










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Water is the most basic requirement of all living beings, ensuring the maintenance of normal physical and cognitive functions (1). Insufficient fluid intake has been associated with adverse health effects in adults (2), (El-Sharkawy, 2015, Acute and chronic effects of hydration status on health;Perrier, 2020 #42)and with cognitive impairment in children (3). Childhood is an important period for the adoption of healthy habits, including those related to total fluid intake (TFI), as adopting healthy dietary habits during childhood can facilitate their maintenance through adulthood (4). Besides, drinking sugar-sweetened beverages (SSBs) instead of water has been widely associated with an increase in body fat, and classified as one of the most important risk factors for overweight and obesity during childhood (5-7).
Age- and sex-specific reference values for an adequate intake (AI) of water have been established by the European Food Safety Authority (EFSA) (8). Specifically, the EFSA AI for total water (i.e., water coming from both foods and beverages) is set at 1600 mL/day for boys and girls aged 4-8 years, and at 1900 mL/day for girls and 2100 mL/day for boys aged 9-13 years. Adolescents over 14 years of age are considered as adults, with AIs set at 2000 and 2500 mL/day for women and men, respectively. Although EFSA AIs are based on total water, it is estimated that roughly 20 % of water intake comes from solid foods, while the majority, or roughly 80 %, comes from beverages and drinking water. Thus, it is possible to approximate the AI for water from fluids as 80 % of the dietary reference values mentioned above. These reference values only apply in moderate environmental temperatures and at moderate physical activity levels, so specific conditions must be carefully considered.
Unfortunately, some studies have shown that a high proportion of children and adolescents do not drink enough to meet an adequate water intake (9). A cross-sectional survey conducted in 13 countries worldwide determined that more than fifty percent of the whole study population were at risk of inadequate fluid intake (10). Moreover, a survey performed in children and adolescents in Latin America, Europe, and Asia concluded that plain water accounted for less than half of TFI, and indicated a prevalent consumption of caloric fluids including juices (11). A recent study in 27 cities in China concluded that only 45 % and 36 % of children and adolescents met the AIs for total fluid intake set by the Chinese Nutrition Society (12), and ranked SSB consumption among the top three sources of fluid intake, together with water and milk (13). Another study performed in Indonesia observed that water was the most frequently consumed drink; however, 24 % of children and 41 % of adolescents consumed at least one serving of SSB per day (14) (national cross-sectional survey). Another study conducted in Latin America, whose participants were children and adolescents, also observed that water and SSBs were the most commonly consumed beverages in this population (15) (national cross-sectional survey). Finally, in a very recent review (16), 12 out of 24 studies reported a mean/median water/fluid intake below recommended levels, while 4 out of 13 studies reporting hydration status indicated under-hydration based on urine osmolality (greater than 800 mOsm.kg-1).
While what children drink is well documented, far less is known about their fluid intake patterns, including the beverages preferred at different moments of consumption during the day, and the beverages chosen for consumption inside or outside the home. Understanding how fluid consumption may differ throughout the day or as a function of location could help drive policy initiatives to encourage healthier drinking habits. As few studies in Spain have focused on the patterns of fluid consumption in young population groups, the aim of our study was to assess the current patterns of fluid consumption among children and adolescents in Spain, including drinking occasions and locations (e.g., at home or at school), and to compare their TFI with the adequate intake (AI) of water from fluids as recommended by the European Food Safety Agency (EFSA).
METHODOLOGY
DESIGN AND STUDY POPULATION
The present analysis reports on a cross-sectional survey in Spain, which was part of a recurring, multinational fluid intake survey campaign using the Liq.In7 questionnaire. The objective of this survey was to assess all sources of fluid consumption, including water and different types of beverages, and their association with other lifestyle variables. The recruitment of participants and further details of the populations included in this analysis have been previously described (17). Briefly, a subsample of 167 (63 % boys) children and adolescents (4-17 years old) were included between April and May, 2018. Participants were recruited via an existing dataset and contacted electronically using a quota-based sampling for age, sex and Nielsen areas, in relation to the total country population and confirmed by the National Statistical Institute (18). Recruitment was limited to one individual per household. Participants who had a parent or a caregiver who was illiterate, or working in a company advertising, marketing, doing market research for, manufacturing, distributing or selling different types of beverages were excluded from participation, as these individuals might be more aware of their fluid intake. Taking medication or suffering from a medical condition (dialysis, heart diseases, etc.) requiring restricted fluid intake, and following a specific diet were also exclusion criteria. Coupons for free products were offered to parents or caregivers for taking part in the study. Each child's parent or caregiver consented to participate via an online questionnaire, and all data were recorded anonymously.
ASSESSMENT OF FLUID INTAKE AND OTHER VARIABLES
Participants or their parents reported all their fluid intake by completing the Liq.In7 questionnaire, a 7-day fluid-specific record previously validated for accuracy and reliability (19), every time they drank something (any drink; e.g., water, beverages, cold and hot drinks, alcohol) for a period of 7 continuous days. For children and adolescents under the age of 16 years a single parent was responsible for completion of the questionnaires. The participants or their parents could fill in the questionnaire up to 48 hours from the actual time of drinking.
The Liq.In7 record is structured according to different times of day from awakening, mealtimes (breakfast, lunch, dinner), in-between meal times (morning, just before lunch, afternoon, evening, just before going to bed), until bedtime. The participant or their parent received instructions to report everything they drank at any moment of the day with the following details: fluid type, volume consumed, size of the container used when they were drinking, where the beverage was consumed, and whether food was also consumed, but the specific type of food was not reported.
In addition to the fluid intake assessment, other variables and lifestyle indicators were also evaluated, such as socioeconomic characteristics, region, habitat (urban or rural classification), and parental education level.
CLASSIFICATION AND ANALYSIS OF FLUID TYPES
The included fluid items were: water (tap water, filtered tap water, natural mineral water, sparkling natural mineral water, fountain water); hot beverages (coffee, coffee with milk, espresso with a drop of milk, cappuccino, tea and other infusions and hot beverages); milk and derivatives (milk, milkshakes, milkshakes with juice, liquid yogurt, other milk drinks); sugar-sweetened beverages (SSB) (carbonated soft drinks (CSD), juice-based drinks including nectar, nectar without added sugar, water with juice, other juice drinks, functional beverages including energy drinks, sport drinks, functional water, flavored water, ready-to-drink (RTD) tea and coffee); 100 % fruit juices; artificial/non-nutritive sweetened beverages (A/NSB) (light/zero/sugar-free drinks); other beverages (beverages based on soluble cereals). Total fluid intake was defined as the sum of all these categories. For the analysis, 100 % of fruit juices, A/NSBs, alcoholic beverages, and other beverages were combined under ‘other fluid types'.
Individual mean daily TFI was compared with the EFSA-derived AI for water coming from fluids (8). The number of individuals drinking ≤ 1 serving (250 mL) of SSB per week, 2-6 servings of SSB per week and ≥ 1 serving of SSB per day was analyzed. These cut-offs are based on meta-analyses showing that such amounts of SSB are associated with potential risks for the development of metabolic diseases (6,7,20).
STATISTICAL ANALYSIS
Participants who did not complete the full 7-day record, or who reported a mean daily total fluid intake below 400 mL or higher than 4 L/day for children below the age of 14 years, and higher than 6 L/day for children aged 14 to 17 years, were excluded from the present analysis (n = 21). The demographic and anthropometric characteristics of the study population are presented as either mean and standard deviation (21) for continuous variables, or as number and percentage for dichotomous variables. Intake data are skewed, therefore TFI are presented as median and percentiles; mean and standard error of the mean (SEM) are provided for completeness. The intake of different fluid types is also presented as median, 25th and 75th percentiles. The intakes of each fluid type according to drinking occasions and locations are presented as percentage of TFI.
Drinking occasions were classified into three categories: 1) meals, meaning that the act of drinking occurred during a main meal (breakfast, lunch or dinner); 2) snack, meaning that the act of drinking occurred with food but outside a main meal; 3) outside meal, meaning that the act of drinking occurred outside a main meal and without any food (a stand-alone drinking occasion). Locations were classified into three categories: 1) at home, 2) at school (including cafeterias), and 3) other locations such as restaurants/bars/pubs, transportation, a friend's or acquaintance's home, sports venue, shopping center, street, park, hotel, hospital, etc.
Wilcoxon's signed-rank test was used to compare medians of total fluid intake between sexes. Statistical analyses were performed using the Statistical Package for the Social Sciences software, version 22.0 (SPSS, Inc., Chicago, IL, USA).
RESULTS
SAMPLE DESCRIPTION
Table I shows the characteristics of the sample. In both age categories, girls were underrepresented as compared to boys (42 % and 33 %, respectively, for subjects aged 4-9 years and 10-17 years). The mean ages of the two groups were 6.4 ± 1.8 years for children and 13.2 ± 2.3 years for adolescents. The distribution of the sample across the geography of Spain was aligned with the current population density map of the country, with Andalusia, the Mediterranean area, and areas around Madrid and Barcelona being those most represented. More than half of the sample in both age categories had parents with university degrees.

DAILY TOTAL FLUID INTAKE
The reported TFIs per age group and sex are shown in table II; there were no significant differences by sex or by age. Total median (25th-75th percentiles) values for the two age categories were 1109 (758-1424) and 1181 (849-1773) mL/day for subjects aged 4-9 years and 10-17 years, respectively.
Table II. Daily total fluid intake (mL/day) among children (4-9 years) and adolescents (10-17 years) by sex

TFI: total fluid intake; SEM: standard error of the mean; NS: not statistically significant. *Wilcoxon's test was performed to compare medians between sexes. †Wilcoxon's test was performed to compare medians between age groups.
COMPARISON WITH EFSA REFERENCE VALUES
Figure 1 shows the proportion of participants consuming ≤ 50 %, 50-75 %, 75-100 %, and ≥ 100 % of the AI of water from fluids derived from the EFSA AI for total water (22). Seventy-two percent of children and 73 % of adolescents failed to meet the TFI AIs derived from the EFSA reference values. Among children, females were less likely to meet the AIs than males (22 % and 32 %, respectively), while the opposite was observed among adolescents, with females more likely to achieve the EFSA AI of water from fluids than adolescent males (41 % and 20 %, respectively). One third of adolescent males consumed ≤ 50 % of the AI of water from fluids, compared to 11 % for adolescent females.

Figure 1. Percentage (%) of participants according to adherence to EFSA AI recommendations for water from fluids among children (4-9 years) and adolescents (10-17 years). AI: adequate intake.AIs for water from fluids were derived from the EFSA AIs for total water, assuming that 80 % of total water comes from water and other beverages: thus, the AIs for water from fluids were set at 1.28 L/d for girls and boys aged 4-8 years; 1.52 and 1.68 L/d for girls and boys, respectively, aged 9-13 years; and 1.6 and 2.0 L/d for girls and boys, respectively, aged 14 years and older.
DAILY INTAKE OF DIFFERENT FLUID TYPES
Median daily intake of the different fluid types is shown in table III by age category and sex. Water was the most commonly consumed beverage, both in males and females, across both age groups, representing 470 (319-691) mL/day in children and 496 (308-805) mL/day in adolescents. Water was followed by milk and derivatives, and by SSBs in both age groups. Together, these three categories accounted for an average of 95 % and 88 % of TFI in children and adolescents, respectively. Median intake of other fluid types is the combination of 100 % fruit juices, A/NSB and other beverages to make reading easy because the volume consumed of each of this specific fluid types was very low.
Table III. Median (P25-P75) daily intake (mL/day) of different fluid types by gender among children (4-9 years) and adolescents (10-17 years)
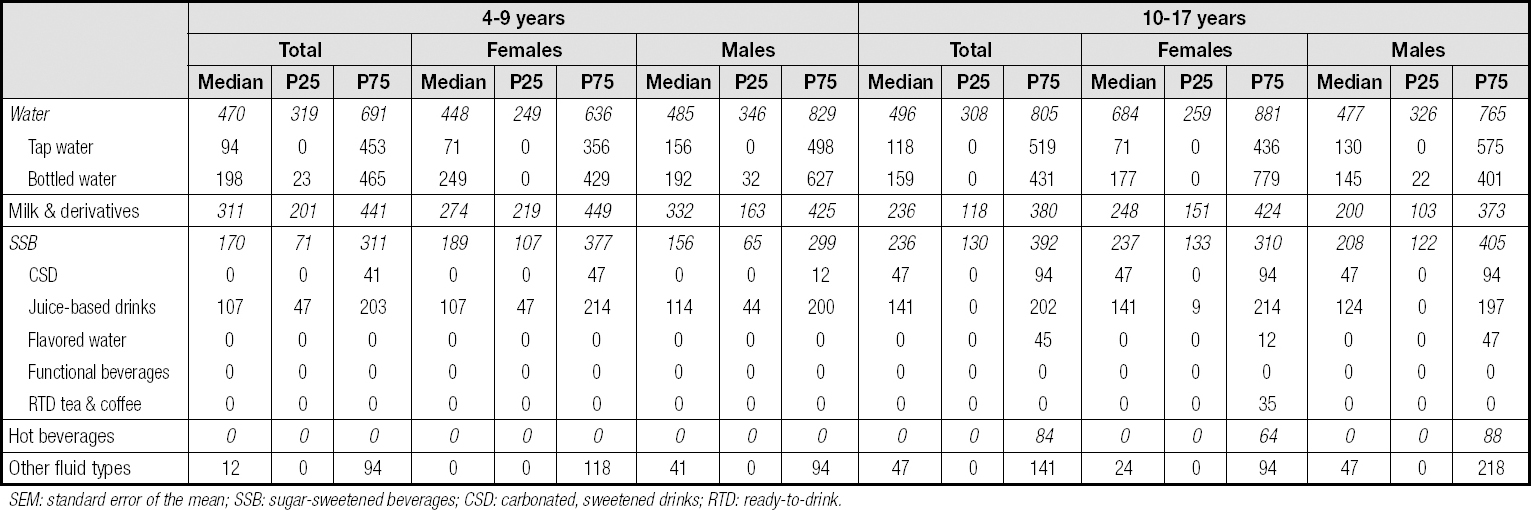
SEM: standard error of the mean; SSB: sugar-sweetened beverages; CSD: carbonated, sweetened drinks; RTD: ready-to-drink.
Table IV shows that most of the children and adolescents drank 2 or more servings of SSB per week (89 % and 95 %, respectively), and that 40 % of children and almost 50 % of adolescents drank ≥ 1 serving per day. When comparing males and females, a higher proportion of males drank 1 or more than 1 serving of SSB per day in both age groups. Around 20 % of both children and adolescents drank less than 1 serving of water per day, with a higher proportion of females consuming less than 1 serving compared to males.

FLUID INTAKE ACCORDING TO DRINKING OCCASIONS
The volume and contribution of the different fluid types to TFI according to occasions are shown in figure 2, while the median intakes are shown in table V.

Figure 2. Volume (mL/day) and contribution (%TFI) of each beverage group to total fluid intake per drinking occasion in children (4-9 years) and adolescents (10-17 years). SSB: sugar-sweetened beverages; A/NSB: artificial/non-nutritive sweetened beverages.
Table V. Median (P25-P75) intake (mL/day) of different fluid types according to drinking occasions among children (4-9 years) and adolescents (10-17 years)
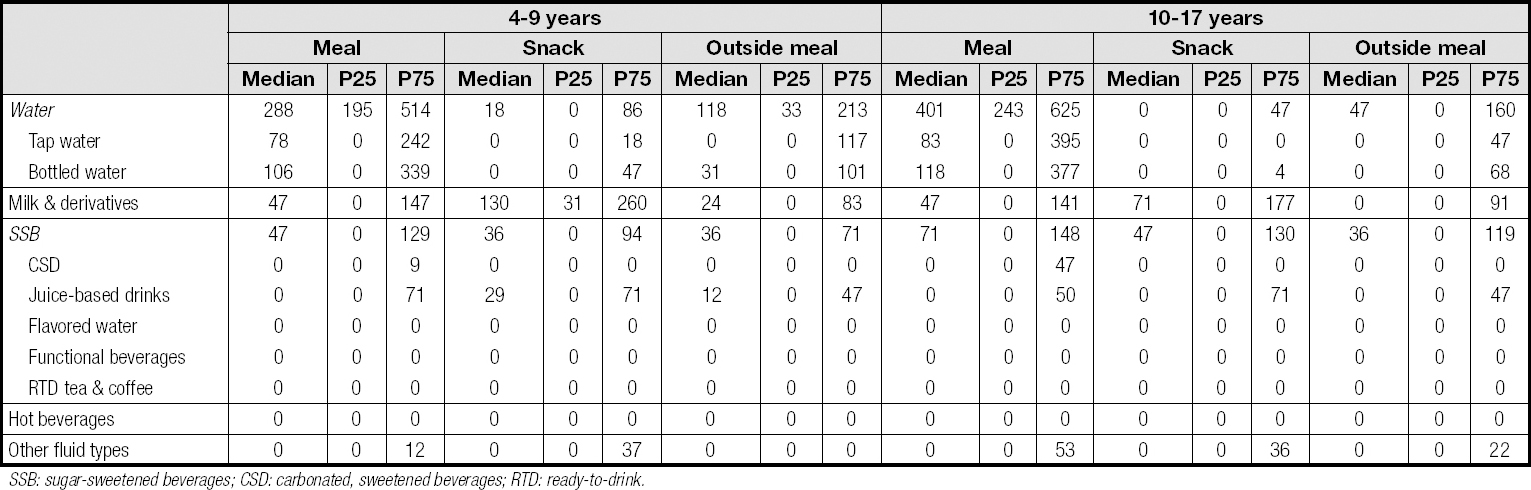
SSB: sugar-sweetened beverages; CSD: carbonated, sweetened beverages; RTD: ready-to-drink.
Fluid intake during meals
In both children and adolescents, the largest proportion of TFI was consumed during main meals (representing 50 % and 54 % of TFI, respectively). During main meals, water was the main contributor to TFI regardless of age or sex (62 % overall). There was no significant difference in the volume of water consumed at main meals between children (288 (195-514) mL/day) and adolescents (401 (243-625) mL/day). In children, water consumption tended to be a larger contributor for males compared to females (66 % and 60 %, respectively); while in adolescents, water consumption was a larger contributor for females compared to males (68 % and 58 %, respectively).
When focusing on SSB contribution, juice-based drinks were the most popular drinks in children at all drinking occasions compared to other types of SSB. In adolescents, juice-based drinks remained the first contributor to SSB, but we observed an increase of CSD contribution when compared to children, with a similar contribution of juice-based drinks during meals (6 %).
Fluid intake during snack occasions
Overall, 25 % of TFI occurred during snack occasions (27 % and 23 % of the TFI among children and adolescents, respectively). In contrast to meals, where water was the dominant beverage, the consumption of milk and derivatives (54 % and 41 % of TFI, respectively) dominated during snack occasions, representing a higher contribution to TFI than SSB (22 % and 29 %, respectively) and water (18 % and 12 %, respectively).
Fluid intake outside of meal occasions
Beverages consumed outside of meals represented 24 % and 22 % of TFI among children and adolescents, respectively. Outside meals, water was the main contributor to TFI for both age groups. As during main meals, milk and derivatives, and SSB were the following main contributors to TFI. We observed sex differences among adolescents, with milk and derivatives playing a larger role in females than in males. Specifically, in females, milk and derivatives and SSB had a similar contribution to TFI (29 % and 26 %, respectively), while in males SSB contributed to 27 % and milk and derivatives to 17 % of TFI.
FLUID INTAKE ACCORDING TO LOCATION
In figure III, the volume and contribution of fluid types according to locations are shown, whereas median intakes (P25-P75) are shown in table VI. In both children and adolescents, the largest consumption of TFI was at home (representing 70 % and 79 % of TFI, respectively). For children, water was the most common beverage consumed at home (47 %), followed by milk and derivatives, and SSB with no relevant differences between males and females. In school, water contributed to half of TFI, followed by SSB and milk and derivatives. No sex differences were observed.
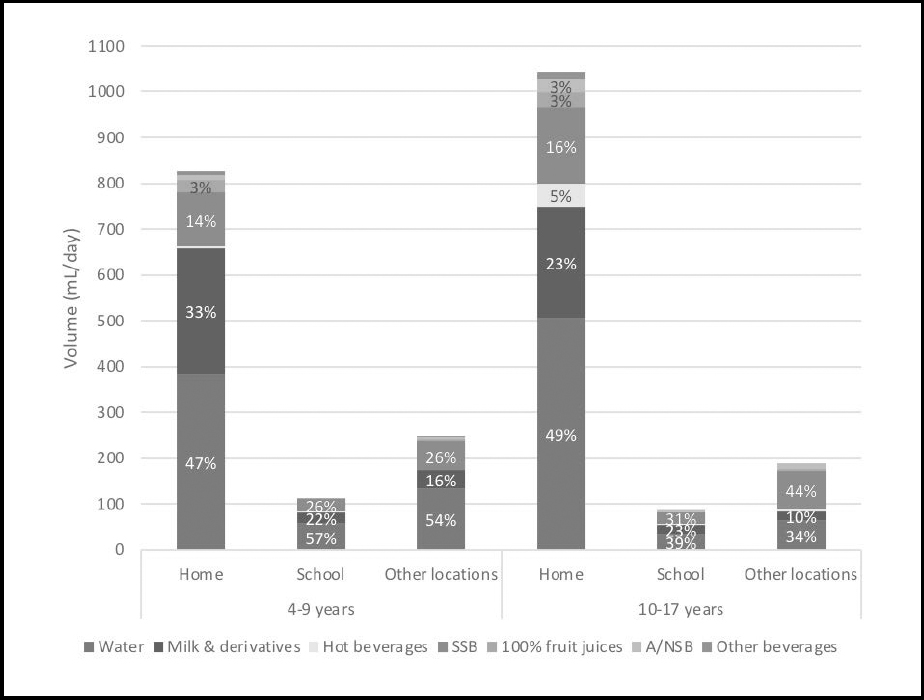
Figure 3. Volume (mL/day) and contribution (%TFI) of each beverage group to total fluid intake per drinking location in children (4-9 years) and adolescents (10-17 years). SSB: sugar-sweetened beverages; A/NSB: artificial/non-nutritive sweetened beverages.
Table VI. Median (P25-P75) intake (mL/day) of different fluid types according to different locations among children (4-9 years) and adolescents (10-17 years)
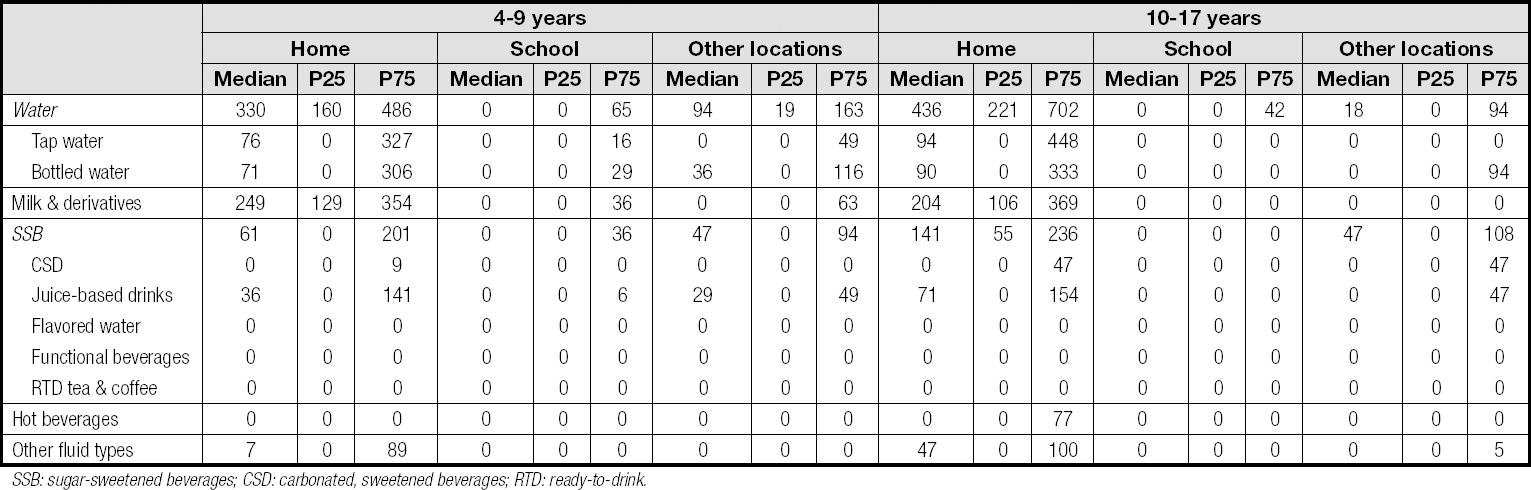
SSB: sugar-sweetened beverages; CSD: carbonated, sweetened beverages; RTD: ready-to-drink.
These observations at school were similar to those at other out-of-home locations. These trends were also found for adolescents at every location with some exceptions: adolescent girls at school drank more SSB (41 %) than water (34 %), and adolescent boys at other locations, who reported a higher contribution of SSB (51 %) than water (29 %) or milk and derivatives (10 %).
In terms of absolute volumes consumed, outside of the home (i.e., at school or in other locations), children and adolescents barely consumed water. Children in other locations (except school) drank at least 1 glass of water (94 (19-163) mL/day).
DISCUSSION
There is increasing interest in the fluid consumption patterns of mainly young populations due to its impact on physical (23) and cognitive performance (24,25) and on body weight-related disorders and their consequences (26). In this study performed in Spanish children and adolescents, we observed that more than 70 % of children and adolescents do not meet the TFI AIs derived from the EFSA reference values (8). For both children and adolescents, water was the most consumed beverage by males and females, contributing to half of TFI, followed by milk and derivatives and by SSBs. Collectively, these three beverage categories reached up to 95 % of TFI and consistently represented the top 3 categories of beverage consumption across age, sex, occasion (meals, snacks, out of meals), and location (home, school, other) categories. The mean SSB intake observed in this survey pointed at almost half of the population consuming SSB on a daily basis. Additionally, some youths drink less than 1 serving (250 mL) of water per day, especially at school. Most of fluid consumption occurred at home (70 % and 79 % for children and adolescents, respectively) and during the main meals, with around half of consumption mainly driven by water across gender and age groups; the rest of intakes were quite equally distributed between snacks and out-of-meal moments. Water consumed during snack times was low, with SSB intake being higher than water consumption.
Compared to the same survey methodology as performed in 2012 (10), mean TFI was strikingly lower than what was previously reported in any of the sex/age categories (more than 500 mL lower than previously reported in male children or adolescents, and approximately 400 mL lower in female children or adolescents). Consequently, the percentage of non-adherence to EFSA-derived adequate intakes is substantially higher than previously reported. While children aged 4-9 showed a higher level of compliance with EFSA-derived AIs (8) compared to adolescents in a 2015 publication, the current study shows this is no longer the case.
Moreover, female children aged 4 to 9 years adhered less to EFSA-derived AI values than males, while in adolescents the opposite was observed, with females being more likely to consume adequate fluids than males. Similar findings were observed in a Spanish survey performed in 2012, as well as in other countries such as in Indonesia, Turkey, and Mexico (10). A potential explanation, could be that boys of younger age are more likely to perform activities that require more energy expenditure than girls of the same age (27), whereas adolescent girls are normally more worried about their health and might try to be well hydrated (28). The very low differences in fluid consumption between age groups are striking. For instance, specifically, TFI both at snack times and outside meals did not differ between children (314 and 278 mL, respectively) and adolescents (310 and 294 mL, respectively). Despite having a larger body size and presumably higher water needs, and despite higher EFSA AIs for water intake, male adolescents did not consume more water than their younger counterparts, so this might be of concern from a physiological point of view since their hydration needs are presumably higher. The difference observed between male adolescents and male children is slightly supported by other European studies showing a decrease in milk intake between childhood and adolescence (29,30). Both children and adolescents have lower intakes of water and of milk and dairy products when compared to a survey published in 2015 (11). This observation is supported by some other surveys showing that milk consumption by children is decreasing over time (30-32). Contrary to what has been shown in other surveys (33,34), this decrease in milk consumption is accompanied by a very slight increase in the consumption of sugar-sweetened beverages. In Europe, adolescents consume more SSBs than older adults and younger children, and there is also some grey literature suggesting children as young as one year old are already consuming SSBs (35).
The intake according to drinking occasions was also observed in a 2014 publication, with 54 % of fluid consumption occurring during main meals, mainly driven by water (17).
SSB consumption raises concerns given their negative effects on children's health (7,20,36), and this applied to the Spanish population, where an increment in soft drink consumption by 100mL has previously been associated with a 0.21kg/m² increase in BMI (37). In addition, the WHO Childhood Obesity Surveillance Initiative (COSI) observed that the prevalence of obesity among the Spanish population is in the highest level of child obesity with approximately 1 in 5 boys, as is also the case in other southern European countries (38). Therefore, more public health policies are needed to slow down and, hopefully, reverse this obesity rate. Of particular concern is the apparently continued rise in SSB consumption among the Spanish and other European populations (increase by 1.2 % in soft drink sales in the EU between 2017 and 2018) (39), whereas we observe a tendency towards a decrease in SSB consumption in other countries such as the USA (40,41). Recent results regarding the effects of SSB taxation in Catalonia, which was introduced on May 1, 2017, have shown a reduction in the consumption of such products (42-44). For now, taxes have been implemented in several countries but the effects on the population's health status have not been examined yet. A recent meta-analysis observed that taxes on SSB reduced also sales and consumption (45). Moreover, some health economic modelling studies suggests promising results of SSB taxes' effect on overweight and obesity (46-49).
In Spain, the average sugar content of SSBs is 10 g per 100 mL, representing 100 kcal (50). Knowing that the estimated, recommended daily energy intake of children and adolescents is about 1800 and 2500 kcal, respectively (51), the consumption of SSBs on a daily basis represents 5.5 % and 4 % of the total energy intake. This observation shows that with only one serving of SSB per day, youths already complete half of the 10 % individual's daily calorie intake coming from added sugars (any sources of sugar, not only from beverages) recommended by the WHO (52).
In addition to SSB-related concerns, the very low water intake seen both in children and adolescents, especially at school, is particularly of concern knowing the importance of good hydration on cognition, especially when these subjects spend most of their day at school (24). Therefore, school-based interventions can play a key role in creating a water-friendly environment for children and adolescents (53). In a certain way, parenting role modelling and controlling home beverage availability may have an impact on the beverage intake behaviors of children (54) when some studies showed that when there were more SSBs available in the home or school environment, children also consume more (55-57). These specific drinking occasions and snack times, because of their low contribution to TFI, might suppose a window of opportunity for substituting water for SSBs and for adding water as a target for future nutritional interventions in young populations.
The most important strength of this study is that the method used to evaluate fluid intake was previously validated for accuracy and reliability (19), even if this validation was performed in an American adult population. Besides, the collection of 7-day records of fluid consumption, providing a representation of a full week and capturing all drinking occasions, may also be considered an important strength (19). A similar survey published in 2015 was also performed under similar conditions and during a similar period of the year, so both may be comparable (11).
However, there are also a number of limitations, mainly related to the data collection performed at school and the sampling method. For the majority of children, a parent was the person responsible for filling in the questionnaire, and thus it is likely that fluid intake at school was underestimated since children would need to be able to accurately report to their parents what they drank at school upon returning home. The questionnaire for measuring total daily fluid intake has been validated as accurate against a gold standard for water turnover (19), but this validation did not assess the accuracy of the questionnaire at specific locations. Inaccuracies between child recall and parent reporting may be one reason for the very low fluid intake reported at school; however, this low fluid intake is also consistent with other reports in several countries (58,59). The participants were recruited as being part of a database; only individuals having a telephone number were included. Therefore, very low socioeconomic groups could be underrepresented, which may be deducted from the distribution of educational levels among participating parents. Due to the methodology used, with parents/caregivers reporting intakes for children under 16 years of age, consumption may be under- or over-estimated. It should also be acknowledged that no biomarkers of hydration were measured, therefore no conclusions related to the hydration status of children are possible. Furthermore, the fact that the sample was not very large may also represent a limitation.
CONCLUSION
This study provides valuable information on fluid intake in a selected sample of Spanish children and adolescents. In combination with previously published data, this most recent survey reiterates the fact that a very low percentage of children and adolescents are drinking liquids adequately. This situation is especially relevant for adolescent boys whose consumption is similar to the one of their younger counterparts while their hydration needs are different. In parallel, the message of the importance of increasing water intake is a necessity as results showed children and adolescents drinking less water than previously with no change in SSB consumption. This behavior, at a time in life when consumption habits are defined that will persist into adulthood, may lead to an increased risk of developing overweight and obesity. It seems that there is a window of opportunity mainly at snack times and outside the meals for changing the pattern of drinking beverages by substituting water for SSBs or by just helping children and adolescents to drink more water at this specific occasions, as well as in other locations other than home. Future research should focus on longitudinal tracking of well-defined populations and study the influence of parental and peers modelling to determine those at higher risk and to provide adequate tools for prevention and intervention in order to slow down the current tendencies in drinking fluids among young population groups.

