Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
According to the World Health Organization (WHO), healthy ageing refers to an individual's capacity to do the things that are important to the person. Healthy ageing is the process of developing and maintaining the functional ability that enables well-being in older age 1. The healthy aging concept has widely developed as the set of biological conditions and behaviors involved in an appropriate lifestyle aimed at improving well-being and life expectancy without disabilities 2,3, and there is quite evidence that shows that nutrition is relevant among these factors 4. In fact, the role of nutrition in the prevention and treatment of age-related diseases and disabilities has been highlighted by the European Union 5, which associates nutrition with a set of diseases related to pathological aging: cardiovascular disease, cancer, diabetes, osteoporosis, sarcopenia and cognitive impairment/decline. In consequence, nutrition has also been associated with independence, well-being and safety of life due to its incidence in functional limitations 6,7 8 9 10-11.
Several indexes have been used to measure the quality of nutrition in advanced ages. Most of them are derived from the Diet Quality Score (DQI), the Alternative Healthy Eating Index (AHEI), the Mediterranean Diet Score (MDS) or the Healthy Diet Indicator (HDI), which have been explained in an extensive revision carried out by Gil et al. in 2015 12. These indexes are frequently designed to be applied to any segment of the population based on overall healthy intakes, usually assumed in research 13. The AHEI, HDI and DQI measure the adequacy of nutrients and diet. They were designed on the basis of a general healthy diet, considering nutrients and food servings, to relate diet with chronic diseases (AHEI) or with mortality (HDI and DQI). The MDSmod measures the adherence to the Mediterranean diet, widely considered as a healthy dietary pattern. Each index has been designed according to a different rank score, indicating that the higher the score the better the score is, except in the DQI, where the ratio is inverse. None of these validated existing indexes was originally designed to evaluate nutrition in order to avoid pathological aging in the elderly population.
There is a wide literature that relates specific nutrients, combinations of them, or specific daily intakes to prevention of chronic diseases and functional limitations. Further quality research is needed to compile these nutrients, and as far as we know, there is no validated index in the literature for measuring the quality of nutrition aimed to prevent pathological aging. Therefore, the objectives of this study were: a) to retrieve from the scientific literature the nutrients and intakes that have shown to be involved in the healthy aging; and b) to propose a new index, considering these nutrients and intakes, to evaluate the quality of nutrition in relation to a healthy aging.
MATERIALS AND METHODS
To identify the nutrients that influence healthy aging, an exhaustive bibliographic review was carried out to retrieve the available information on the nutrients associated with healthy aging. For all the nutrients, the syntaxes were elaborated combining the name of the nutrient with different factors involved in the aging process, using the terms aging, diet, nutrition, elder, elderly, lifestyle and disability, and six groups of diseases associated with pathological aging according to the literature : cardiovascular disease, cancer, diabetes, osteoporosis, sarcopenia (loss of muscle mass), cognitive impairment and cognitive decline. The search was carried out in the databases Medline, PubMed, Embase, CAB Abstracts, CINAHL, Scopus, JSTOR, Web of Science and Google Scholar.
Only original articles and bibliographic reviews published between 2000 and 2017, written in Spanish, English and Portuguese, which analyzed the association between a nutrient and its effects on aging and the diseases associated with it were included. Initially, a total of 206 articles were retrieved, and after eliminating the repetitions, 161 articles were left to proceed with the selection process.
Each article was reviewed independently by two expert nutrition researchers (ML and LM), making a selection of the articles of interest that met the inclusion criteria. Those articles showing a disagreement between the two reviewers on compliance with the inclusion criteria were evaluated by a third expert nutrition researcher (JMR) who decided if the article was finally included in the review.
The selection of articles was carried out in three stages. In the first stage the articles were selected based on the reading of the title (in this first stage a total of 73 articles were excluded). In a second stage, the articles were selected based on the content of the abstract (in this stage, 29 articles were excluded). In a final stage the articles were selected based on the in-depth analysis of the full text of the article (in this stage eleven articles were eliminated). It was verified that the articles excluded in the last stage did not meet the inclusion criteria of the bibliographic review.
To achieve the second objective, it was necessary to compile the nutritional and dietary data of two convenience samples of elderly people to compare and validate the results. Non-institutionalized elderly people were chosen as target population. Hence, two convenience samples were recruited among users of the public social welfare services offered in the eastern region of Spain. People of both sexes, aged 65 and over, were included. Only those with a lack of cognitive ability to follow an interview were excluded. Thus, up to 469 potential participants were recruited although all questionnaires with missing data were dismissed, so finally 354 participants were included.
Participants of the first sample (n = 203) were residents of four metropolitan municipalities (with populations between 20,000 and 70,000 people). Participants of the second sample (n = 151) were residents of eleven rural municipalities of inland regions (with populations between 500 and 5,000 people).
Data on dietary intake, dietary habits, anthropometrics and demographics were collected from all participants through interviews. The interviews were carried out by social workers from each collaborating municipality, previously trained by the project managers at University. Data on food consumption were obtained in strict spring season to guarantee the same food seasonality. The PREDIMED validated food-frequency questionnaire was used 14. To verify the quality of the diet, data obtained through questionnaires were analyzed by the DIAL software, version 2.12. The daily intake of energy, macronutrients, micronutrients, alcohol and water of each participant was calculated.
The protocol of this study was approved by the Ethics Committee of (removed for blind peer review) and respects all the principles of the Declaration of Helsinki and the Spanish legal regulations on protection of personal data. Study participants were informed of the objectives and the scope of the study and signed an informed consent for their participation.
Nutritional and dietary data obtained from the study sample were used to calculate the scores of four nutritional indexes already validated: MDSmod, AHEI, HDI, and DQI, as well as the proposed new Healthy Aging Diet Index (HADI).
The procedure followed to select the nutrients to be considered in the new HADI was carried out in two stages: a) in the first place, the six groups of diseases most frequently associated with pathological aging were chosen, according to the literature (cardiovascular disease, cancer, diabetes, osteoporosis, sarcopenia and cognitive impairment/decline) 5; and b) next, from the group of nutrients found in the literature review, those that were significantly associated to these six groups of diseases were selected to be reflected in the HADI, also considering the dietary pattern followed by the population samples of this study 15.
Likewise, the total intake of liquids was added to the design of the HADI due to its well-known effect on the general state of health in elderly people and its relevance in dehydration.
Additionally, optimum daily consumption ranges were considered according to the recommendations made in the literature 15,16,17,18,19. The score was applied following the methodology used in the validated indexes 12, based on the discretization. Thus, the participant obtains 1 point if the average intake of nutrients meets the criterion, and 0 if it does not comply.
The "optimal score" was defined as the maximum score that can be obtained with the application of the HADI and its value is 14. The closer the score of the maximum score is, the better the quality of the diet in relation to a healthy aging.
Thus, mean scores of each index were calculated in both samples to assess the suitability of the nutritional pattern and to evaluate possible differences in both samples. See Gil et al., 2015 12 for design details as well as the methods to obtain the scores in each validated index.
The result of each index was presented as scores (two decimals) and also as a percentage (one decimal) of the maximum score established for each index to compare the scores obtained with these four indexes and the new index proposed in this study (HADI).
The Student's t-test was performed among samples to verify the estimates of the indexes (p-value > 0.05 indicates equivalence between samples). All statistical analyses were performed using R version 3.2.4.
The STROBE guidelines for observational studies have been followed in this study.
RESULTS
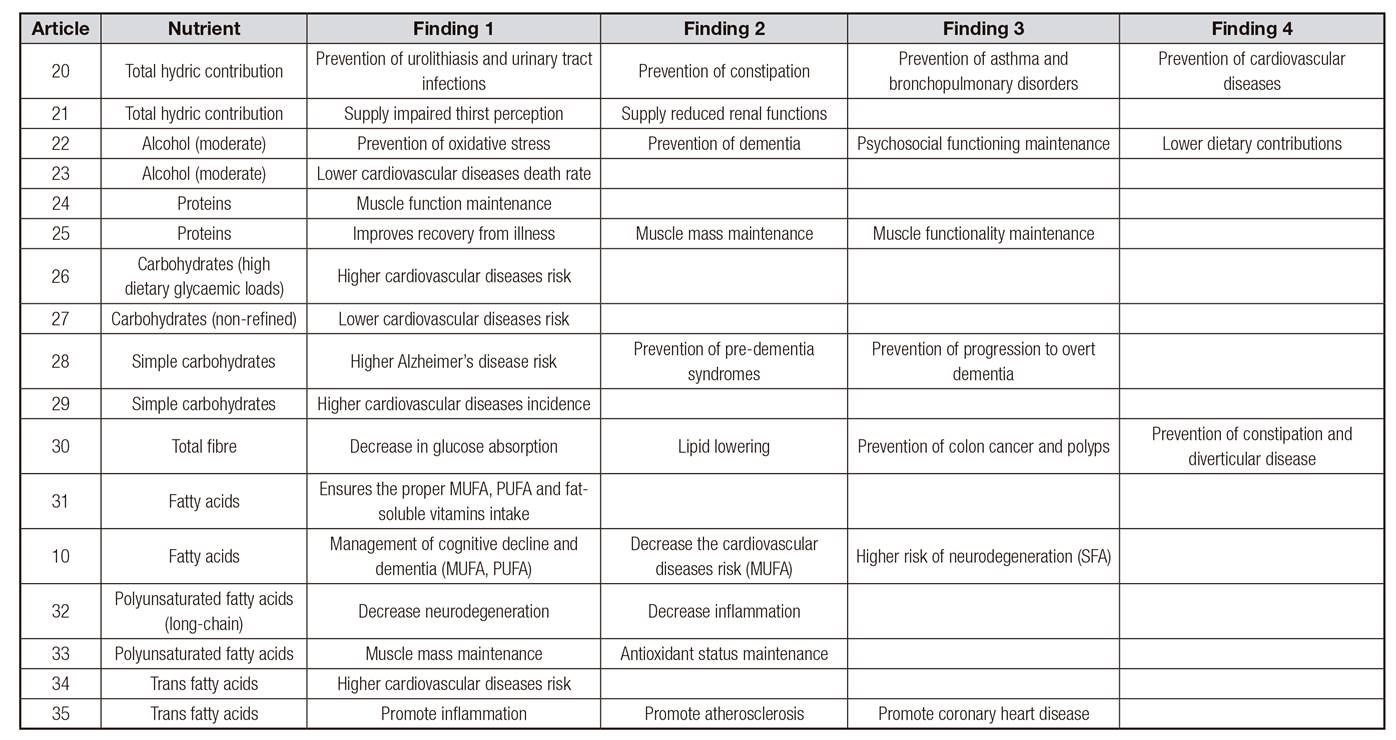
Figure 1 summarizes the articles retrieved in the bibliographic review carried out to identify the nutrients involved in healthy aging. Likewise, this figure details the number of articles excluded at different moments of the peer-selection process. In all cases, articles that did not meet the inclusion criteria were excluded, and a total of 48 articles 10 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65-66 were finally selected for the in-depth analysis of the full text. The results extracted from these 48 articles, with special attention to the nutrients for which significant associations were found with some of the diseases related to aging, can be consulted in the Appendix 1. A complete list of the nutrients related to aging is shown in Table I. The scientific literature that supports the associations between each nutrient and the diseases is also shown in the table.

Figure 1. Selection process of articles. Bibliographic review to identify nutrients involved in healthy aging.
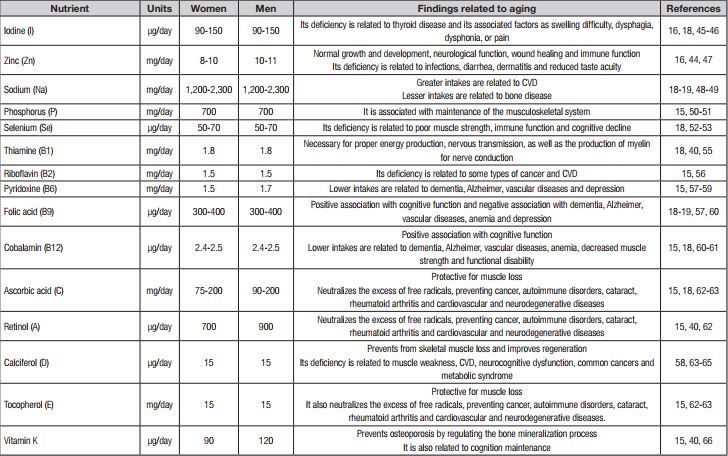
Table I. Bibliographic review: nutrients involved in healthy aging. Optimum intakes, findings related to aging and references
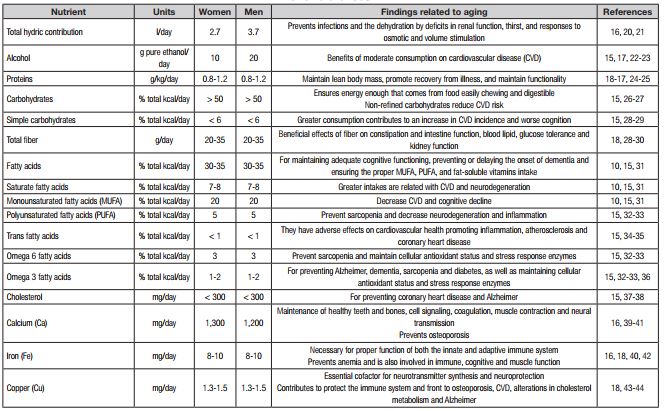
CVD: cardiovascular diseases
Associations were found between cardiovascular diseases and macronutrients, dietary fiber, sodium and vitamin D; between cancer and fatty acids; between diabetes and fatty acids, fiber and simple sugars; between osteopenia or osteoporosis and calcium and vitamin D; between sarcopenia (muscle mass loss) and proteins, calcium, and vitamin D; and cognitive impairment or cognitive decline was associated with fatty acids and folates.
All these nutrients for which associations were found were incorporated into the new index. Table II summarizes the design of HADI. The scoring for each nutrient is also presented in the table assigning points, following the procedure described in the methods section. The total intake of liquids was added to the design due to its well-known relevance in dehydration.
Table II. Design of the Healthy Ageing Diet Index (HADI)

*1 g of fat = 9 kcal; each gram of protein equals 4 kcal; each gram of sugars equals 4 kcal.
†Measured as linolenic acid.
To compare the five nutritional indexes, Table III shows the results of all the indexes for both samples. Both samples obtain low scores in all the assessed indexes. In all cases, with the exception of AHEI, sample 2 obtained lower scores, but they were not statistically significant (values of p > 0.05).
Table III. Summary of indexes results (12,13)

*The higher the score the better the score is.
†The higher the score the worse the score is.
The scores obtained for the modified MDS (which measures adherence to the Mediterranean diet) were 4.46/9 and 4.13/9 in samples 1 and 2, respectively. These results point to a higher degree of adherence to the Mediterranean diet of metropolitan participants compared to rural participants. This result was not statistically significant (p-value = 0.07).
The behavior of HADI is similar to that of the previously evaluated indexes, since the scores obtained were 6.24/14 and 6.10/14 in samples 1 and 2, respectively, also obtaining sample 2 the lowest score.
DISCUSSION
The index proposed in this study (HADI) measures the adequacy of nutrients and diet for a healthy aging, and also takes into account the adequacy of nutrient intake for this purpose.
According to the scores obtained in all the assessed indexes, participants of both samples poorly meet the nutritional requirements to achieve a healthy aging. For this reason, the results obtained with the HADI, especially designed for healthy aging, showed the same behavior as the general nutritional indexes, obtaining 46.1% and 43.6% in samples 1 and 2, respectively. When comparing this result with the rest of indexes for samples 1 and 2, the AHEI obtained 35% and 35.8%, respectively; the HDI, 27.9% and 27.1%, respectively; the DQI, 40.8% and 40.1%, respectively; and the dietary index MDSmod reached the highest result, with 49.5% and 45.9%, respectively. Sample 2 scored lower on all indexes. Comparing it with the scores obtained by sample 1, it would be indicating the existence of a diet farther from the optimal point in relation to the adequacy of the diet for healthy aging.
Those results do not differ substantially from other studies conducted outside and within Europe, where the AHEI scores presented are generally low. In a study carried out among 71,495 women and 41,029 men in the USA, the average AHEI values were 52.9% and 58.2%, respectively 67. The AHEI showed similar results in the United Kingdom after being applied to a large sample of the population 68. In the United States and Canada, the DQI obtained 51.8% of the maximum score and the HDI did not reach 39% 69. However, other studies offer results in another direction, with scores for this same index which are much higher. In an extensive review developed by Fernandes et al. in 2015 70, which included eleven international studies, the AHEI scores varied from 56.7% to 96.3%. In the Spanish study analyzed in this review, the AHEI was calculated to 29,478 people and the subset of older people obtained the highest scores (average of 85.7%), with significant differences with respect to the other age groups 71.
In relation to specific indexes to evaluate the Mediterranean diet, such as the MDSmod, adherence to the pattern is usually higher in Spain among women, the elderly and among the more physically active participants 72. It is possible to find studies in the literature reporting an inverse trend for other European countries with different dietary patterns such as Sweden 73.
It is recognized that nutritional indexes are useful and validated tools to assess the quality of the diet of populations 12,13,71. The differences in the scores presented in different publications indicate quite clearly that the scores obtained in the different dietary indexes depend on the dietary patterns of the geographical area where they have been applied and other factors related to the fulfilment of a healthy life, some of which have been analyzed in this study.
Concerning the results shown in terms of demographic variables, our results are coincident with previous studies. The direct relationship between the best socioeconomic status in metropolitan areas and diet has been described in the literature as a general trend in developed countries 74.
Our review has identified nutrients directly involved in diseases related to aging. As far as the authors of this publication are aware, this complete collection of nutrients, which includes their attributes in healthy aging, has not been found in other studies nor has it been used in the design of validated nutritional indexes. This collection of nutrients adds useful evidence for the design of diets that allow healthy aging. The new index proposed in this study (HADI) is a tool of specific nutritional measurement in populations of advanced ages with risk of disability.
This study has some limitations. The data on exposure (nutritional data) and the effects analyzed in this study (diseases associated with aging) were collected at the same time and, therefore, it is not possible to rule out inverse causality by not being able to determine a temporal sequence between causes and effects. However, significant associations have been found that give us clues to start up studies with epidemiological designs that allow establishing causal relationships. Therefore, further research is needed with other epidemiological designs (cohorts or case-control studies) to determine the causal relationships between the nutrients that are part of the diet and healthy aging.