










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Osteomalacia is characterized by abnormal matrix mineralization in established bone, and although present in children with rickets, it is used to describe bone mineralization defects after completion of growth (1). Myopathy manifested as proximal muscle weakness affecting the lower extremities has been described as a prominent feature of osteomalacia, which may be present even before biochemical signs of bone disease (2-3). Moreover, since the discovery of the vitamin D receptor in human muscle cells, studies conducted particularly among older adults have reported with conflicting results the relationship between 25-hydroxyvitamin D (25(OH)D) levels and muscle strength (4). Although some observational studies demonstrated a positive correlation between 25(OH)D levels and muscle strength (5-9), others did not (10-11). Despite these facts, relatively few studies have explored the relationship between vitamin D status and muscle strength in adolescents.
Previously, a cross-sectional study conducted in Chinese girls aged 12 to 15 years reported that serum 25(OH)D concentrations ≥ 20 ng/mL were associated with greater grip strength (12). Likewise, in the Young Hearts Study, boys 15-year-old with serum 25(OH)D levels > 20.4 ng/mL had significantly greater grip strength (GS) than those with 25(OH)D levels < 12.8 ng/mL. However, in the latter study, GS did not significantly differ across 25(OH)D levels among girls and 12-year-old boys (13). Given that muscle strength correlates with bone mass acquisition during adolescence, it is relevant to determine the effect of 25(OH)D levels on muscle strength during this critical period of musculoskeletal growth (14). Therefore, the present cross-sectional study aimed to examine the relationship between vitamin D status and grip strength in a nationally representative sample of adolescents.
METHODS
STUDY POPULATION
The present cross-sectional analysis was based on data from participants aged 10 to 19 years in the continuous National Health and Nutrition Examination Survey (NHANES) 2011-2012 and 2013-2014 cycles. The NHANES is designed to assess the health and nutritional status of adults and children in the United States (USA). A complex, multistage probability sampling design was used to select a sample representative of the civilian noninstitutionalized household population of the USA. The NHANES protocol was approved by the National Center for Health Statistics Research Ethics Review Board (study protocol # 2011-17). An informed consent was obtained from those who had reached the age of maturity in their State. A parent or guardian gave permission for minors to participate (15).
Characteristics of participants
Age, sex, and race/ethnicity were self-reported. The household reference person described the highest level of education obtained, and the ratio of family income to poverty was calculated as a measure of family's poverty status. In the interview file, sedentary lifestyle over the past 30 days was assessed by asking participants “How many hours per day did you sit and watch TV or videos? Self-reported general health was grouped as good to excellent and fair to poor. In the dietary interview component, participants' daily total protein intake was reported in grams. Standing height (cm) was measured using a stadiometer and a fixed vertical backboard. Moreover, participants' total percent fat mass and total lean mass (g), excluding bone mineral content, were measured using whole-body scans densitometers (Hologic, Inc., Bedford, Massachusetts, USA).
Vitamin D status
Total 25-hydroxyvitamin D (25(OH)D) is the predominant circulating form of vitamin D and is considered to be the most reliable index of vitamin D status. Total 25-Hydroxyvitamin D is the sum of 25-hydroxyvitamin D2 and 25-hydroxyvitamin D3, but excludes epi-25-hydroxyvitamin D3. The ultra-high performance liquid chromatography-tandem mass spectrometry (UHPLC-MS/MS) method was used for the quantitative detection of serum 25(OH)D. A complete description of the laboratory procedure manual is available at: https://wwwn.cdc.gov/nchs/data/nhanes/2011-2012/labmethods/VID_G_met_Vitamin_D.pdf.
For this analysis, 25(OH)D level in nmol/L was converted to ng/mL (1 nmol/L = 0.4 ng/mL). According to the American Endocrine Society guidelines, adolescents with 25(OH)D levels < 20 ng/mL were defined with vitamin D deficiency, those with 25(OH)D levels between 20 and 30 ng/mL represented vitamin D insufficiency, and those with 25(OH)D levels > 30 ng/mL were considered as having vitamin D sufficiency (16). Moreover, as indicated by the Institute of Medicine, subjects with serum 25(OH)D levels < 12 ng/mL were at risk of deficiency relative to bone health (17).
Muscle strength
A detailed description of the muscle strength procedure manual is available at https://wwwn.cdc.gov/nchs/data/nhanes/2013-2014/manuals/muscle_strength_2013. Briefly, muscle strength was measured using a handgrip dynamometer. Participants, while standing, squeezed the dynamometer as hard as possible. The exam was then repeated in each hand three times, with a 60-second rest between trials on alternating hands. The combined maximum GS, expressed in kilograms (kg) was calculated as the sum of the greatest reading for each hand. Those who were unable to hold the dynamometer with both hands or had any surgery in the hands/wrists in the prior 3 months were excluded for this analysis.
STATISTICAL ANALYSIS
The characteristics of participants were compared across vitamin D status using the Chi-squared and ANOVA tests for categorical and continuous variables, respectively. Sex-specific general linear models were assembled to examine the association between vitamin D status and combined maximum GS. The following covariates were included in the multivariate models: model 1 was adjusted for age and height, and model 2 was further adjusted for race/ethnicity, household reference person's education, ratio of family income to poverty, hours of sedentary lifestyle, self-reported health, total fat mass percent, total lean mas, and daily protein intake. The SPSS Complex Sample software, v.25 (SPSS Inc, Chicago, Illinois, USA) was used in all analyses to account for the NHANES complex survey design. A p-value < 0.05 was considered statistically significant.
RESULTS
A total of 2,528 adolescents with a mean age of 14.5 (SE: 0.07) years comprised the study sample. Table I shows the characteristics of participants stratified according to vitamin D status. In general, girls, non-Hispanic black, low income, higher total percent fat mass, sedentary lifestyle, and lower protein intake were characteristics associated with vitamin D deficiency. Overall, vitamin D deficiency, insufficiency, and sufficiency were prevalent in 25.6 %, 48.5 %, and 25.9 % of participants, respectively. Moreover, 4.1 % of adolescents were defined at risk of vitamin D deficiency relative to bone health. As shown in figure 1, the combined maximum GS was similarly distributed in both sexes among participants aged 10 to 12 years. Thereafter, GS progressively increased in boys, reaching a maximum strength of 88.7 kg at the age of 19 years. In girls, the increase in GS was less accentuated. However, between the ages of 13 and 19 years, GS increased by 9.8 kg in girls.
Table I. Characteristics of participants according to vitamin D status
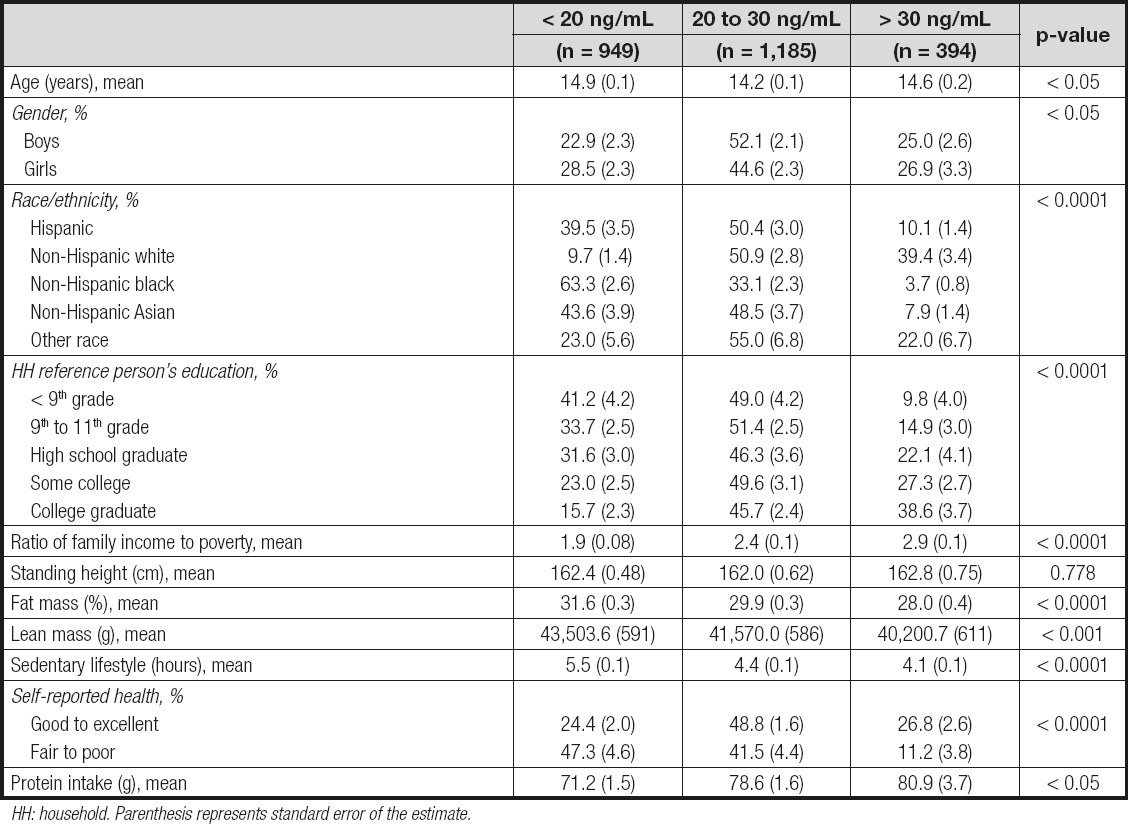
HH: household. Parenthesis represents standard error of the estimate.

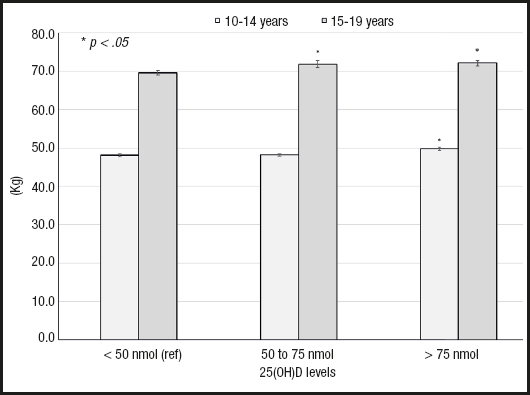
Table II shows the combined maximum GS stratified according to vitamin D status and sex. As expected, boys were consistently stronger than girls regardless of their vitamin D status. Notably, after adjusting for potential confounders, the combined maximum GS was on average 2.9 kg higher among boys with vitamin D sufficiency than their counterparts with vitamin D deficiency. Similarly, girls with vitamin D sufficiency were 2.1 kg stronger than those with vitamin D deficiency. Moreover, boys defined as having severe vitamin D deficiency were 4.1 kg weaker than those who did not. However, muscle strength did not significantly differ between girls with or without severe vitamin D deficiency (Table III). In a subgroup analysis, participants aged 15 to 19 years were considerably stronger than their younger counterparts, irrespective of their vitamin D status. However, according to age group, a similar difference in GS (1 kg) was seen between participants with vitamin D sufficiency and those with vitamin D deficiency (Fig. 2).
Table II. Combined maximum grip strength in adolescents according to vitamin D status and sex
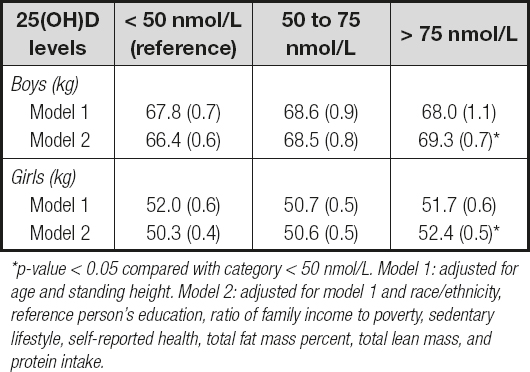
*p-value < 0.05 compared with category < 50 nmol/L. Model 1: adjusted for age and standing height. Model 2: adjusted for model 1 and race/ethnicity, reference person's education, ratio of family income to poverty, sedentary lifestyle, self-reported health, total fat mass percent, total lean mass, and protein intake.
Table III. Combined maximum grip strength in adolescents according to severe vitamin D deficiency and sex
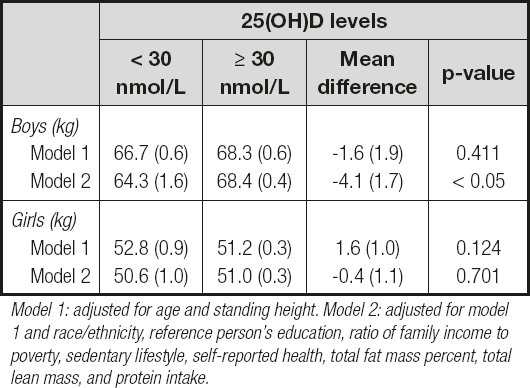
Model 1: adjusted for age and standing height. Model 2: adjusted for model 1 and race/ethnicity, reference person's education, ratio of family income to poverty, sedentary lifestyle, self-reported health, total fat mass percent, total lean mass, and protein intake.
DISCUSSION
The results of this cross-sectional study indicate that vitamin D status was significantly associated with muscle strength in adolescents. Notably, boys and girls with vitamin D sufficiency were significantly stronger than their counterparts with vitamin D deficiency. Moreover, boys at risk of vitamin D deficiency (< 12 ng/mL) relative to bone health were on average 4.1 kg weaker than those at no such risk. As expected, the combined maximum GS among adolescents markedly increased from age 12 years onward and boys were stronger than girls. The differences in muscle strength between age groups and sexes among adolescents have been explained by an age-dependent increase in fat-free mass and the anabolic effect of testosterone after puberty in boys (18,19). Nevertheless, even after adjusting for body composition, adolescents aged 15 to 19 years with vitamin D insufficiency and sufficiency were significantly stronger than those with vitamin D deficiency.
The present findings are consistent with those reported in a cross-sectional study among Chinese adolescent girls aged 15 years, in which participants with 25(OH)D levels ≥ 20 ng/mL had on average 1.8 kg greater GS than their counterparts with a poor vitamin D status (12). Similarly, in the Young Hearts Study, boys 15-year-old with 25(OH)D levels > 20.4 ng/mL had on average 3.8 kg stronger GS than those with 25(OH)D levels < 12.8 ng/mL (13). In addition, among girls in the HELENA study and a small study conducted among Ethiopian school children, serum 25(OH)D levels were significantly correlated with GS (20,21).
In contrast, a 7-year longitudinal study among girls aged 10 to 13 years recruited from schools in Central Finland reported no differences in muscle strength between participants with 25(OH) D levels < 20 ng/mL and those with higher 25(OH)D levels (22). Likewise, previous clinical trials designed to determine the beneficial effect of vitamin D supplementation on muscle strength have reported negative results. For instance, a small placebo-controlled study conducted among British men with a mean age of 22.7 years reported that participants supplemented with vitamin D 10,000 IU/day for 12 weeks achieved 25(OH)D levels > 48 ng/mL. However, these 25(OH)D concentrations did not improve the peak torque for maximal extension and flexion of the lower limbs as compared with the placebo group (23). Among Asian Indian females with a mean age of 21.7 years and a high prevalence of vitamin D deficiency at baseline, cholecalciferol 60,000 IU/week for 2 months, and then 60,000 IU twice per month for 4 months did not significantly increase grip strength at the end of the trial (24). Possible reasons for these contradictory results may be related to the age of participants, race/ethnicity, sample size, and a high prevalence of participants with vitamin D deficiency at baseline.
Although the physiological effects of vitamin D on muscle strength have not been completely elucidated, it was reported that 1,25-dihydroxyvitamin D3 increases calcium influx in muscle cells and may have a role in the regulation of muscle cell cytoskeleton protein synthesis (25). Moreover, Girgis et al. demonstrated that mice with deletion of the vitamin D receptor or diet- induced vitamin D deficiency were weaker than controls (26). Notably, cholecalciferol therapy has demonstrated to improve muscle mitochondrial maximal phosphorylation after exercise in individuals with severe vitamin D deficiency, which may partially explain the myopathy experienced by these subjects (27).
The present study has some limitations that should be mentioned. First, because of its cross-sectional design, the temporal relationship between vitamin D status and combined maximum GS may not be established. Second, the hand-grip strength was used as a proxy for overall muscle strength. However, unadjusted and weight-adjusted hand-grip strength has been reported to have a strong and moderate correlation with other muscle groups in children and adolescents, respectively (28). Whether vitamin D status has similar effects on total muscle strength among adolescents is uncertain. Third, although 25(OH)D cutoff levels defining vitamin D status were developed relative to bone health, it appears that vitamin D status may also be used to identify adolescents with muscle weakness. Finally, data on the participants' pubertal status and sex hormone levels were not included in this analysis. Despite these limitations, the study findings may be generalized to the adolescent population in the U.S.
CONCLUSION
In conclusion, vitamin D sufficiency was significantly associated with stronger combined maximum grip strength in adolescents. In contrast, boys with severe vitamin D deficiency were considerably weaker than their counterparts without deficiency. The present findings should be further explored to determine if maintaining optimal 25(OH)D levels might result in greater muscle strength in adolescents.

