










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
In children negative changes in lifestyle such as increased consumption of processed foods with low nutritional value and high calories, and decreased physical activity (PA) patterns have affected their mental and physical health as indicated by health-related quality of life (HRQoL) (1,2) and different psychological factors such as self-esteem (3,4). Unfortunately, self-esteem is associated with children's social, emotional, behavioral, and mental health, playing a vital role during childhood (5); low self-esteem has been strongly associated with different mental health diseases that affect childhood development (6). In contrast, high self-esteem has been associated with better cognitive development (7). Likewise, well-being is also an important factor, defined as a construct that encompasses all aspects of healthy and successful living, including psychological, physical, and other domains (8). Subjective well-being has been associated with immediate and long-term positive life outcomes including school, community factors, and social relationships with family and peers, which have a strong influence on the subjective well-being of children (9). In this way, the importance of emotional development has become a priority of education (10), as research has shown that social-emotional competence can be taught in schools and can make a positive difference in young people's lives (11).
On the other hand, healthy food habits generally have a strong participative role in the overall state of well-being including HRQoL (12). Evidence has shown that adherence to the Mediterranean diet (MD) is associated with positive effects on specific components of well-being and mental health (13). Likewise, children's food habits have an influence on health in later life, present associations with different factors of mental health (14), and can be protective factors for subjective well-being in children (15). Moreover, decreased PA and fitness, and increased sedentary behaviors such as screen time (ST) have been associated with a cluster of behavioral risk factors and negative mental health in children (3), this being considered a new variable in child and youth health (16). Additionally, PA and fitness have been indicated as an important factor to prevent physical and mental health (17) due to is modifiable nature. So, identifying modifiable lifestyle behaviors such as MD adherence and PA patterns linked to feelings and well-being is necessary to develop preventive strategies for schoolchildren. Therefore, the purpose of this study was to determine the association between healthy and unhealthy behaviors (i.e., MD, PA, ST, and fitness) with well-being in Chilean schoolchildren.
MATERIALS AND METHODS
This cross-sectional study included 615 schoolchildren, both girls (n = 271, 11.7 ± 1.00 years old) and boys (n = 344, 11.8 ± 1.1 years old) from different primary public schools in Chile, selected by convenience. Parents and guardians were informed about the study and provided their signed written consent for participation. Additionally, all children gave their written assent on the day of assessment. The investigation complied with the 2013 Helsinki Declaration and was approved by the Local Ethics Committee (ACT 086 2017).
Inclusion criteria were: i) informed consent of parents and assent of participant; ii) belonging to educational centers; and iii) between 10 and 13 years of age. Exclusion criteria included having a musculoskeletal disorder or any other known medical condition that might impair a participant's health and physical activity levels. Moreover, schoolchildren with physical, sensorial, or intellectual disabilities were excluded.
ANTHROPOMETRIC ASSESSMENT
Body mass index (BMI), calculated as body mass divided by the square of height in meters (kg/m2), was used to estimate the degree of obesity. Body mass (kg) was measured using a TANITA scale, model Scale Plus UM - 028 (Tokyo, Japan); the children were weighed in their underclothes without shoes, and height (m) was estimated with a Seca® stadiometer, model 214 (Hamburg, Germany) that was graduated in mm. BMI is shown according to the growth table of the Centers for Disease Control and Prevention (CDC), Overweight and Obesity, verifying the corresponding age and sex-related percentile. Child obesity is defined as a BMI equal to or greater than the 95th percentile, and overweight as a BMI equal to or greater than the 85th percentile among children of the same age and sex (18). Waist circumference (WC) was measured using a Seca® tape measure model 201 (Hamburg, Germany) at the height of the umbilical scar (19). The waist-to-height ratio (WtHR) was obtained by dividing WC by height, and was used as a tool for estimating the accumulation of fat in the central zone of the body following international standards.
MEDITERRANEAN DIET ADHERENCE
MD adherence was assessed by the Krece Plus test (20), which is a tool to assess eating patterns and their relationship with nutritional status based on MD. The questionnaire has 15 items, and the format assesses a set of items about the food consumed in the diet. Each item has a score of +1 or -1, depending on whether it approximates the ideal of MD. The total points are added, and according to the score, the nutritional status is classified as follows: i) low nutritional level: less than or equal to 5; ii) moderate nutritional level: from 6 to 8; and iii) high nutritional level: greater than or equal to 9.
SCREEN TIME AND PHYSICAL ACTIVITY AFTER SCHOOL
Lifestyle was evaluated with the Krece Plus test (20). The Krece Plus is a quick questionnaire that classifies lifestyle based on the daily average of hours spent watching television or playing video games as screen time, and the hours of PA after school per week. The classification is made according to the number of hours used for each item. The total points are added, and the person is classified as with a good lifestyle (men: ≥ 9, women ≥ 8), regular lifestyle (men: 6-8: women: 5-7) or bad lifestyle (men: ≤ 5 and women: ≤ 4) according to the lifestyle score.
PHYSICAL ACTIVITY
PA levels were measured using the Physical Activity Questionnaire for Children (PAQ-C) (21). In brief, the self-administered, 7-day recall questionnaire was comprised of nine items and collected information on participation in different types of activities and sports (activity checklist), and efforts and activities during lunch, after school, in the evening and over the weekend during the past 7 days. Each item was scored between 1 (low PA) and 5 (very high PA). To calculate the final score, the mean score of the nine questions was estimated, where “1” indicates low PA and “5” indicates very high PA. The 10-item PAQ-C asks participants whether they were sick last week or whether anything prevented them from doing normal PA.
PHYSICAL FITNESS
To evaluate the health-related physical fitness of children we used the ALPHA-fitness test battery (22). Lower-body explosive strength was assessed by a standing long jump test (SLJ), in which the child stood behind a marked line and jumped with both feet together as far as possible. Each child jumped twice, with the best result recorded. Higher scores indicate better performances. Cardiorespiratory fitness (CRF) was measured by the progressive 20 meter shuttle run test (20mSRT) (23). The participants were required to run between two lines 20 metres apart while keeping pace with audio signals emitted from a pre-recorded CD. The results were unified according to the Leger test protocol, and maximal oxygen consumption (VO2MAX) was calculated using Leger's equation. Handgrip strength, measured with a hand dynamometer (TKK 5101 Grip D; Takei, Tokyo, Japan) was used to measure upper body strength. The test consists of holding a dynamometer in one hand and squeezing as tightly as possible without allowing the dynamometer to touch the body; force is applied gradually and continuously for a maximum of 3-5 seconds. The test was performed twice, and the maximum score for each hand was recorded in kilograms. The average of the scores achieved by the left and right hands was used in the analysis. Higher scores indicate better performance.
WELL-BEING AND SOCIAL HEALTH
The KIDSCREEN-10 was used to measure HRQoL and well-being items. The questionnaire is a validated and widely used assessment tool, developed for monitoring global HRQoL in children and adolescents (8- to 18 year old). The KIDSCREEN-10 has 10 items, each answered on a five-point Likert scale indicating the frequency of a specific behavior or feeling (1 = never; 2 = almost never; 3 = sometimes; 4 = almost always; and 5 = always) or the intensity of an attitude (1 = not at all; 2 = slightly; 3 = moderately; 4 = very much; and 5 = extremely). The responses to items 3 and 4 (negatively formulated) were recoded to have scorings from 1 to 5, and the raw scores were used for different analyses, with higher values indicating a higher HRQoL (24). The question “Have you had a good time with your friends?” was used to determine “social health”.
SELF-ESTEEM
For measuring self-esteem we used the Coopersmith Inventory (25). The inventory has been validated in a Chilean children population (26). This self-reported questionnaire is designed to measure attitudes toward the self in a variety of areas (family, peers, school, and general social activities). The instrument is commonly used to assess self-esteem in both research and clinical practice, and higher scores reflect a higher self-esteem.
STATISTICAL ANALYSIS
The statistical analysis was performed using the SPSS v23.0 software (SPSS™, IBM Corporation, NY, USA). Normal distribution was tested using the Kolmogorov-Smirnov test. For continuous variables, values were presented as means and standard deviation (SD). Differences between sexes were determined using the one-way ANOVA. To determine the association between adherence to lifestyle, HRQoL, and self-esteem a multiple lineal regression was used. Values of p < 0.05 were considered statistically significant.
RESULTS
Table I shows anthropometric parameters, fitness, adherence to MD, and well-being according to sex. Girls reported lower CRF and handgrip strength values than boys.
Table I. Anthropometric parameters, fitness, adherence to MD, and well-being according to the study sample
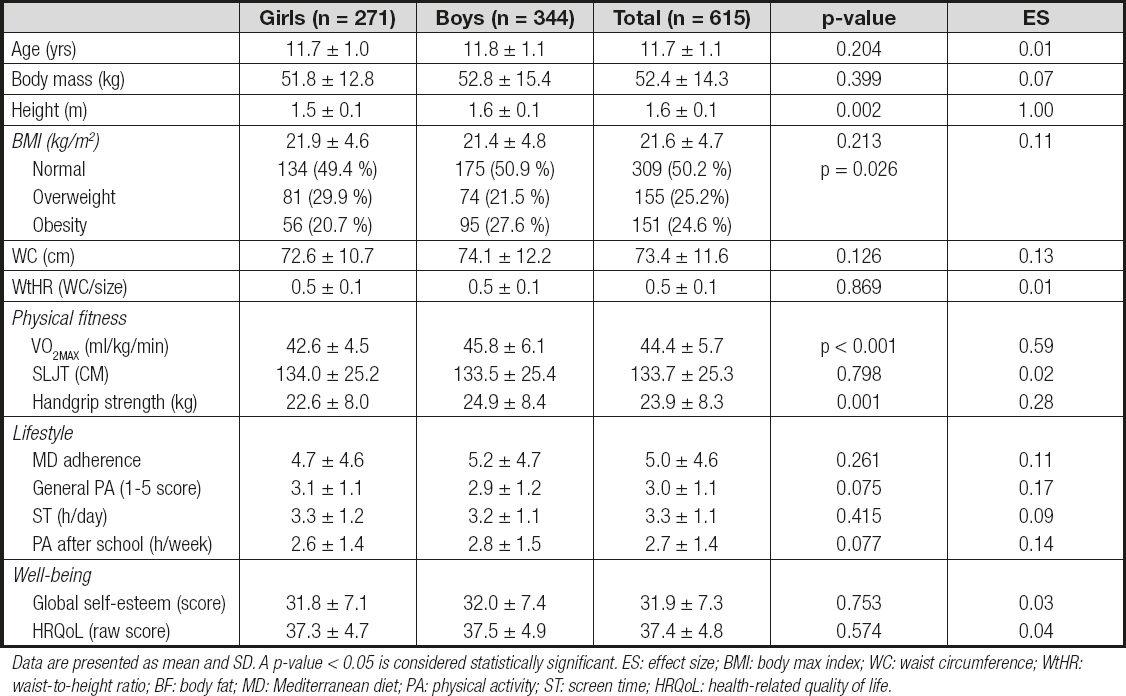
Data are presented as mean and SD. A p-value < 0.05 is considered statistically significant. ES: effect size; BMI: body max index; WC: waist circumference; WtHR: waist-to-height ratio; BF: body fat; MD: Mediterranean diet; PA: physical activity; ST: screen time; HRQoL: health-related quality of life.
Table II shows the multivariable lineal regression for each item of MD. HRQoL was linked to the items “Takes a fruit or fruit juice every day” (β: 1.93, 95 % CI: 0.63, 3.23, p = 0.004) and “Consumes fresh or cooked vegetables > 1 time/day” (β: 1.12, 95 % CI; 0.20, 2.05, p = 0.018). Self-esteem was associated with “Consumes a dairy product > 1 time/day” (β: 3.30, 95 % CI: 0.32, 6.28, p = 0.030). Social health was linked inversely to “Eats at a fast food restaurant ≥ 1 time/week” (β: -0.26, 95 % CI; -0.42, -0.09, p = 0.003) and positively to “Consumes pasta or rice almost every day” (β: 0.35, 95 % CI: 0.00, 0.70, p = 0.049).
Table II. Association between adherence to MD items and psychological well-being

data shown represent β, (95 % CI), p-value. A p-value < 0.05 was considered statistically significant (in bold).
Table III shows the association between physical status and psychological HRQoL with CRF (β: 0.12, 95 % CI: 0.06, 0.17, p < 0.001) and PA after school (β: 0.32, 95 % CI: 0.04,0.60, p = 0.023). Self-esteem was linked in an inverse way with ST (β: -1.35, 95 % CI: -2.04, -0.65, p < 0.001). Finally, social health presented a positive association with PA after school (β: 0.06, 95 % CI: 0.00,0.12, p = 0.037).
Table III. Association between physical status and psychological well-being
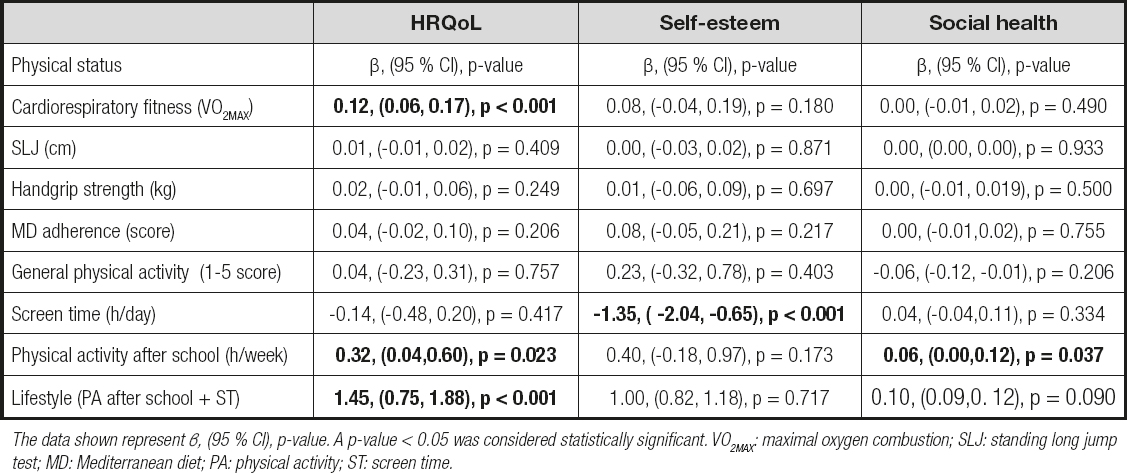
The data shown represent β, (95 % CI), p-value. A p-value < 0.05 was considered statistically significant. VO2MAX: maximal oxygen combustion; SLJ: standing long jump test; MD: Mediterranean diet; PA: physical activity; ST: screen time.
DISCUSSION
The purpose of this study was to determine the association of items of MD adherence, fitness components, and lifestyle with psychological and social health in Chilean schoolchildren. The main findings were: i) CRF and PA after school presented a positive association with HRQoL; ii) social health had a positive association with PA after school; and iii) “Eats at a fast food restaurant ≥ 1 time/week” presented an inverse association with “Had a good time with friends.”
In the present study PA after school was linked to HRQoL and social health in schoolchildren. Along these lines, evidence has shown that it is fundamental to understand that PA promotion should be emphasised to improve HRQoL in children (27). Similar to our results, another study conducted in American schoolchildren reported a positive association between PA, PF and HRQoL; moreover, PA was positively associated with subjective well-being (28). Additionally, the literature has reported that the highest level of PA at recess, lunchtime, and after school was associated with better HRQoL scores in Australian adolescents (29). Likewise, it has been indicated that the perception of self-reported fitness is associated with HRQoL and self-rated health in Portuguese adolescents (30). In this context, the findings of another study carried out in Malaysian children reported that children who are physically active have better HRQoL (27).
In the present study adherence to MD items showed an association with psychological and social health in schoolchildren; likewise, negative items such as “Eats at a fast food restaurant ≥ 1 time/week” was linked negatively to social health. In this same line, an investigation has reported that Japanese children with undesirable lifestyles, such as poor food habits, were more likely to have less well-being, regardless of sex, BMI, or social background (31). Likewise, a study that evaluated adherence to MD with HRQoL in Portuguese adolescents reported that adherence was positively associated with well-being (32). Moreover, a recent study carried out in Spanish schoolchildren concluded that adherence to MD was found to behave as a protective factor for positive well-being in a cross-sectional analysis (33). In this line, a study that evaluated the relationship between adherence to MD, HRQoL, and subjective happiness reported positive associations with adherence to MD, higher levels of subjective happiness, and better HRQoL in adolescents (13). Additionally, a previous study has reported that adherence to MD presented positive correlations with different factors of well-being (14).
In the present study ST was linked negatively to psychological health (i.e., self-esteem). Regarding our results, it has been reported that higher levels of ST are associated with poorer psychological and physical health in children (34). In addition, another study reported that ST was significantly associated with poor mental health outcomes, psychological distress, and low self-esteem in a sample of youth (35). Likewise, evidence has shown that ST has been linked to lower psychological well-being as well as decreased perceived HRQoL in schoolchildren (36). Similarly, a recent study carried out in schoolchildren showed that high exposure to ST increases the risk of emotional and behavioral problems (37). According to our results, evidence has shown that exceeding two hours of ST each day was associated with significantly lower well-being scores in Australian adolescents (29).
CRF was linked in a positive way to HRQoL. In this sense, a study carried out in Portuguese schoolchildren reported that HRQoL was positively associated with CRF and muscular fitness (38), both fitness components. Similar to the results of this present study, it has been reported that CRF has been positively associated with higher scores on all five KIDSCREEN-27 domains in a sample of schoolchildren (39). Moreover, another study indicated that children with high levels of fitness have a higher HRQoL when compared to children with low levels of fitness. Similarly, CRF has been associated with physical and emotional well-being in Spanish schoolchildren (40). Therefore, improving CRF and physical fitness components could be a good strategy for improving HRQoL in children.
In the present study we reported that self-esteem was linked with healthy patterns of MD such as “Consumes dairy products (> 1 time/day).” In this context, the findings of another study indicate that good food habits such as MD adherence were positively associated with self-esteem in Spanish adolescents (30). Similarly, evidence has shown that a higher healthy dietary adherence score at baseline in normal weight and overweight children was associated with better self-esteem (41). In contrast with our results, another study reported that higher self-concept was associated with lower consumption of dairy products; likewise, children classified as having “high self-esteem” reported higher consumption of fruit, vegetables, fish, nuts, and pulses (14). On the other hand, it has been indicated that an adequate intake of milk and dairy products seems to be an important factor for adolescents’ health (42).
LIMITATIONS
The limitations of the present study include those inherent to its transversal character. Another limitation would be self-reporting in relation to well-being, self-esteem, food habits, and PA, which could mean that these data are underestimated or overestimated. The strengths of this study are that we examined several variables that affect the psychological and social health of children, contributing to a better understanding of the serious problem of bad food habits such as eating fast foods or candies repeatedly among Chilean schoolchildren.
CONCLUSION
In conclusion, MD adherence items, fitness, and lifestyle (i.e., PA after school and ST) were linked to psychological and social health, therefore it is necessary to develop preventive strategies for schoolchildren to change in a positive way these modifiable lifestyle behaviors. This suggests that interventions for children need to begin early in order to establish healthy habits, as lifestyle habits acquired during childhood will persist into adulthood.

