carried out in December 2016 to identify the relevant articles. The following databases were used: PubMed, Lilacs and Scielo, as well as manual bibliographical reference search of the studies. According to the Medical Subject Headings of the National Library of Medicine (MeSH), "childhood cancer", "ghrelin" and "leptin" were used as descriptors.
INCLUSION/EXCLUSION CRITERIA
Studies (prospective and cross-sectional) with ghrelin and leptin as outcome during follow-up treatment of children and adolescents (age below 20 years) with any type of cancer were included. To be included in this review, articles also had to be peer-reviewed full report, and published either in English or in Portuguese. Book chapters, reviews, letters, abstracts or dissertations, or any clinical trial with an experimental treatment for childhood cancer were excluded.
STUDY SELECTION AND DATA EXTRACTION
We used a spreadsheet to manage screening and selection of studies. Two reviewers (APTF and ADLB) completed an initial, independent screening of all titles and abstracts retrieved from the database searches, and independently reviewed the full texts of the studies. A third reviewer (RF) resolved any conflicts at both stages. In an effort to prevent the false exclusion of a relevant study, among any conflicted decisions in which the third reviewer moved to exclude the study, all three reviewers discussed the article and came to a consensus. Methodological quality was not an inclusion criterion.
Furthermore, reported limitations or limitations found during reading were abstracted.
RESULTS
Initially, 76 articles were identified. After removing duplicate articles (03) and reading their title names and abstracts, a total of 23 articles were selected to be read in full. After careful reading, ten articles were excluded of final analyses and two articles were included. A flowchart showing the details of the selection process is shown in Figure 1. In the end, 15 studies were included in this systematic review. Table I shows the result of the systematic review.

CHARACTERISTICS OF THE POPULATION INCLUDED IN THE STUDIES
A total of 863 patients were evaluated, ages ranging from 0 to 21 years. Most of the studies reported on children and adolescents with ALL 3) (16),(18),(20) (21) (22) (23),(26) (27) (28) (29, with non-Hodgkin's lymphoma 20) (25) (27 being the second most prevalent. The studies included a population of both genders, and many of them had completed their treatment and were considered as cancer survivors. Four studies 16) (19) (21) (28 followed the patients up, including measures before and after treatment.
HORMONE CONCENTRATIONS IN CASE-CONTROL STUDIES
Most studies analyzed leptin levels; only two studies 16) (19 evaluated levels of ghrelin. In one of these studies 16, children with cancer had lower ghrelin concentrations when compared to their controls, but this concentration increased significantly after the maintenance phase of chemotherapy. The studies showed discrepant results in relation to leptin levels when compared to controls. While one study showed that leptin levels were higher in the cancer group 26, others showed that the levels were significantly lower in patients with pediatric cancer 20) (27, while still others found no difference between the groups 21) (24) (25.
HORMONE CONCENTRATIONS DURING TREATMENT OR BETWEEN DIFFERENT CONDITIONS OF CÁNCER
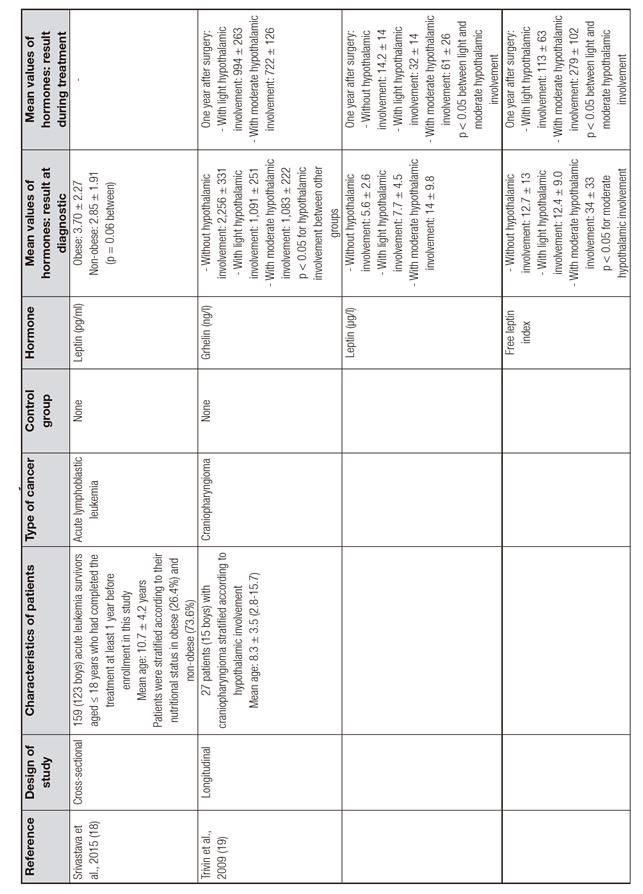
The studies showed a wide variation in the health conditions of patients, and some studies compared the hormonal levels in different cancer treatment regimens. Srivastava et al. found that leptin levels were slightly higher in obese children with cancer 18, and Kojima et al. found that patients with metabolic syndrome had higher concentrations of leptin 3. As to the impact of treatment on hormonal concentrations, Trivin et al. found that patients with craniopharyngioma and hypothalamic involvement had lower concentrations of ghrelin and higher concentrations of leptin 19. In this same study, after one year of the surgical procedure, ghrelin levels were significantly reduced only in patients with moderate hypothalamic involvement, while leptin levels increased independently of hypothalamic involvement. Treatment with high doses of methylprednisolone during seven days significantly increased leptin levels in patients with leukemia 21, but another study demonstrated a reduction in leptin levels at day 33 of chemotherapy 28.
DISCUSSION
This review confirms that there is a large discrepancy between studies in relation to the concentrations of these hormones in cancer patients compared to controls, and between different treatment protocols. Many studies evaluated hormones in cancer survivors, not necessarily with active disease, and this may have contributed to the variety of findings. Survival rates after childhood cancer have improved markedly, and, today, more than 80% of patients with a pediatric malignancy will become five-year survivors 30. With the improved survival rates, long-term treatment-related effects are being observed more frequently, and need to be addressed. Obesity is one such late effect, which increases the long-term risk of death from cardiovascular diseases. This condition likely has a significant association with appetite hormones.
An interesting aspect of the studies included in this systematic review is that very few studies have evaluated ghrelin. Ghrelin is a key regulator of nutrient sensing, meal initiation, and appetite 31. Additionally, studies have reported that ghrelin exhibits proliferative properties in cancer 32. Interestingly, the articles that included the evaluation of this hormone dosed total ghrelin, not its fractions (acylated and non-acylated). There is a debate about the usefulness of total ghrelin as a biomarker of appetite. For some authors, total ghrelin measurements do not accurately reflect specific biological actions of ghrelin. Ghrelin circulates in both acylated and unacylated forms; the unacylated form's levels are 2.5 times higher than the acylated form's 33. It is felt that acylation at serine-3 is essential for the biological activity of ghrelin. However, unacylated ghrelin is able to antagonize the metabolic but not the neuroendocrine response elicited by acylated ghrelin 34. More information on the relationships of acylated and unacylated ghrelin in patients with cancer is called for.
Of the studies included in the systematic review, only two evaluated ghrelin concentrations in the pediatric population with cancer 16) (19, and both measured total ghrelin. Levels of ghrelin in children with ALL were lower than in controls, and in the maintenance phase of chemotherapy there was a significant increase in the circulating levels of the hormone 16. In acute leukemia, there is inflammation and serum hyperlipidemia, and both may suppress ghrelin at diagnosis 35. Leukemia causes a more intensive inflammatory process than solid tumors; so, gut hormones may behave differently in ALL. Trivin et al. 19 observed that the hypothalamic involvement in patients with craniopharyngioma decreased levels of ghrelin, and this reduction was more significant the greater was the involvement. In the particular setting of craniopharyngioma, the destruction, or functional impairment, of the hypothalamus is probably responsible for the failure to integrate neuronal, hormonal and metabolic signals from the body, leading to changed feeding behavior 36.
Leptin is proportional to total body fat mass and, communicating primarily with the hypothalamus, has a role in satiety and energy use 18. Recently, leptin has been shown to play a regulatory role for differentiation within the myeloid and erythroid cell lineage, whereas results of its regulatory effects on lymphocytes and related tumor cells have been contradictory 28. Higher serum leptin levels have been associated with body fatness in ALL survivors 37. In the current systematic review, the results in leptin concentrations were quite discrepant between studies. This may be due, in part, to the fact that leptin levels are affected by several variables, including gender, pubertal stage, weight, diet and the analytical method 38. Small variations are expected in the values assayed by different methodology. Large variability is probably due to different pubertal stages and BMIs in the studies 39) (40.
Most of the studies included in the review evaluated children and adolescents with ALL or survivors of hematological malignancies. Leukemia is the most common malignancy in children 9) (41. It is a heterogeneous group of diseases in which there is a substitution of normal medullary and blood elements by immature cells (blasts), and accumulation of these cells in other tissues 42. Because more than 80% of children with ALL survive to adulthood, the late effects of therapy must be considered 23) (43. In survivors, overnutrition may be one of the risk factors for type II diabetes mellitus, hypertension, and cardiovascular disease. This is a particular problem for cancer survivors, who already have the additional risk for cardiovascular disease due to potential cardiotoxic effects of chemotherapy or radiotherapy 44. The role of leptin in hematological malignancies has been explored, not just as an appetite hormone, but also as a stimulus for proinflammatory cytokines, hematopoiesis and lymphopoiesis 25, promoting atherogenesis. It may indeed be an independent risk factor for cardiovascular disease.
According to Srivastava et al. 18), leptin is proportional to total body fat mass and communicates primarily with the hypothalamus, promoting satiety and influencing energy usage. However, studies have failed to find a direct relationship between leptin levels and anthropometric parameters of body fat 45) (46. Petridou et al. have shown that elevated serum adiponectin, but not leptin levels, might be independently associated with both Hodgkin's and non-Hodgkin's lymphoma incidence, as well as with poor prognosis, in children 24) (25. In young adult survivors of childhood cancer, adiponectin might be associated with insulin resistance 47. The differences between studies do not allow us to characterize leptin changes in children with cancer in this review. More studies are needed to investigate the role and associations of appetite hormones in children and adolescents with cancer, in order to better understand the pathophysiology of nutritional findings, and even to establish different patterns of response in different types of cancer.
In conclusion, changes in the responses of the ghrelin and leptin hormones in children and adolescents with cancer are quite diverse, probably due to the different types of cancer observed, different treatments performed and biological characteristics of this age group. Because of growing interest in the effectiveness of strategies to minimize cardiometabolic risk in the childhood cancer population, further research is necessary to better understand the behavior of these hormones during the disease and its possible relations with the nutritional status and the prognosis of the patients.

