










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The field of home enteral nutrition (HEN) has undergone a huge development in recent decades, leading to a reduction in the frequency of malnutrition and its serious consequences. Health care at home provides medical services in a more comfortable and familiar environment.
Despite the growing importance of HEN, there is still a notable lack of information about its epidemiology and characteristics, which can be explained both by the absence of obligatory registries and the large differences among HEN organizations in different countries or regions.
Obligatory records would offer valuable information about HEN frequency and characteristics, including the most frequent indications, complications and outcomes of patients. Also, registries could help estimate the consumption of resources needed by this therapy and its impact on the health system. However, HEN records are rare and often voluntary, which limits the reliability of their data. In 2009, a systematic review found only eleven home artificial nutrition (HAN) records published between 1987 and 2007 (60% home enteral nutrition and 40% home parenteral nutrition) in eight different countries (Australia, Germany, Italy, Japan, Spain, Sweden, the UK and the US). They all had limitations and heterogeneity in data collection, making it difficult to obtain representative information 1.
In Spain, the HAN group of the Spanish Society of Parenteral and Enteral Nutrition (NADYA-SENPE) has conducted an annual record since 1994. Although useful, it is a voluntary record and it offers only a limited view of the magnitude of HAN in our country 2,3,4,5,6,7,8,9,10,11,12,13,14.
The uncertainty about HAN, especially in the home enteral nutrition (HEN) area, can also be explained by the lack of definition of common criteria. Thus, in some countries it includes only those therapies administered by tubes or ostomies, while other countries consider oral treatments too when a certain amount of calories is exceeded 15,16. This fact makes comparison between records from different countries almost impossible.
The time limitation in which professionals can include data has forced the records to focus on collecting information about those patients who cover more than 75% of their requirements with HEN, thereby creating an underestimation of the actual frequency of HEN. In the UK the number of patients in recent records has dropped due to the lack of time available to dietitians to enter data and the problem of obtaining patients' written consent 17. All these difficulties account for the main motivation of this study.
OBJECTIVE
The aims of this study were to assess the status of HEN in our area, with regard to its incidence and characteristics; to weigh the importance of HEN as a therapy; and to detect fields in need of improvement in our practice. We hypothesized that voluntary registries underestimate the real frequency of HEN, and we hope to offer a more realistic vision of HEN that includes all patients regardless of the administration route or the percentage of calories provided.
METHODS
This is a prospective, observational, two-year study performed at the Complejo Hospitalario Universitario of Santiago de Compostela (CHUS), a tertiary university hospital in Galicia (Spain).
In Spain, HEN is financed by our public health system. However, HEN organization exhibits important organizational differences between autonomous communities. In our region, nutrition units are the main prescribers of HEN, although other specialist physicians may be prescribers as well. Regarding the dispensing of HEN products, in most communities this takes place in the pharmacy offices, but in Galicia it is carried out through hospital pharmacies. This peculiarity has allowed us to better control patients with HEN and has enabled us to obtain a more accurate estimate of the incidences.
INCLUSION AND EXCLUSION CRITERIA
All the patients who started HEN in the period from October 15, 2009 to October 14, 2010 at the CHUS were included in the incidence study, regardless of the type of nutrition or prescriber department.
For the descriptive study of the characteristics and the evolution of HEN, those treatments prescribed and monitored by other hospital services were excluded because of the difficulties in proper data collection.
INCIDENCE OF HEN
All new HEN prescriptions during the study period were included, regardless of the type of artificial nutrition (enteral nutrition by tube or ostomy, oral supplements, thickeners or protein modules). To avoid loss of patients, the HEN dispensing registries of the Hospital Pharmacy Department were reviewed.
Therefore, the incidence of HEN in our health area was calculated as the ratio between the patients who started HEN in the study period (both prescribed by a Nutrition Unit and by other hospital departments) and the total adult population of the area (aged > 14 years), according to the last report of our regional healthcare service (SERGAS) 18.
DESCRIPTIVE STUDY OF HEN PATIENTS AND CHARACTERISTICS
Baseline variables
At the first visit, epidemiological data, medical history, functional status and percentage of patients in nursing homes were registered. Regular home medication was also collected, with a focus on drugs that may interfere with nutritional status.
Nutritional screening tests were initially carried out, including the Malnutrition Universal Screening Tool (MUST) and the Mini Nutritional Assessment (MNA) (only in patients aged ≥ 65 years), in order to assess the risk of malnutrition. Then, a complete nutritional assessment with anthropometry (weight, height, body mass index, percentage of weight loss and tricipital skinfold) and laboratory tests (levels of albumin, prealbumin, transferrin and protein bound to retinol [PBR]) was performed. Both the nutritional screening tests and the complete evaluation were performed by the Nutrition Unit staff when the patient's situation permitted it. Patients were weighed standing barefoot on a Seca 220(r) mechanical scale with a precision of 0.1 kg. Height was measured with a measuring rod (Seca 220(r)) with a precision of 0.1 cm. A John Bull(r) skinfold caliper was used to determine tricipital skinfold.
Nutritional classification of patients followed the Spanish Society of Enteral and Parenteral Nutrition (SENPE) and Spanish Society of Medical Documentation (SEDOM) definitions 19.
The indication, type, administration route and calories provided by HEN were also described. When HEN provided less than 1,000 kcal/day, it was considered as supplementary nutrition. When it provided ≥ 1,000 kcal/day, it was defined as complete nutrition.
Follow-up variables
The patients were followed until October 15, 2011, to evaluate their evolution and modifications in nutritional support. During routine patient visits, changes in clinical and functional status, medication and HEN were recorded. The appearance of complications (gastrointestinal, mechanical, metabolic and infectious complications) with nutritional support (both patient-reported and those registered in the electronic medical history), the episodes of attendance at the Emergency Service and hospitalizations related to HEN were also registered.
At the end of the follow-up period, a final assessment of nutritional status was conducted, and duration of nutrition was calculated. In cases where HEN had been suspended, the cause of treatment discontinuation was investigated by contacting patients, with special interest in recording cases of death.
STATISTICAL ANALYSIS
Statistical analysis was performed using SPSS 19.0 (SPSS Inc., Chicago, IL, USA). The normal distribution of quantitative variables was examined by the Kolmogorov-Smirnov test. Variables matching normal distribution were presented in terms of mean and standard deviation (SD), and those without normal distribution were presented in terms of median and interquartile range (IQR). Quantitative variables with normal distribution were compared using the Student's t test. Quantitative variables without normal distribution were compared using the Mann-Whitney and Wilcoxon tests for independent or related samples, respectively. Categorical variables were expressed as percentages and compared to the Chi-squared test. A p value lower than 0.05 was considered as statistically significant.
RESULTS
INCIDENCE OF HEN
During the study period, 788 new patients started home enteral support in our health area (85% of them monitored by the Nutrition Unit). The reference population was the 342,694 adult patients in the area 18.
The incidence of HEN in this sanitary area resulted in 229 cases/100,000 inhabitants/year, regardless of the type of HEN and the prescriber department.
BASELINE CHARACTERISTICS OF PATIENTS
Only 573 of the 788 incidents of HEN patients were finally included in the descriptive study. The main reason for exclusion was the lack of prospective data among patients whose HEN treatment was prescribed and monitored by other hospital services. Also, patients who were not registered in the recruitment period were excluded, although HEN was prescribed in the Nutrition Unit (Fig. 1).

Of the 573 patients included in the registry, 59.7% were women. The median age was 79 (IQR 87) years, with 78.6% of patients over 65 years. The distribution of patients by age was represented in Figure 2.

We found high levels of comorbidity (Table I). The median number of home treatments was six (IQR 19) drugs, and 35.9% of patients reported taking medications associated with nutritional risk, especially corticosteroids, anti-Parkinson drugs or digoxin.
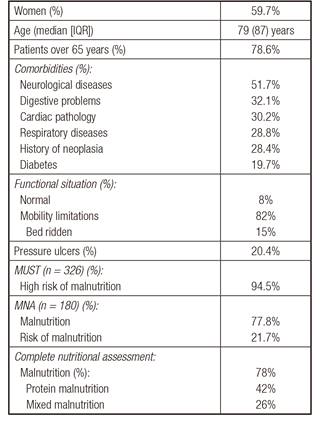
About 80% of the patients reported mobility limitations, with 15% of patients being bed-ridden and 20.4% experiencing pressure ulcers. A total of 60.3% needed a home caregiver, and 19.7% were living in nursing homes.
Nutritional screening with MUST was performed in 326 patients, in which it was found that 94.5% were at high-risk of malnutrition. MNA was carried out in 180 of 447 patients older than 65 years with available data, and the percentages of malnutrition or risk of malnutrition were 77.8% and 21.7%, respectively. At baseline, the complete nutritional assessment showed that 78% of the patients were malnourished, mainly with protein or mixed malnutrition (42% and 26%, respectively).
HEN INDICATIONS AND CHARACTERISTICS AT FIRST VISIT
Neurological and oncological diseases, which are the most common indications of HEN, accounted for almost 50% of indications in the registry. In 35% of cases, HEN was prescribed due to a neurodegenerative or neurovascular disease that affects swallowing or intestinal motility. Mechanical disorders, especially those caused by head and neck cancer or surgery, represented 11.9% of HEN indications. The remaining cases were malnourished patients who received short periods of HEN after hospitalization or after a hip fracture.
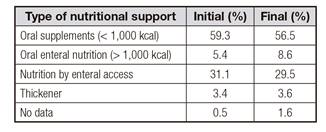
The oral route was the most used (69.2%), followed by enteral administration by tube (25.1%). Only 29 patients (5%) had a gastrostomy at the first visit. Among patients with HAN by enteral access, bolus by gravity was the most common form of administration (95.9%). Continuous infusion pumps were used in six cases and bolus administration by syringe was used in one case.
The type of nutritional support is summarized in Table II.
High-calorie and standard (normoproteic and isocaloric) diets were the most reported in the present study (32.5% and 32.1%, respectively), while high-protein and special formulas accounted for a third of the total prescriptions.
With regard to energy intake, 38.8% of patients received more than 1,000 kcal/day, and their median intake was 1,500 (IQR 1,560) kcal/day. The remaining 61.2% of patients received less than 1,000 kcal/day, with a median intake of 600 (IQR 827) kcal/day.
EVOLUTION OF PATIENTS
Of the 573 patients initially enrolled in the study, 304 patients only had a first visit. Therefore, follow-up data were available in 269 patients. In this group, gender and age distribution were similar to baseline. The median duration of HEN was 8.5 (IQR 22.2) months and was slightly higher in patients with enteral nutrition (by tube or ostomy) than in those with oral nutrition (10.6 versus 8.7 months; p = 0.010). The type of HEN at the end of the study period is summarized in Table II. Oral route of administration was still the most common (70%). Enteral access by nasogastric tube accounted for 18%, gastrostomy accounted for 12% and one patient had a jejunostomy.
Regarding the nutritional evolution of the patients, we found that 75% maintained or increased their weight during follow-up, with a mean weight gain of 1.6% (mean initial weight 60.1 [SD 13.3] kg vs final weight 61.1 [SD 11.7] kg; p = 0.008). The percentage of patients with normal or overweight rose from 74% to 82.7% (p = 0.001) at the end of the study. In the elderly, nearly half had a normal MNA result and the remaining were predominantly at risk but had not established malnutrition. The complete nutritional evaluation obtained an increase in the group of patients with normal assessment, from 23.2% to 67.2%, although this difference did not reach statistical significance.
In the subgroup of patients with follow-up, a significant reduction in the percentage of pressure ulcers was observed (15.7% at baseline vs 10.3% at final visit, p < 0.001). However, no changes in patients' functional status were detected.
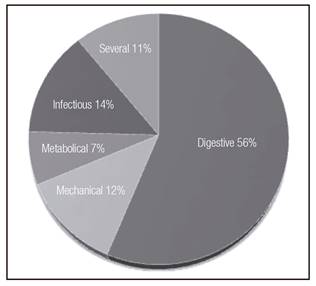
During the study period, the 74.7% of followed-up patients did not experience any complication associated with HEN. A total of 64 patients reported 105 episodes of HEN complications, mostly mild digestive problems (Fig. 3). In addition, 104 hospitalizations in 68 patients were registered (16 bronchial aspirations, seven admissions for placement gastrostomy and one admission for refeeding in a patient with eating disorders). The index of hospitalizations related to HEN was 0.083 episodes/patient/year.
At the end of the study period, home nutritional support was active in 24.4% of the 573 patients included at baseline (mainly patients with underlying neurological diseases: 46.2%); the rest had already discontinued it. Discontinuation of treatment was due to patients' death in 56.8% cases, to clinical improvement in 32.5%, to loss of follow up in 5.7% and to transfer to another health area in 3.6%.
At the end of the study, the percentage of deaths was 43.1% (247/573), including those 246 patients who had maintained HEN until death, and one patient who had previously been lost to follow-up but who had also died at the end of the study.
DISCUSSION
This paper presents the results of a systematic HEN registry, which has allowed us to calculate the actual incidence of home enteral nutritional support in our health area, including all forms of HEN, regardless of caloric intake or route of administration.
The first epidemiological data about HEN in Europe date from the late 90s, when a survey conducted in eight European countries (Belgium, Denmark, Spain, France, Italy, Poland and the UK) found a mean incidence of HEN of 163 cases/million inhabitants/year 20. However, it also highlighted the existing disparities among the countries surveyed and the big difference with the prevalence reported in the US, about ten times higher (up to 1,660 cases/million in Medicare beneficiaries, or 415 cases/million in the general population) 21,22.
Comparing our epidemiological data with international registries, we found a frequency of HEN that was clearly higher than those described in Europe and the US, but closer to the Medicare population data. This could be explained because the Medicare population includes mainly people ≥ 65 years or disabled, and HEN funding in Medicare is more similar to our public health system 20,21,22.
In an Italian study in Treviso, with a similar size population to ours, only 655 patients were included in the HEN registry over a period of five years, resulting in an incidence 6.9 times lower than that obtained in our study 23. These marked differences may be due to exclusion in the register of patients with oral nutritional support.
In Spain, the last NADYA record reported a much lower prevalence (80.58 to 90.51 cases/million inhabitants) 14, and studies in other Spanish regions also showed a lower frequency of HEN than ours. However, in recent years a clear increase in HEN incidence and prevalence has been observed, especially in oral nutritional support 24,25. Thus, the prevalence of HEN described in a previous study of our region was 1,034 cases/million, which is in line with the results obtained in our area a decade later 26.
CHARACTERISTICS OF REGISTRY POPULATION
The characteristics of HEN patients in terms of age, functional status or condition clearly depend on the characteristics of the registries and the definition of HEN used, which favors heterogeneity, making comparison between records a real challenge.
Our study found a marked aging that was not present in other registries, such as the US record, with an average age that was 15 to 20 years lower (between 61 and 65 years) 22. In other European studies, the percentage of HEN patients older than 65 years was slightly above 50%, while our data was close to 80% 20. However, the last Spanish NADYA record described a HEN population with a median age somewhat higher (73 years) 14, and the Treviso (Italy) registry population appeared to be most similar to ours, with an average age of 77.4 years and a percentage of patients over 65 years of 81.3% 23.
In Europe, neurological diseases are the most common pathologies reported in HEN registries, accounting for 45 to 50% of the total indications. They are followed by malignant tumors, especially head and neck cancer and esophageal tumors (25 to 35%) 17,20. Spanish records data exhibit similar results (60.5% neurological indication, followed by neck and head tumors) 14. By contrast, in US HEN registries, the proportion is reversed, involving 60% cancer patients and 40% neurological patients 22. The peculiarities of the records are probably what explain these disparities. For example, the latest data from the UK showed a downward trend in the percentage of neurological patients, probably as a result of the decrease in indications of nutritional support in patients with advanced dementia 17. In our population, the inclusion of all types of home nutritional support, including thickeners, modules and supplements, likely explains the different pathology distribution found. Neurological diseases and cancer accounted for only half of the indications. The rest were predominantly cases in which patients received perioperative nutrition after a hip fracture or cases of malnourished or at risk of malnutrition patients, including elderly people who did not meet their requirements with a traditional diet, mainly after hospitalization. In Spain, the latter two indications are not reimbursed by the national health system, but both have been included in our clinical practice following the recommendations of the guidelines of the European Society of Parenteral and Enteral Nutrition (ESPEN) Geriatrics (grade of recommendation A) 27.
NUTRITION THERAPY FEATURES
The route of administration of nutritional support is very influenced by the characteristics of the registry. Due to this fact, it is understandable that our results, with a clear predominance of the oral route and only 30% of patients undergoing other enteral accesses, differ from those data recorded in traditional voluntary HEN registries. Thus, the British record directly excludes oral nutrition, reporting just tube feeding/ostomy patients (75% and 17.5%, respectively) 17,28. In the US, only treatments expected to last more than three months are financed, thereby explaining the high prevalence of gastrostomies (550/million population in 1998) 22). Also, in other European countries, the frequency of percutaneous endoscopic gastrostomies (PEG) is high (about 58.2% of patients with HEN), followed by NGT (29.3%) 20. The Spanish NADYA registry takes into account only patients with ≥ 900 kcal/day, thus excluding most patients with oral supplements 11. In the last Spanish record published, the NGT rate represented approximately 50% of the cases, and gastrostomies accounted for 42% 14. However, the authors have warned about the limited usefulness of the registry for evaluating nutrition routes, because this data is not available in many patients. In addition, the apparent decline in the oral route (64% in 2007 vs 10% in 2010) seems to reflect a tendency to include only cases of HEN by NGT/ostomy due to work overload and limited time in clinical practice.
NUTRITIONAL EVOLUTION
At baseline, our study population showed a high percentage of malnutrition (over 75%), especially protein or mixed malnutrition. It was probably related to the patients' profiles, which mostly included acute diseases or acute exacerbations of chronic diseases. This would explain the impact on protein reduction and even the frequency of pressure ulcers (present in one out of every five patients), although other studies have found an even higher prevalence 23.
Nutritional support can improve patients' nutritional status regardless of their underlying pathology. In particular, oral supplementation, which is the most common HEN subtype in our study, is recommended, with a high degree of evidence, for elderly malnourished people, people who are at risk and the frail elderly. However, while some studies have found improvement in various nutritional parameters, even with small volumes of supplements 29,30,31,32,33,34, others have failed to demonstrate this nutritional improvement. The stage of disease at which treatment is started seems also to be a determining factor in the effect of HEN 35,36,37.
In our area, a small weight gain was achieved in HEN patients (+ 1.6%), which is slightly lower than that described by a review of studies performed in elderly patients with oral supplementation (around 2.2%) 29. However, it was enough to maintain or increase their initial weight in 75% of patients. The distribution of BMI, the nutritional assessment and the presence of pressure ulcers also experienced a marked improvement during follow-up.
TREATMENT EVOLUTION
Despite the spread of artificial nutrition, not many HEN registries detail the development of complications. In 2003, the NADYA-SENPE Spanish group published a specific study with a rate of complications/patient/year of 0.16, with gastrointestinal (62.5%) and mechanical complications (33.2%) predominating 38. These data are consistent with those published in a Galician (Spain) study (0.18 complications/patient/year, especially digestive and infectious complications) 26 and also with those of our study, except for a lower percentage of mechanical complications, which is expected because most of our patients were receiving oral HEN. Most episodes were mild and were frequently resolved by the patient or their caregiver or by contacting the Nutrition Unit, without treatment interruption. However, the use of enteral access by NGT/ostomy may involve mechanical complications, requiring further consultation to solve them 39. Therefore, HEN appears to be a safe therapy, with a low risk rate of complications and an index of hospitalizations that is lower than other records (0.083 episodes/patient/year vs 0.3 to 0.4 episodes/patient/year complications in our study vs US records, respectively) 22.
FINAL SITUATION
HEN duration is one aspect that depends on the age and conditions of the patients included in the registry. In our area, at the end of the study period, only 24.4% of patients continued with active HEN. Most of these had neurological diseases and little chance of recovery. These results are similar to the US registry results, with 25% neurological patients and 6% oncological patients with active HEN 22.
As in the US and Canadian records 40, in our population the high percentage of short treatments and patients with a single visit was remarkable (53%). This reflects the high mortality rate found in HEN patients but also the high rate of patients with temporal indication of nutrition, which is suspended after patient amelioration (e.g., postoperative supplementation after hip fracture). As in other records, the most important causes of suspension were death or clinical improvement 10,11,12,13,14.
LIMITATIONS AND STRENGTHS
We have to point out as a limitation that our data represent the particular situation of HEN in our area, and they may not be extrapolated to other populations. Although we could only include in the analysis patients who had been prescribed HEN by the Nutrition Unit (due to lack of prospective data from the group in which HEN was prescribed by other hospital departments), we consider that our sample is representative of the HEN situation in our media, including more than 70% of the incident population.
As strength, this registry has shown the real situation of HEN in the health area of Santiago de Compostela, allowing us to obtain an accurate incidence estimate (including all prescriptions) and offering a realistic view of the HEN, not available in other voluntary registries.
In conclusion, HEN incidence in our area is clearly superior to that described in other epidemiological studies. The characteristics of both patients and nutrition differ from those reported in voluntary records (which usually include only certain subgroups of patients). This shows the existence of an aging and multi-pathological population that requires HEN, mainly in the form of oral supplements, during short periods until the resolution of the situation that motivates the nutrition indication.

