










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Linear growth is considered as one of the best indicators of a child's growth, bearing in mind the importance living conditions have on growth. The World Health Organization (WHO) reports advocate following-up growth as a routine care activity for children and adolescents 1,2.
Growth analysis may take place on account of an individual or community's nutritional state and body ratios. A child's health and nutritional state will be evident in their quality of growth 3. However, the chronological age (CA) does not always reflect adolescents' true levels of growth and development, considering that young people of the same age could display varying degrees of maturity 4.
To evaluate an individual's general growth or maturation, the methods frequently used are the determination of chronological and bone ages, observing variations in weight and height, and demonstrating secondary characteristics of the sexes, which follow up the phases of pre-adolescence and adolescence 3. Puberty is a period of biological maturation, marked by the appearance of secondary sexual characteristics, a growth spurt and alterations in body composition. Thus, the staging of puberty becomes an important measure to characterize an adolescent's level of growth 5.
Bone age (BA) is the skeletal development index, and an aspect of an individual's maturation 6. It is a component pertaining to biological age and considered as the best expression of human development, as it is a more precise and secure indicator than CA to evaluate an individual's progress to maturity 6,7.
Among the factors which may influence bone development, poor nutritional conditions extending for long periods are highlighted, and act significantly in skeletal maturation, causing a delay in BA in relation to CA; similarly, excess weight causes accelerated bone maturation 6,8. The use of the body mass index (BMI) is recommended to diagnose the nutritional stage of population groups, since it is a non-invasive method, is easily accessible, and has high reproducibility and a low cost 9.
An analysis of the variables in children's physical growth and body composition is considered to be important, since it is a relevant health indicator within the context that they are placed. There is still little research related to the level of impairment between nutritional state and bone age. Thus, this study evaluates the relation between BMI and bone age in adolescents.
PATIENTS AND METHODS
This is a cross-sectional study, with primary data collection, carried out in a municipal public network school in the urban zone of Lagarto-Sergipe, Brazil, during August to October 2016. For convenience and at random, the sample comprised 172 adolescents.
The non-inclusion criteria were as follows: individuals aged under ten and over 15, those with severe disorders (neurological sequelae and dystrophy); amputees or those with any physical-postural problem, which compromised checking anthropometric measurements, producing radiographs which impede visualizing the bone structures of interest.
The data was collected by administering a previously standardized and pre-coded questionnaire, managed by a trained team, containing information on socio-demographic data, anthropometric evaluation (weight and height), radiological examination (bone age) and maturational evaluation.
Weight and height measurements were taken for the anthropometric evaluation, according to the techniques proposed by Lohman et al. 10, confirmed with the assistance of portable digital scales (Filizola® brand, with a 150 kg capacity and 100 g intervals) and portable stadiometer (Seca® brand), respectively.
The BMI obtained from the ratio of weight over height squared was analyzed by the BMI indicator/age (BMI/I), classified according to the cut-off points proposed by the WHO 11 in z-score and its respective standard deviations (SD), categorized as: underweight (BMI /I < -2 SD), normal weight (BMI ≥ 2 SD and ≤ +1 SD) and overweight (BMI > +1 SD).
To determine the BA, the method proposed by Tanner & Whitehouse 3 (TW3) 12,13 was used, with carpal radiographs taken according to the criteria suggested by Bloom Junior 14. The left hand was centralized on the metallic film-holder chassis, with the palm facing the film, the axis of the middle finger in a straight line with the axis of the forearm, fingers slightly spread out and the thumb at a 30° angle with the index finger. The X-ray beam was centralized on the third metacarpal bone, at a film-focus distance of 1.52 m.
Identification of the sexual maturation stage was carried out according to the self-evaluation protocol described by Tanner 15, as described in the literature as a good correlation between self- and physician assessments, as demonstrated in epidemiological studies, self-assessment may be sufficiently accurate for a simple distinction between pre-puberty and puberty 16,17. For this evaluation, images with stages of maturational development, different between the sexes, were presented individually to the adolescent, in an especially reserved place. The individual identified their maturational stage at the time of the evaluation and then the identified image was classified according to the stages described by the Tanner Criteria: stage 1: pre-pubertal; stage 2: initial pubertal; and stage 3: peak height velocity (PHV).
The statistical analyses were carried out with the assistance of Statistical Package for the Social Science (SPSS) software, version 20.0. Data normality was verified by the Kolmogorov-Smirnov test for all the variables analyzed. For the variables which did not present a normal distribution, non-parametric tests were used. The continuous variables were presented through descriptive measurements and the categorical variables were expressed as absolute and relative frequencies. Pearson's Chi-squared test was used to evaluate the association between the nutritional and maturational states and sex variables.
To evaluate the difference between the adolescents' BA and CA averages in the maturational and nutritional state categories, the ANOVA test was used, followed by the Bonferroni post-hoc test. The correlation between the BMI, BA and CA variables was evaluated by the Pearson's correlation coefficient. Multiple linear regression analysis models were constructed to verify the influence of CA, BMI and maturational stage variables in the BA estimate. Multiple variables with p < 0.20 were included in the model via stepwise forward and adjustment variables established in literature. The independent variables remained in the multiple model if they were statistically significant (p < 0.05) and/or conformed to the model. A level of significance of less than 5% was adopted for all the tests.
The Federal University of Sergipe Ethics Research Committee approved this research in report No. 745.543/2014, in compliance with the Ministry of Health National Health Council Resolution (Brazil) No. 446/2013 on research involving human beings. Participation in the study was on a voluntary basis, with the signature or fingerprint of the person responsible for the minor on the Term of Free and Informed Consent, after being informed of the study's aims and the procedures which the children would undergo.
RESULTS
One hundred and seventy-two adolescents were evaluated, with the majority being female (62.2%). The CA average was 12.8 (± 1.2) years, while the BA was 13.3 (± 1.9) years. The girls had a higher BMI average when compared to the boys (p = 0.019) and the majority of the adolescents had an adequate nutritional state (73.9%). With regards to the maturational stage, 42.5% were classified as initial pubertal, followed by 40.6% as PHV, and with a difference observed between the sexes (p < 0.001) (Table I).
Table I. Characterization of adolescents for chronological age, bone age, nutritional status and pubertal stage, stratified by gender

*Data expressed as mean (standard deviation). BMI: body mass index.
It was confirmed that the adolescents classified as PHV had a higher BA average for both sexes (p < 0.05). For CA, it was noted that there was a difference in the CA average among the girls when the maturational stage classifications were analyzed (p = 0.003) (Table II). In addition, it was observed that the girls who were overweight had a higher BA average (p = 0.005) (Table III).
Table II. Mean and standard deviation of chronological and bone ages pubertal stage by gender

PHC: peak height velocity; SD: standard deviation. Different superscripts indicate in which classifications of pubertal states significant differences in chronological and bone ages were observed by gender (p < 0.05).
Table III. Mean and standard deviation of chronological and bone ages by nutritional status by gender
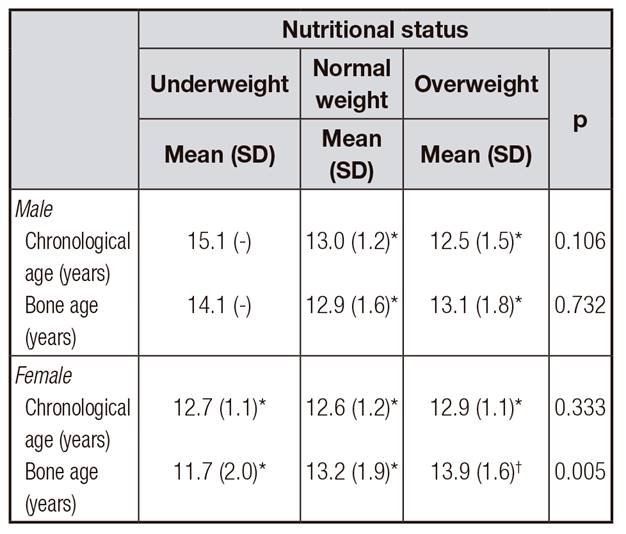
SD: standard deviation. Different superscripts indicate in which classifications of nutritional states significant differences in chronological and bone ages were observed by gender (p < 0.05).
Analyzing the correlation between the BMI, chronological and bone ages, it was verified that there was a moderate correlation (r = 0.440; p < 0.001) between BMI and BA when the general population was analyzed in this study (data not presented in tables). A correlation between BA and the BMI was observed among the male adolescents classified as pre-pubertal (r = 0.419; p < 0.05). For the girls, there was a correlation between the BMI and BA for those in the pre-pubertal (r = 0.798; p < 0.05) and PHV stages (r = 0.421; p < 0.001) (Table IV).
Table IV. Correlation of body mass index with chronological and bone ages by pubertal stage and gender

PHV: peak height velocity.
*p < 0.05; †p < 0.001.
With regards to the relation of the variables to predict the adolescents' BA, it was observed that model 3 (CA, pubertal stage and BMI) explained the variability noted in BA (Table V) in up to 50.3%, represented by the following equation: BA = -0.374 + (CA x 0.754) + (pubertal stage x 0.13) + (BMI x 0.114).

DISCUSSION
Our study demonstrated a relation between BMI and BA, especially between the girls, those in PHV and the overweight. Undoubtedly, the CA should be observed as an important indicator to characterize growth, but not as the cause and main element. There are various ways of evaluating the development of children and adolescents, highlighting skeletal and nutritional state evaluations and an analysis of sexual characteristic development.
Bone maturation reflects physical maturity, as its relation with the appearance of the alterations of puberty are much more straightforward than any other measurement 18. The results of this study indicate that the pubertal stage and BA are directly correlated. As expected, a BA increase was observed with the onset of puberty, corroborating studies performed by Linhares et al. 19 and Cabral et al. 20.
According to Marcondes 6, the fourth most frequent cause of BA progression is early puberty. This fact was observed in our study, considering that the BA was more advanced than CA in girls in the initial pubertal stage than boys at the same stage. Although assessing bone mineral density (BMD), Fortes et al. 21 noted that the more advanced the participants' pubertal stage, the higher the BMD values.
Silva, Daminani and Cominato 22 emphasize that adolescence is a critical period for mineral accumulation, so that deficits in this phase of life could be permanent, increasing the incidence of osteoporosis and, consequently, the risk of spontaneous fractures in adult life. This can be noted in the study by Mika et al. 23, in which anorexic adolescents presented a BMD reduction in the first six months of evolution and a slight improvement in bone mass, following 24 months of treatment.
Therefore, the BMI is highlighted as an important indicator to evaluate growth, yet this variable has been analyzed in relation to CA, which results in a reduction of its explanatory power, since biological age (maturational) becomes a more reliable parameter in adolescence 24.
In relation to nutritional state, it was noted that overweight girls presented higher BA averages, when compared to those who were underweight and had a normal weight. However, no statistically significant difference was observed for the boys. As observed in a previously published study 25, the percentage of body fat of the girls evaluated in this study was influenced more by that of the BMI and pubertal stage (p < 0.001).
This study is in line with the results of Pinero et al. 26, in research conducted with children and adolescents with a CA of between four and 16, in which the results showed a statistically significant difference between healthy and obese patients, with the latter group displaying more advanced bone ages.
These results conform to the review carried out by Marcondes 6, which puts forward that among the factors which influence skeletal maturation, nutritional factors can be highlighted, acting significantly in skeletal maturation, whether with its delay or acceleration. As noted by Elamin et al. 27, confirming a delay in boys' skeletal maturity was higher in the group which had a lower stature, compared to the control group.
It should be highlighted that the literature describes that sex has an influence on BA, since girls had a higher skeletal matural velocity than boys during almost the entire growth period, especially from between the ages of ten and 12 6, the age range in which our research is situated.
In this study, despite a moderate correlation between BMI and BA, when the general population is analyzed, it was observed that this relation among the girls was better for those classified in the pre-pubertal stage and PHV.
Data similar to these results can be found in Nozimoto's 3 study, which concludes that the BA was lower than the CA by up to seven months in underweight boys. However, girls with a low BMI did not present significant differences between chronological and bone ages. The results obtained demonstrated that BMI has a relation with bone age.
Evaluating the relation between BA and BMI, Chaumoitre et al. 28 observed that the BA was more advanced in children with a higher BMI, independent of sex. Similarly, Petrou et al. 8, evaluating obese children and adolescents, observed a statistically significant correlation between BMI and BA for both sexes, concluding that obese individuals tend to have a more advanced BA than CA average. However, considering that their bone maturation is more accelerated than CA, the final height does not exceed the genetically predicted height.
Using a regression model, it was noted that the CA, BMI and pubertal stage may explain the BA variability in this research in up to 50.3%, so that the individuals' BA increases by 0.81 years for every increase in pubertal stage. Godfrey et al. 29, in a study with children and adolescents, determined the formula for bone age index in obese and overweight children and identifying the particular BMI which resulted in bone age advancement. They used the correlation regression formula (bone age index = 0.016 x [BMI] + 0.6742).
Studies reveal that the main periods for bone mass growth are between the M3 breast development period among the girls and G4 stage among the boys 21,30,31. This information is in line with our results, suggesting that there is a window of opportunity to gain bone mass between the ages of 12 and 16 and in the initial pubertal stage.
It is important to emphasize that BMI is a fundamental index in the evaluation of the growth and development of children and adolescents. However, BMI is evaluated in relation to the chronological age, generating a loss of its explanatory power. The relationship between BMI and bone age can be explained by the fact that age is a more reliable parameter for evaluation of child and adolescent development, since the bone age assessed by hand and wrist radiography, as performed in this study, relates to the presence of ossification centers 24.
The results of this study should be interpreted with caution, as there are some limitations. The data was collected at a single municipal school and, therefore, is not a probability sample. In addition, the study age range was reduced (between the ages of ten and 15), limiting extrapolation of the results for individuals under the age of ten. The bone age evaluation can be carried out using different methods, complicating comparability between the studies. It is highlighted that this study is relevant, due to the shortage of research on the topic, especially in Brazil, assisting the understanding of published work.
Prospective studies are required to corroborate these results and better assess the growth and development of children and adolescents, in relation to the formation of bone mass. In addition, intrinsic and extrinsic factors influence an individual's growth pattern and development, which highlights the need to evaluate BA, associated to factors such as economic circumstances and genetic pattern, and relating them to the ethnic characteristics of different populations. Carrying out studies while adopting criteria for analysis, such as by ethnic group, age (children and adolescents) and economic circumstances are suggested to better assess the influence of the nutritional state and specificities which occur between the sexes to evaluate bone age.
The results found resulted in the conclusion that BMI has a relation to BA, especially for females, confirming dimorphisms between the sexes, and the nutritional and pubertal states are related to adolescents' BA. These findings reinforce the use of simple indicators, such as BMI, to evaluate the development of children and adolescents, since it is a simple, reproducible and reliable index.

