










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Chronic kidney disease (CKD) is a pathology related to multiple etiologies; it can be defined as a structural or functional damage of the kidney (1). Studies indicate that there is no clear registry of the number of patients with kidney disease; however, diabetes has been reported as one of the most important predisposing factors for the development of this condition in Mexico, to such a degree that the number of people who suffer from CKD increases on a yearly basis. Diabetic nephropathy is currently the third most important cause of death in Mexico (2).
CKD is a condition characterized by a gradual loss of kidney function due to structural or functional abnormalities over the course of > 3 months. CKD is classified based on cause, GFR category (G1-G5), and albuminuria category (A1-A3), abbreviated as ACR. Stage 5 is the final stage, where patients require supportive therapy either by hemodialysis or peritoneal dialysis. This final stage is called kidney failure and occurs when the glomerular filtration rate (GFR) falls below < 15 mL/min/1.73 m2 (2,3).
Although GFR is only one component of renal excretory function, it is commonly accepted as the best overall index of renal function, given that it usually decreases after some type of structural damage. In CKD, most kidney functions decrease in parallel with the decreasing GFR (4). In most cases, if hemodialysis treatment is not initiated, patients die within a period of one to two weeks, and this period may even be shortened to less than 3 days in older adults (5).
Advanced CKD is a proinflammatory condition in which chronic inflammation contributes to decreased muscle strength and physical function through a reduction in muscle mass (6). High ultrafiltration rates can lead to hypotension and poorer health overall, thus having also a negative impact on muscle strength (7).
Patients undergoing hemodialysis tend to develop muscle wasting, decreased cardiorespiratory capacity and malnutrition, all of which are also associated with chronic diseases such as systemic arterial hypertension (SAH), anemia, dyslipidemia, type-2 diabetes mellitus (T2DM), coronary artery disease (CAD), and years of disease progression. These factors may also play some role in the reduction of muscle mass observed in these patients (8). Reduced exercise capacity is another factor which causes these individuals to be less active, and consequently to have poorer physical function (6).
Many factors may contribute to this decrease in muscle strength, such as muscle atrophy and a decreased ability to generate muscle strength or a decreased ability of the central nervous system to activate the necessary functional mechanisms. Observations show that patients who undergo dialysis treatment tend to have certain structural alterations in their muscle tissue when compared to the general population. These changes are especially evident in type-II fast-twitch fibers (contraction), which develop structural and mitochondrial anomalies comparable to those found in certain myopathies.
Decreased muscle strength, myopathy or uremic neuropathy are all consequences of elevated serum levels of calcium, urea, and hydrogen ions, as well as low levels of carnitine and/or secondary hyperparathyroidism. Chronic uremia is considered to be the factor that affects muscle function the most. Myopathy can also develop in the presence of vitamin D metabolism disorders, high serum calcium levels, prolonged inactivity, malnutrition, or inadequate dialysis (9,10).
OBJECTIVE
This study aimed to compare muscle strength, as measured by dynamometry, in a group of Mexican patients undergoing hemodialysis with available reference values, and to determine the association between dynamometry and age, height, weight, glomerular filtration rate, urea, creatinine, glucose, cholesterol, triglycerides, hemoglobin concentration, and subjective global assessment.
MATERIALS AND METHODS
STUDY DESIGN
A cross-sectional study was conducted with the participation of 150 patients with CKD, undergoing hemodialysis treatment. The sample size was obtained using convenience sampling, a non-probabilistic sampling technique, in order to recruit patients with stage-5 CKD. The participants in question, both men and women, were included if they were between 20 and 81 years of age and were attending the outpatient service of the Nephrology Department of Hospital General Regional No 46 of the Mexican Institute of Social Security, in Guadalajara, Jalisco, between January and July of 2018.
STUDY SUBJECTS
Any patient who met the selection criteria for stage-5 chronic kidney disease, and who was also currently undergoing hemodialysis, was recruited into the study (GFR < 15 mL/min/1.73 m2). Any patients with an active infection, an active neoplastic process, receiving nutritional support, consuming any type of supplement or who required intensive care were excluded from participating.
After the patient selection process, a member of the research team provided a detailed explanation of the study to the volunteers, along with the advantages of participating and information relating to their results at the end of the investigation.
The study was carried out on a date that did not overlap or interfere with the patient's hemodialysis treatment, and dynamometry was performed using the patient's right arm.
The study was approved by the Ethics Committee. The study conforms to the provisions set forth by the Declaration of Helsinki in 1995 (as revised in Fortaleza, 2013). Each patient received and signed an informed consent form, which contained all pertinent information related to the study.
VARIABLES
Clinical measurements
The medical history of each patient was reviewed by a researcher who obtained all the relevant clinical data. Glomerular filtration rate (GFR), creatinine, urea, hemoglobin concentration (male ≤ 13 g/dL and female ≤ 12 g/dL, to rule out anemia) (17), glucose, total cholesterol, triglycerides, and subjective global assessment, which includes certain clinical manifestations such as dizziness, muscular weakness, vomiting, diarrhea and constipation, were obtained with the intention of identifying any associated comorbidities and any associated pharmacological treatment for each patient.
Anthropometric measurements
Body weight was measured using an Omron® brand bioelectric impedance scale. Height was evaluated with the subjects in a standing position; their chin was elevated so that the lower edge of the orbital cavity was horizontally aligned with the upper part of the ear/Frankfurt plane. Height was measured using a Seca® stadiometer. Body mass index (BMI) was calculated as the body weight divided by the height squared (kg/m2), which was classified according to the parameters of the 2005 Australian Guide, which states that BMI is considered to be 23-26 while undergoing dialysis (11).
Triceps skinfold thickness was measured with a Slim Guide® brand plicometer, according to the ISAK protocol. The average arm circumference was measured with a Seca® brand fiberglass tape measure.
Muscle strength was measured in the right arm before the hemodialysis session using a Smedley III hand-held dynamometer (mechanical), with a precision of 2 kg. The patients were instructed to stand with both arms extended towards the sides of the body with the dynamometer facing forward. They were then instructed to grasp the dynamometer with maximum strength for a sustained muscular contraction of 3 seconds to record the maximum value. Three similar tests were carried out with a rest period of at least one minute between each test. The mean of the 3 values was taken to be the final value. The 5th, 10th, 25th, 50th, 75th, 90th and 95th percentiles were calculated for both men and women and were adjusted for age groups. The average values of each age group and for each sex was compared against the 50th percentile of a reference population (12).
STATISTICAL ANALYSIS
Results were analyzed using the SPSS statistical software, version 21 (SPSS, Inc., Chicago, IL, USA). Inter-group differences were calculated using the nonparametric Mann-Whitney U-test. The normal distribution of variables was analyzed with the Kolmogorov-Smirnov test. The associations between dynamometry and age, weight, height, BMI, triceps skinfold thickness, GFR, creatinine, urea, glucose, total cholesterol, triglycerides, SGA and hemoglobin were evaluated using Pearson's correlation coefficient for normal and non-normal variables. A multiple linear regression model was constructed to determine the factors related to muscular strength. A value of p < 0.05 was considered statistically significant. The chi-squared test was used to evaluate the association between qualitative variables.
RESULTS
Initially, a total of 176 patients undergoing hemodialysis were considered for inclusion in the study, of whom 16 were excluded because they did not meet the inclusion criteria, and another 10 refused to participate. The remaining 150 patients were included in the study.
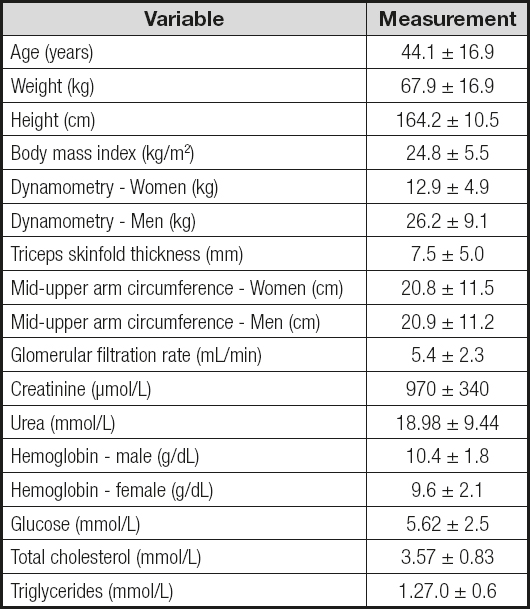
The characteristics of the study population were as follows: 97 (64.7 %) men and 53 (35.3 %) women, with an average age of 44 ± 16.8 years; average body weight was 67.9 ± 16.9 kg, with a GFR of 5.4 ± 2.3 mL/min/ 1.73 m2 and with creatinine and urea values of 11.0 ± 3.9 and 114 ± 56.7 mmol/L, respectively. Table I shows the anthropometric and biochemical variables of the study population. The rest of the variables are shown in table I. The average date of diagnosis was 2010 ± 6 years, thus the time from diagnosis was approximately 8 years on average.
Patients were found to be taking the following pharmacological treatments: iron, 26 (17 %); erythropoietin, 51 (34 %); antihypertensive treatment, 134 (89 %); diuretics, 16 (10.6 %); proton-pump inhibitors, 23 (15 %); insulin, 18 (12 %); calcitriol, 17 (11 %); vitamin B complex, 116 (77 % ); and folic acid, 63 (42 %). Only two (1.3 %) patients were treated with prednisone whereas only 4 (2.6 %) were receiving pravastatin.
Hemoglobin concentration tests revealed that 104 (69 %) patients had anemia, 71 men (68 %) and 33 women (32 %). The groups were further evaluated according to body composition and BMI, with 58 % of the population within the normal weight range while 25.3 % was considered overweight, 10.7 % obese and 6 % malnourished. Some of the most common comorbidities found in this population of patients were: SAH, which was found in 133 (88.7 %) of the patient sample; and T2DM, found in 51 (34 %) of the population. On the other hand, 17 (11.3 %) were found to have no comorbidities. Both patients with SAH and T2DM, however, showed signs of diminished muscular strength with no significant difference between these two groups.
Average muscle strength, as measured by dynamometry, was 26.2 ± 9.1 kg for men and 12.9 ± 4.9 kg for women. In all, 97.9 % of the evaluated men, and 100 % of the women presented a muscle strength which was lower than the 50th percentile of the reference values. These data are shown in table II.
Table II. Comparison of grip strength with mean reference values, categorized by age and sex
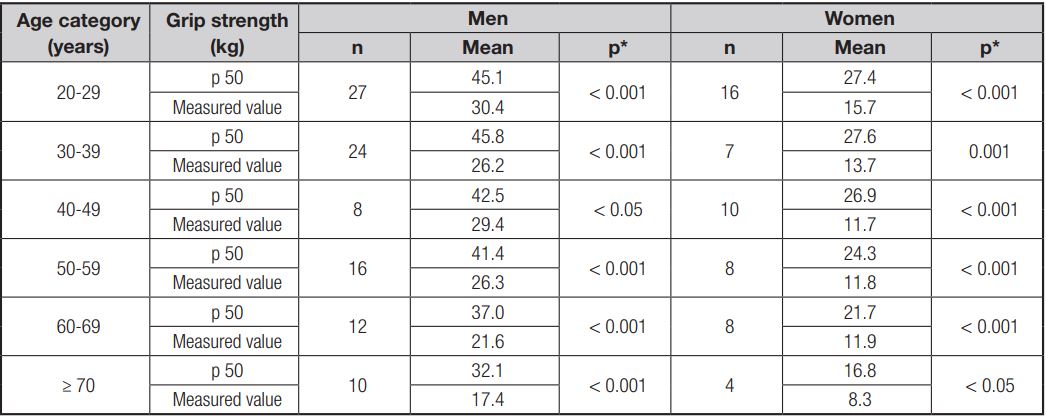
Mann-Whitney U-Test; p 50: percentile 50.
Regarding the results of the muscular strength assessment, 92.3 % of the patients were within the 10th percentile. Table II shows the comparison between the reference dynamometric values (50th percentile) published by Schlüssel and collaborators (12), versus the average dynamometric values observed in this study. The results are categorized by age and sex. Statistically significant differences were found in both men and women, across all age ranges.
Dynamometric values correlated strongly and were statistically significant for age, weight, height, glomerular filtration rate, hemoglobin, creatinine, glucose and subjective global assessment; the results are shown in table III.
Table III. Statistically significant correlations between dynamometry and the evaluated variables
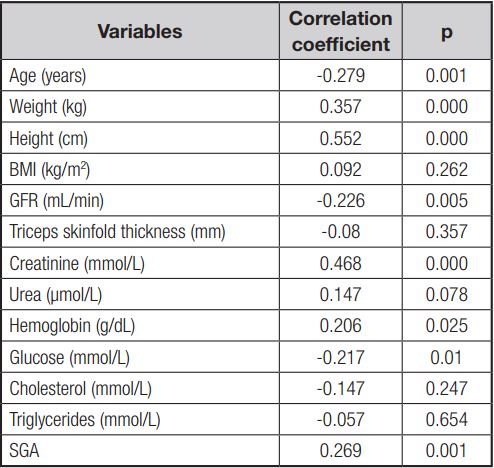
BMI: body mass index; GFR: glomerular filtration rate; SGA: subjective global assessment.
Table IV shows the results of the multiple linear regression. This model explains the results of 45.8 %, which demonstrates that height, glomerular filtration rate, creatinine, and hemoglobin have a significant impact on the dynamometric values of muscular strength.
Table IV. Results of multiple linear regression with dynamometry as dependent variable
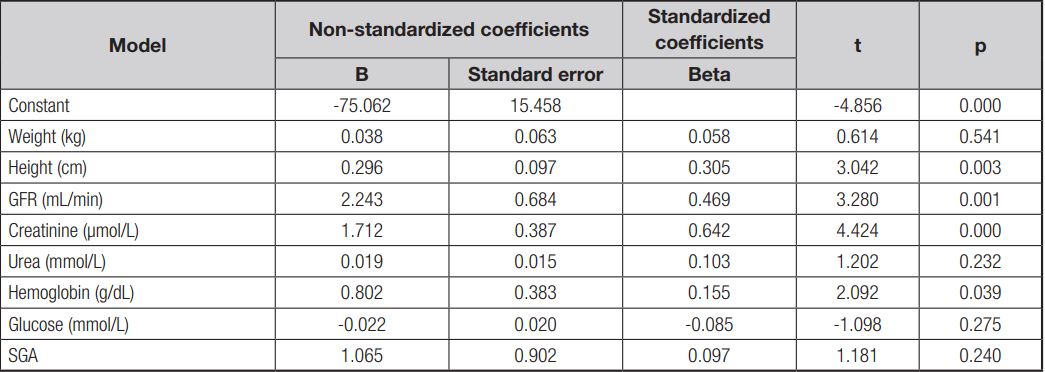
BMI: body mass index; GFR: glomerular filtration rate; SGA: subjective global assessment.
Table V shows the qualitative variable analysis. Statistically significant correlations were found for the following variables: sex vs. BMI, diabetes vs. muscular weakness, glucose vs. muscular weakness, and dynamometry vs. hypertension.
DISCUSSION
The results of this study demonstrate that patients with advanced CKD show a decrease in muscle strength. The overwhelming majority (92.3 %) were found to be within the 10th percentile for muscular strength when compared to reference values; these results are similar to those found in a study conducted by Pinto AP et al. (12), who assessed muscle strength in patients undergoing hemodialysis by measuring grip strength before and after the hemodialysis session. Pinto AP et al. concluded that there was a significant decrease in muscle strength, with about half of the patients falling below the 30th percentile and one third of them below the 10th percentile; The study concluded that, after dialysis, more than fifty percent of the patients were below the 30th percentile for muscle strength.
On the other hand, the most prevalent comorbidities in the study were SAH and T2DM. Our results demonstrated that patients with either SAH or T2DM showed decreased muscle strength. These results are consistent with those found by Amaral C de A et al. (14), who observed that a decrease in muscle strength, measured by means of a survey and dynamometry, was associated with morbidity and multimorbidity among adults in Rio Branco, Acre, Brazil. The study showed that muscle strength in men decreases with age and that this process tends to begin around age 40, and that men with low muscle strength are more likely to develop hypertension, diabetes, skeletal muscle disorders and multimorbidity.
Our results regarding the relationship between muscular strength and age concur with those found in a study carried out by the Nutritional Evaluation Laboratory of the Simón Bolívar University in Caracas, Venezuela, which describes the association between aging and a decrease in muscular strength and motor ability.
Regarding the relationship that exists between muscular strength and height, taller subjects were found to have greater muscular strength, on average, than those of smaller height. This observation was also described in an article published in the Journal of Physical Medicine and Rehabilitation, titled “Relationship between muscular strength and knee proprioception in asymptomatic patients.”
A study carried out by the University of Chile medical school analyzed the grip strength of healthy, 20-year-old subjects, and compared the results between men and women of the same age group. Women were found, on average, to have lower grip strength than men in both hands.
Previous studies, such as the one conducted by Yorke AM et al. (15), have shown that both age and sex are some of the most important factors with the greatest influence on grip strength; however, chronic conditions can also contribute to muscle weakness and deterioration of muscle strength, as can be observed when comparing the grip strength of adults with multimorbidity, who demonstrated a lower grip strength, to those without any chronic conditions. These results are consistent with those found in the current study, where patients who suffered from the two most common comorbidities, SAH (88.7 %) and T2DM (34 %), were found to have lower muscular strength than those without them. It is worth mentioning, however, that hemodialysis and CKD seem to be the most important factors responsible for loss of strength and muscle mass in these patients, regardless of any comorbidities, age or sex.
The results of the correlation between dynamometry, hemoglobin, age, and weight of the current study concur with those discussed by Assun García RS et al., in which muscle strength was analyzed via dynamometry in 102 patients with stage-5 CKD. The results showed that anemia, as a complication of CKD, could also have a significant negative impact on muscle strength and overall physical activity (16). This was of particular importance to our study given that 68 % of patients presented with anemia according to the clinical practice guidelines for anemia in chronic kidney disease (17). Anemia occurs frequently in patients with CKD and has been shown to have a negative impact on overall health.
One of the limitations that we found within our study was the lack of dynamometric reference values for a healthy Mexican population and for patients with kidney disease. Therefore, the current study compares the average dynamometric value of each group of patients, classified by age and sex, against the value of the 50th percentile of those reported by Schlüssel et al (13).
Statistically significant differences were found in all age ranges, both in men and in women, which supports the hypothesis that patients with CKD have impaired muscular strength due to their underlying disease. It would be necessary, however, to have reference values for a healthy Mexican population to better characterize these results and clearly establish this difference.
CONCLUSIONS
Patients with advanced chronic kidney disease undergoing hemodialysis treatment were observed to be within the 10th percentile for muscular strength, measured by dynamometry, thus demonstrating a marked decrease in muscle strength. These results could, however, also have been affected by different factors such as patient age, height, weight, glomerular filtration rate, hemoglobin concentration, serum creatinine, glucose, and the subjective global assessment, given that a significant association was also found between these and muscle strength. The results of the current investigation support the routine assessment of grip strength, which can provide prognostic data and information about the functional limitations in patients with advanced CKD undergoing hemodialysis treatment.

