










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Ever since it was introduced as an Olympic sport in Seoul, Korea, in 1988, competitive table tennis has grown in status at national and international levels and it is now played by more than 40 million people worldwide 1. Table tennis belongs to the racket sports group, as does badminton, squash, and tennis. It is characterized by continuous changes of rhythm and intensity, with repeated fast actions of short duration. It involves intermittent periods of explosive and high-intensity muscle activity, requiring significant energy from both the anaerobic alactic and aerobic energy systems 1.
Nutrition is considered to be an essential factor for success in sports, as it may affect a player's ability to train, play and recover from exercise 2. Athletes should consume diets that provide adequate amounts of nutrients, by consuming a variety of foods and the recommended number of servings, as specified in the food guide pyramids 2. Adolescents that participate in sports competitions deserve even more attention, due to the psychological and physiological stress to which they are exposed. Thus, additional care should be given to their diet, since the extra needs of their physical activities are additional to their nutritional needs for growth and development 3.
Previous studies have indicated that many athletes have sub-optimal dietary intakes 4,5. This might be related to their low levels of nutritional knowledge and the use of low quality nutritional information sources 4,5. It has also been argued that cultural backgrounds, taste preferences, together with appetite and cooking skills, may inhibit the implementation of appropriate dietary strategies by the athletes themselves 6. However, such food behavior might be differently influenced according to age. During adolescence, dietary habits are highly dependent on the food behavior of their parents 3, while in adulthood, despite having higher educational levels and greater health awareness, many athletes have difficulties in adapting to a healthier diet, due to the lack of time for meal preparation 7.
An evaluation of an athlete's dietary intake may help to understand the principal dietary inadequacies that are found in athletes and how other factors, such as nutritional knowledge and age, might also influence their food behavior. However, only a few studies have evaluated the athletes of racket sports 8,9 and, to the best of our knowledge, none of them have been conducted on table tennis athletes. Therefore, the objective of the present study has been to evaluate and compare the nutritional knowledge and the dietary intake between adult and adolescent competitive table tennis players.
MATERIALS AND METHODS
STUDY SAMPLE
Table tennis players from three clubs in the State of Sergipe, Brazil, volunteered to participate in the research. To be eligible for the study, a participant had to be federated, had to have been practicing table tennis, as well as to have participated in at least two tournaments in the previous year. Those individuals with a chronic or an acute disease, or who were on any medication, were excluded.
The data collection occurred during training and two state championships, between September and December of 2015. Forty-two athletes agreed to participate in the study. Thirty-three athletes from the regional training center team, together with nine athletes from two other smaller teams in the capital and from a city in the interior of the state, were all evaluated. During the previous year, 25 athletes participated in national competitions (20 were medalists) and 24 participated in regional competitions (13 were medalists). All of the participants were participating in state competitions.
Twenty-five athletes were adolescents (age range: 10-19 years) and 17 were adults (age range: 21-56 years). All of the adults were male, while two adolescents were female and 23 were male. There was no difference in the results when they were analyzed without the female athletes; thus, they were included. The athletes responded to a nutritional knowledge questionnaire and, in sequence, nutritional assessments were performed. Written informed consent was given by all participants and, if they were not of legal age, their parents. Inform assent was also obtained from the adolescents.
This study was conducted according to the guidelines as laid down in the Declaration of Helsinki and all of the procedures involving the human subjects were approved by the Research Ethics Committee of the Tiradentes University (C.A.A.E.53350316.5.0000.5371).
ANTHROPOMETRY AND DIETARY INTAKE ASSESSMENTS
The anthropometric measurements were performed following the techniques as proposed by Lohman et al. 10. The athlete's height was measured to the nearest 0.1 cm by using a stadiometer (AlturaExata(r)) and their body weight was measured to the nearest 0.1 kg by using an electronic scale (LIDER(r)).
Their dietary intake was assessed by using two non-consecutive 24-hour food recalls (one day of the week and one weekend day). The data on the food that had been consumed, the weight information, the portion sizes, and the food preparation techniques were also collected.
The dietary intake was calculated by using the software AVANUTRI 4.0 (Avanutri Informática Ltda., Rio de Janeiro, Brazil). To increase data reliability, energy and nutrients were analyzed hierarchically based upon the following nutrient databases: Brazilian Food Composition Table 11, Brazilian Institute of Geography and Statistics Food Composition Table 12 and the National Nutrient Database for Standard Reference from the United States Department of Agriculture 13. For any processed foods for which the nutritional information was not available, the data was obtained from the nutritional fact labels that were available on the food companies' websites.
ENERGY, NUTRIENT AND FOOD PORTION EVALUATIONS
The basal metabolic rate (BMR) was estimated using the Schofield et al. 14 equation. The activity level factor was estimated according to the number of training hours 15. The proportions of energy intake and the basal metabolic rate (EI:BMR) were compared by using the Goldberg cut-off points method 16, which was aimed at assessing the underreporting magnitude.
The nutrient intake classification was performed after a comparison of the specific recommendations 2. The carbohydrate intake was compared to the recommendation of 5-7 g/kg/day, while to evaluate the protein ingestion, the recommendation of 1.2-2.0 g/kg/day was used. The World Health Organization (WHO) guidelines 17 were used in order to evaluate the ingestion of total fat, cholesterol, and the fatty acid compositions of the diets. In order to evaluate the fiber intake, the cut-off points as proposed by Williams, Bollella and Wynder 18 were used (adolescents: chronological age plus five grams of fiber; adults: at least 25 g of fiber/day).
The following criteria were adopted in order to calculate the percentages of inadequacy of the athletes 19. The individuals with intakes below the recommendations of carbohydrate, fiber, monounsaturated fat and polyunsaturated fat were considered as being inadequate. For total fat, cholesterol and protein, the athletes who consumed more than the recommended intake were also considered as inadequate.
The ingestion of micronutrients was classified following the Dietetic Reference Intakes Standard. According to the American Institute of Medicine 15, the intakes of vitamins and minerals under the estimated average requirement (EAR) were considered as inadequate. Since the mean intake of sodium in Brazil is elevated, the values of the tolerable upper intake level (UL) were used in order to determine the prevalence of individuals with an inadequate intake of this nutrient 15.
The consumption of food portions was compared to the recommendations as proposed by the Brazilian Food Pyramid 20. The percentages of inadequacy were calculated from the prevalence of those individuals below the proposed recommendations, except for oils, fats, sugars and sweets. For these groups, the inadequacy percentages were obtained from the prevalence of the individuals who were over the recommended portions number.
NUTRITIONAL KNOWLEDGE
A two-part questionnaire was distributed to all of the athletes. The first part of the questionnaire presented demographic questions, including age, education level, hours of training/week, a rating of their own diet quality, reasons for not eating healthier food (responded only to those that rated their own diet quality as poor), as well as their nutritional information sources 21.
The second part of the questionnaire consisted of a validated nutritional knowledge test 22,23. The questionnaire had 14 questions divided into three sections. The first section contained three multi-choice questions about the basic aspects of nutrition. The second part consisted of a question that was related to the Brazilian Food Guide Pyramid, where the athletes had to fill in the pyramid with the correct food groups. The third section addressed the issue of sports nutrition and it was comprised of ten statements to which the athletes should mark "yes" if they agreed with the statement, "no" if they disagreed with the statement, or "do not know" if they were unsure. The correct issues were worth a plus point and the wrong or "do not know" answers received no points. The average percentages of the correct answers were calculated.
The questionnaire had its discriminative validity determined in a previous study by our research group 21. The test was applied to 19 graduates of the 4th period of nutrition and to 16 adolescent athletes. To be considered as valid, the questionnaire had to be able to differentiate the participants at different levels of knowledge. After the application, the students had a significantly higher mean percentage of correct answers (97.4%) than did the athletes (57%).
STATISTICAL ANALYSIS
The software SPSS, version 17.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analyses. The numerical variables have been presented as mean and standard deviations (SD). Non-normally distributed variables were presented as medians and interquartile range (ICC). For the categorical data, absolute and relative prevalence were used. Continuous measurements were compared between the adolescents and the adults by using independent-sample Student's t-tests and the categorical data was compared by using Pearson's Chi-square test. Non-normally distributed data were compared by the Mann-Whitney non-parametric test. Pearson's correlation coefficients between the ingestion of key nutrients that are commonly used to analyze diet quality in nutrition knowledge studies (calcium, phosphorus, sodium, fiber, total fat, dairy, vegetables, fruits, sweets, oils and fats) and the nutritional knowledge measurements were also calculated 6. Non-normally distributed variables were log-transformed before correlation analysis.
Due to underreporting, the residual method was used in order to obtain energy adjusted amounts of nutrients and food portion intakes 24. The method is an alternative to control for confounding the total energy intake and to remove the extraneous variations due to the total energy intake.
The internal consistency of the nutritional knowledge questionnaire was obtained by Cronbach's alpha coefficient (). A minimum value of 0.70 was recommended by Rowland, Arkkelin and Crisler 25. For all analyses, a statistical significance was set at p < 0.05.
RESULTS
The adolescents and the adults had a mean of 13.8 ± 2.5 and 33.6 ± 10.8 years (p < 0.05), respectively. There was no difference between the athlete's hours of training per week (adolescents: 6.4 ± 4, adults: 5 ± 1.5, p < 0.05).
Most of the adolescents (92.8%) were at middle/high school, while all of the adults had completed a higher education degree. There were no differences between the groups in the prevalence of underreporting (adults: 58.8%, n = 10; adolescents: 36%, n = 9, p < 0.05).
The athletes from both groups showed a high prevalence of inadequacy in their ingestion of cereals, vegetables, dairy and sweets and more than half of the adolescents were inadequate in their ingestion of fruits and legumes.
The adolescents showed a higher intake of carbohydrate and protein and a lower ingestion of vitamins A, B5, B6, C, calcium, zinc and phosphorus (Table 1). Both groups showed a high prevalence of inadequacy in the ingestion of nutrients. However, the adults were more inadequate in their ingestion of carbohydrate and protein, while the adolescents showed a higher inadequacy in vitamins B6, B9, C, and phosphorus (Table 1).
Table I. Nutrient intake and prevalence of inadequacy in adult and adolescent table tennis players (n = 42)

Vit.: vitamin; SAF: saturated fatty acids. MUFA: monounsaturated fatty acids; PUFA: polyunsaturated fatty acids.
*p <0.05 by Mann-Whitney test.
†p <0.05 by Pearson's Chi-square test or Fisher's exact test.
A higher prevalence of adolescents rated their dietary quality as excellent/good, while a higher prevalence of adults rated their dietary quality as poor/very poor. The adults reported that habit was the reason for not eating healthier. The nutritional information sources that were most used by the adolescents and the adults were their parents and the Internet, respectively (Table 2).
Table II. Self-perception of dietary quality and nutrition information sources of adult and adolescent table tennis players (n = 42)

*p < 0.05. †Responded only by those that rated their own diet quality as poor/very poor. The other categories were not presented due to the lack of responses.
The internal consistency values of the nutritional knowledge questionnaire showed an acceptable reliability for both groups (adults: 0.88; adolescents: 0.86). The between-group analyses showed that the adults had a higher nutritional knowledge than did the adolescents (Table 3).
Table III. Mean (standard deviation) of the nutrition knowledge of adult and adolescent table tennis players (n = 42)
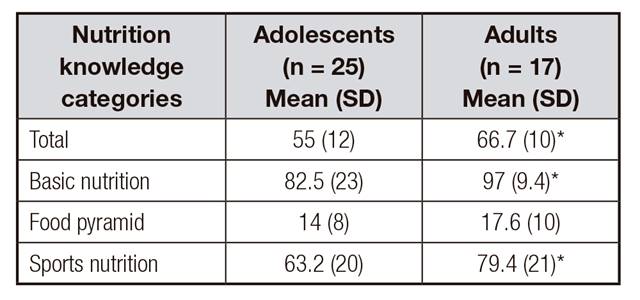
*p < 0.05 by independent t-test.
Negative correlations were found between adults' total nutritional knowledge and their sodium intake (r = -485) (p < 0.05). There was no correlation between adolescents' nutrition knowledge and dietary intake.
DISCUSSION
To the best of our knowledge, this is the first study that has evaluated the dietary intake and the nutritional knowledge of table tennis players. The table tennis game is characterized by periods of effort and rest. For the fast and powerful movements during a rally, it is the anaerobic system that is decisive, as it represents the difference between winning and losing 1. Therefore, muscle glycogen appears to be the main source of energy during the game 1. In the present study, the athletes showed a high prevalence of inadequacy in carbohydrate, which may negatively affect their performances. Fatigue by low glycogen levels may be manifested by decrements in power, stamina, poor positional play, and mistimed or miss-hit strokes, which may lead to a decline in the accuracy of the shots played 26.
Athletes from both groups showed a poor quality of diet. This was demonstrated by the high prevalence of inadequacies in their ingestion of fruits, vegetables, sweets and dairy. The low variety of food groups may have contributed to the inadequate intake of important nutrients, such as fiber, unsaturated fat and vitamins. Fiber and unsaturated fat have a role in the prevention of metabolic diseases 17,18, while B-complex vitamins act as enzymes during the reactions of energy production. Antioxidants (i.e., vitamins E and A) may help in the prevention of oxidative damage that is caused by exercise 2.
Only a few studies have analyzed the dietary habits of athletes from the racket sports and most of them have been conducted on tennis athletes 9. As far as we know, this is the first study that has addressed the dietary behavior of table tennis players. The inadequacies that were found were similar to those that have been observed in badminton athletes 8. These were higher than those that have been observed in the most studied modalities, like endurance sports 27, together with other intermittent modalities, such as tennis 9. It should be noted that, different from table tennis, the sports cited above have been researched for more years and have detailed and practical guideline positions 28,29. This knowledge might have been transferred to athletes by health professionals and public policies, thus, influencing the cultures of the sport. Therefore, the present study is relevant, as it may serve as a way of catching the attention of sports professionals and table tennis athletes to the importance of an adequate diet. Future studies should elaborate on sport-specific guidelines for this sport.
The results have shown that dietary inadequacies were found in both groups, however, the adolescents showed a high prevalence of inadequacy and lower nutrient intakes than the adults. Similar results were found by Keppling et al. 30. Nutritional deficits and poor eating habits in adolescent athletes may compromise growth and contribute to the occurrence of injuries. Chiplonkar et al. 31 found that lower levels of calcium, zinc, folate and vitamin C were associated with a short stature and these lower levels may increase the risk of bone injuries. Low levels of zinc may affect a cognitive performance 32, which might influence those abilities that are decisive for achieving success in a table tennis game, such as motor control, coordination and decision making.
The adolescents also showed a worse self-perception of dietary quality than did the adults. This result might be related to the lower levels of nutritional knowledge found in this group. Studies reporting on the influence of age on nutritional knowledge have consistently found that younger participants score lower than middle-aged individuals, possibly by the lack of interest in nutrition (adolescents consider nutritional knowledge less relevant) and differences in the participant's levels of education 33. Levels of education have been associated with superior performances on other nutritional knowledge instruments and this has been more than likely supported by the capacity to use written material, in order to gain nutritional knowledge and then to implement favorable lifestyle behaviors 34.
Nutritional knowledge is one of the few modifiable determinants of dietary behavior. Individuals with a higher nutritional knowledge are almost 25 times more likely to meet the present recommendations for fruit, vegetable and fat intakes, than those with a low knowledge 34 and have a healthier diet 6.
Differently from those studies involving adults, research regarding adolescents has found fewer, or no correlations, between nutritional knowledge and dietary practices 35,36. The scarcity of association may be due to the numerous barriers that can hinder adolescent athletes from translating nutritional knowledge into practice. The adolescents may have difficulties in achieving an appropriate intake of some nutrients, due to the increased needs that are related to growth. In addition, their search for identity, their struggle for independence and acceptance, which are characteristics of this phase, may be expressed through eating less healthy foods, or not eating as an act of parental defiance. The high vulnerability to societal and peer pressure, often reinforced by the media, may also negatively influence their dietary practices 37.
The results of the present study have shown that the table tennis players had poor dietary habits and a low level of nutrition knowledge, thus, such nutritional interventions in this population are warranted. Nutritional education programs should specifically target gaps in the knowledge. In this way, an explanation of food pyramids would help to encourage and emphasize the importance of a healthy diet. Strong declarative knowledge, without procedural skills, may not translate to a healthier dietary intake, so specific nutritional advice about the ingestion of cereals, dairy foods, fruits and vegetables should be included. Future studies should also test the efficacy of nutritional education programs that involve trainers, parents and web-site interventions, as these are the most used nutritional information sources for athletes, and analyze the impact of these interventions on table tennis performance.
LIMITATIONS
Despite the relevance of the present study, some methodological limitations must be taken into consideration. The analysis of food intakes by using two 24-hour recall periods is a limiting factor. However, it was necessary to use this particular method due to the operational difficulties in accessing the same participant more than twice. According to Magkos and Yannankolia 38, in these cases, the use of less than three 24-hour recall periods might be an alternative. Other works have also used this method 22. The low number of participants may also be a limitation since bigger samples reduce the inter-subject variability when assessing dietary intake.
CONCLUSION
The present study has shown that table tennis players have inadequate dietary habits and low levels of nutritional knowledge. They also use a low quality of nutritional information sources. When comparing the groups according to age, the adolescents showed higher dietary inadequacies, a worse self-perception of dietary quality, as well as lower nutritional knowledge levels, than did the adults. There was only a negative moderate correlation between nutrition knowledge and sodium intake in adults.

