










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Dietary indices are effective in assessing diet quality and the adherence of populations to dietary recommendations for food and nutrient consumption (1). In relation to micronutrients, epidemiological studies in Brazil reveal an inadequate consumption in children (2), adolescents (3), adults (4), and the elderly (5).
Knowing that inadequacy of micronutrient consumption is related to several chronic diseases (6), strategies that evaluate and ensure the adequacy of their consumption are of interest. Macronutrients have already been reported as important factors influencing adequacy of consumption for some micronutrients (7), and previous studies have evaluated both the quantity (8-10) and the quality (11-13) of carbohydrates in the diet as factors influencing adequacy of consumption of micronutrients. Recently, the evaluation of the quality of carbohydrates has been reported to be more relevant than the evaluation of its quantity (14). One of the methods for evaluating the quality of carbohydrates in the diet is by using the carbohydrate quality index (CQI) (11), which considers the amount of fiber, the glycemic index, and the relationship between the intake of whole grains and total grains as well as between the intake of solid carbohydrates and total carbohydrates.
Studies evaluating the relationship between the quality of dietary carbohydrates as measured by CQI and the consumption of micronutrients are scarce (11,15), as are studies that evaluate these variables specifically in women. In a study on women carried out by our research group (16), the micronutrients whose consumption was consistently associated with a CQI value were identified, but the relationship has not been thoroughly investigated.
Considering that adequate consumption of several micronutrients is associated with health benefits (17) and a lower risk of developing chronic diseases in women, such as breast cancer (18,19) and osteoporosis (20), it is important to assess the adequacy of micronutrient consumption in women since reports have shown their consumption to be inadequate in this group (21-23). It is also important to understand how the quality of the dietary carbohydrates that women consume can influence the adequacy of micronutrient consumption. Thus, the purpose of this study was to assess whether the quality of dietary carbohydrates, as measured using the CQI, is associated with adequacy of consumption for 13 micronutrients in a sample of women monitored by the Brazilian Unified Health System.
MATERIALS AND METHODS
STUDY POPULATION
This study examined data from the Prevendo Project: Health, Aging, Diet, and Inflammation, which was a cross-sectional study that aimed to develop, validate, and/or standardize instruments for use in the routine care of the Unified Health System (SUS) in Brazil. The Prevendo project was approved by the Human Research Ethics Committee of the State University of Ceará under protocol number 314.351, in accordance with the standards established by the Resolution No. 466/2012 of the Brazilian National Health Council. The study was conducted in accordance with the Declaration of Helsinki and all participants provided a written informed consent.
The study population consisted of women monitored by SUS who sought care at a health unit, which acts as a reference service in mastology in the SUS. In summary, 672 women were interviewed who met the inclusion criteria: consenting to participate in the study, age >18 years, absence of cancer in any anatomical site, absence of any disease that prevented participation in any stage of the study (for example, cognitive impairment), those on monitoring by the SUS, those who underwent mammography at the service, and those who were not pregnant or lactating.
DATA COLLECTION AND ANALYSIS
Data collection was carried out between 2016 and 2017, and included the application of a structured questionnaire containing questions regarding sociodemographic data (age, education, income, marital status, and self-declared color), lifestyle (smoking and food consumption), and anthropometrics (weight, body massindex (BMI) waist circumference, and percentage of body fat).
Age was recorded in complete years and used consistently. The level of education was defined as the years of completed study categorized as follows: ≤ 8 years of study, 9 to 11 years of study, and ≥ 12 years of study. Marital status was categorized into married and unmarried (because of the low number of women in other categories). The self-declared color was classified as white and nonwhite. Income was collected in minimum wages and classified as < 1, 1 to 3 and > 3. The prevailing minimum wage established by the Brazilian government at the time of data collection was US$ 185 (R$ 937). Smoking habit was categorized as smoker and nonsmoker (those who never smoked or had quit smoking).
ANTHROPOMETRIC ASSESSMENT
Anthropometric data were obtained according to the Center for Disease Control and Prevention protocol (24). Weight and height were obtained using a Filizola® scale with an attached stadiometer having a capacity of 200 kg (100 g range) and 2.00 m (1.0 cm range). BMI was calculated from these data and classified according to WHO recommendations based on the stage of life of the women (25).
Waist circumference (WC) was measured with an inelastic tape placed directly on the skin at the midpoint of the distance between the last rib and the iliac crest in a horizontal direction without causing skin compression. This was performed while the participant was standing with feet together, arms outstretched, and abdomen relaxed. WC was classified into adequate (< 88 cm) and elevated (≥ 88 cm) (25).
Body fat percentage (%BF) was assessed by ultrasound using the BX2000 (BodyMetrix Pro System, IntelaMetrix Inc.) with an established protocol that uses the anatomical points of measurement of the skin folds in the abdomen, triceps, and suprailiac region. %BF was classified into adequate (up to 32 %) and inadequate (> 32 %) (26).
ASSESSMENT OF FOOD CONSUMPTION
The participants were required to provide two 24-hour food recalls (R24h) on two nonconsecutive days, one being on a weekend. The first R24h was obtained at the time of the interview with the participant while the second was obtained through telephone contact or home visit. The interviews to obtain the R24h were performed by properly trained nutrition students and nutritionists.
Data were entered in a software developed to standardize the entry of food consumption data based on the first National Food Survey component of the 2008-2009 Family Budget Survey (27). After entry, the data were transferred to the Statistical Analysis System (SAS) to analyze nutrient compositions using the Table of Nutritional Composition of Foods Consumed in Brazil, which was prepared by the POF 2008-2009 (28). To reduce errors inherent to the methods of assessing food consumption, nutritional composition data were adjusted to remove intrapersonal variance using the Multiple Source Method (MSM), a statistical program available online to estimate the usual intake of nutrients and foods. A total of 13 micronutrients were analyzed which were as follows: zinc, selenium, magnesium, manganese, copper, phosphorus, vitamins A, E, D, thiamine, riboflavin, niacin, and pyridoxine. The adequacy of micronutrient consumption was determined by the cutoff point of the estimated average requirement (EAR). This is a simplified method of the probability method, which estimates the proportion of individuals with values below the EAR (29).
CARBOHYDRATE QUALITY INDEX
The CQI was applied to assess the quality of dietary carbohydrates. CQI considers the glycemic index, fiber content (quantity in grams), the relationship between whole grains (whole grains + products prepared with whole flour) and total grains (whole grains + refined grains + products prepared with whole and refined flours), and the relationship between solid carbohydrates and total carbohydrates (liquid carbohydrates + solid carbohydrates) in the diet (11).
Dietary liquid carbohydrates were estimated by the sum of carbohydrate values from sugary drinks and fruit juices, while dietary solid carbohydrates corresponded to the carbohydrate content of other foods with any carbohydrate content. In the CQI, the GI is analyzed continuously; however, we also categorize the diets into low, moderate, or high GI, where low GI ≤ 55; moderate GI = 56 to 69; and high GI ≥ 70. We also determined the glycemic load (GL), as the GL has a relationship with the GI, as well as with the consumption of micronutrients (12). The GL is calculated by multiplying the quantity in grams of the carbohydrate with the GI, divided by 100 (12). The GL was considered low if the value was < 80, moderate if between 80 and 120, and high if > 120. Each CQI criterion was scored from 1 to 5 and the values were added to determine the CQI, which varied from 4 to 20 points (Table I) (11). Based on their CQI values, the participants were divided into tertiles.

STATISTICAL ANALYSIS
Descriptive analyses were performed according to the tertiles of the carbohydrate quality index, with mean and standard deviation for continuous variables and percentage and a 95 % confidence interval (95 % CI) for categorical variables. ANOVA or Pearson's chi-square test were used to assess statistical significance between means and percentages, respectively.
Logistic regression analyses were performed to assess the association between the tertiles of the carbohydrate quality index (tertile 1 was considered as the reference) and the adequacy of micronutrient consumption (adequate consumption was considered as the reference). The models were adjusted for age (continuous), smoking habit (smoker or nonsmoker), marital status (married or not married), level of education (< 8 years, 9 to 11 years or > 12 years of study), GL of the diet (low, moderate, or high), and energy intake. Crude and adjusted odds ratios (ORs) were estimated with their respective 95 % CI and p-value. All analyses were performed using the R software, version 3.6.3. Values of p < 0.05 were considered statistically significant.
RESULTS
Of the 672 women interviewed, 24 were excluded for nonavailability of complete data, leading to a final count of 648 women evaluated in this study. Table II shows the characteristics of the women who participated in the study according to CQI tertiles. Women in the third tertile of the CQI were more likely to be unmarried, have a moderate/low dietary GL, and have a higher consumption of solid carbohydrates. The consumption of micronutrients increased in higher CQI tertiles, with the exception of selenium. No statistical difference was found between the CQI tertiles regarding the consumption of vitamin A and riboflavin. In addition, pyridoxine consumption values remained unchanged in the CQI tertiles.
Table II. Characteristics of women studied according to tertiles of Carbohydrate Quality Index. Fortaleza, 2020

Table II (cont.). Characteristics of women studied according to tertiles of Carbohydrate Quality Index. Fortaleza, 2020
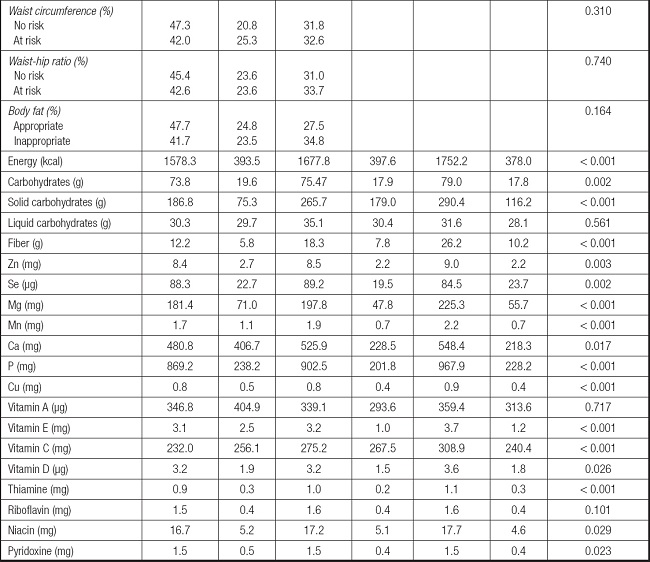
*ANOVA or Chi2 for means and proportions, respectively.
Table III shows the rates of inadequate consumption of micronutrients according to CQI tertiles. Women classified in the third tertile had a lower rate of inadequate consumption, except for magnesium and thiamine.
Table III. Percentages of inadequate consumption of micronutrients evaluated according to tertiles of the Carbohydrate Quality Index. Fortaleza, 2020

†Vitamin E, D and riboflavin have inadequate consumption above 90 %. Selenium less than 1 % of inadequacy, it is not possible to adjust models for these nutrients.
‡Total women with inadequate consumption. *Chi2 test.
In general, the micronutrients that demonstrated the lowest consumption rates were vitamin A, magnesium, manganese, and thiamine.
Table IV presents the crude and adjusted ORs of the logistic regression analyses for the micronutrients zinc, magnesium, manganese, copper, phosphorus, thiamine, and pyridoxine. It was not possible to perform a regression analysis for vitamin E, vitamin D, selenium, and riboflavin, as this would violate the applicability criteria of the logistic regression model considering that all women demonstrated low percentages of inadequacy (6 % and 2 % for selenium and riboflavin, respectively) or low percentages of adequacy (6 % for vitamin D) for these micronutrients and a rate of 99.9 % of inadequacy in consumption of vitamin E (data not shown).
Table IV. Crude and adjusted analysis of association between tertiles of Carbohydrate Quality Index with adequacy of micronutrient consumption. Fortaleza, 2020
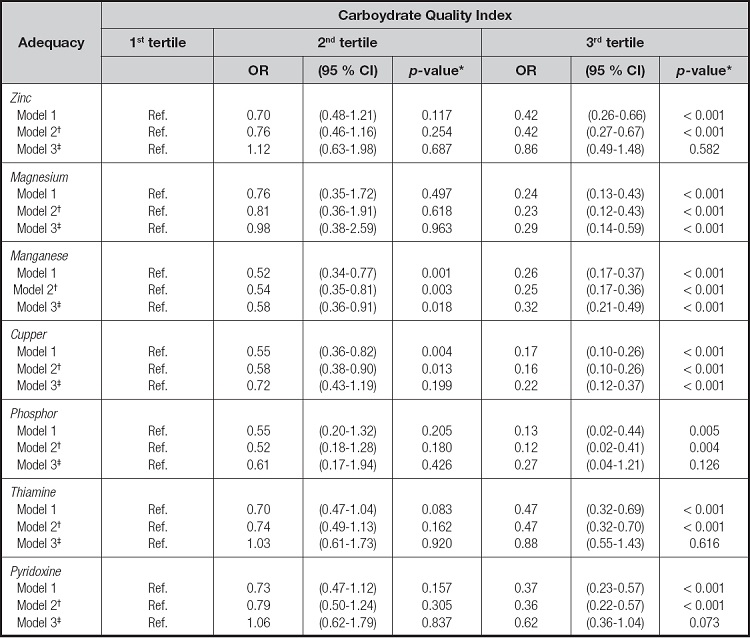
†Model adjusted for age (continuous), marital status, education, smoking and glycemic load of the diet.
‡Model adjusted by Model 2 and energy (kcal).
*Wald test.
In the evaluation of crude ORs using logistic regression models, women classified in the second tertile showed a lower prevalence of inadequacy in consumption of manganese (OR, 0.52; 95 % CI, 0.34-0.77) and copper (OR, 0.55; 95 % CI, 0.36-0.82), while women classified in the third tertile showed a lower prevalence of inadequacy for all micronutrients evaluated in the logistic regression (zinc [OR, 0.42; 95 % CI, 0.26-0.66], magnesium [OR, 0.24; 95 % CI, 0.13-0.43], manganese [OR, 0.26; 95 % CI, 0.17-0.37], copper [OR, 0.17; 95 % CI, 0.10-0.26], thiamine [OR, 0.47; 95 % CI, 0.32-0.69], and pyridoxine [OR, 0.37; 95 % CI, 0.23-0.57]).
After the first adjustment, adequacy of consumption of manganese (OR, 0.54; 95 % CI, 0.35-0.81) and copper (OR, 0.58; 95 % CI, 0.38-0.90) remained inversely associated with women in the second CQI tertile. In women classified in the third tertile, the significant inverse associations continued with p < 0.001 for all micronutrients except phosphorus (OR, 0.12; 95 % CI, 0.02-0.44). There were no changes in the ORs of the third tertile in the adjusted model compared with those in the crude model.
In the final adjustment model (adjusted by model 2 and energy intake), only consumption of manganese remained significant (OR, 0.58; 95 % CI, 0.35-0.91) in the second CQI tertile, while in the third tertile, consumption of magnesium (OR, 0.29; 95 % CI, 0.14-0.59), manganese (OR, 0.32; 95 % CI, 0.21-0.49), and copper (OR, 0.22; 95 % CI, 0.12-0.37) remained strongly significant (p < 0.001).
DISCUSSION
This study evaluated the association between the quality of dietary carbohydrates and the adequacy of micronutrient consumption in a sample of women monitored by the SUS. Adequacy of consumption of the minerals magnesium, manganese, and copper was inversely associated with the quality of dietary carbohydrates in women classified in the third tertile of the CQI after final adjustments using the regression models.
In this study, the micronutrients with the highest prevalence of inadequate consumption were vitamin A, magnesium, manganese, thiamine, copper, pyridoxine, and zinc. These findings are consistent with the previous reports on micronutrient consumption inadequacy in the Brazilian population (4-5,30).
Most previous studies have sought to identify factors associated with adequate micronutrient consumption (31-33), while few studies have focused on investigating the dietary patterns (34), and diet quality (35) as a means of determining the adequacy of micronutrient consumption. In a previous study (16) carried out by our research group, micronutrients whose consumption was consistently associated with the CQI value were identified, but this relationship has not been thoroughly investigated. Thus, in the current study, we sought to understand the relationship of CQI with the adequacy of micronutrient consumption using logistic regression models properly adjusted for potential confounding variables. Therefore, we found that women classified in the third tertile of the CQI, who had the highest CQI values, had a lower prevalence of inadequate consumption of magnesium, manganese, and copper in all three models, including the crude and adjusted ones, and lower prevalence of inadequate consumption for zinc, magnesium, manganese, copper, phosphorus, thiamine, and pyridoxine in the crude models after adjusting for the variables of age, education, marital status, and GL in the diet.
Previous studies (11,15) that assessed the relationship of CQI with the adequacy of micronutrients found that individuals in the largest quintiles of CQI were less likely to have inadequate consumption of micronutrients. However, these studies assessed the inadequacy of micronutrient intake in two ways: one assessed the chance of failing to meet four or more DRI recommendations (> 4 DRI) and failing to meet eight or more DRI recommendations (> 8 DRI) according to CQI quintiles (11), while the other study assessed the chance of not meeting six or more DRI recommendations (> 6 DRI) and eight or more DRI recommendations (> 8 DRI) also according to CQI quintiles (15). Both studies were performed in the Europe population. In our study, we aimed to investigate the relationship of each micronutrient with the tertiles of the CQI, and we found that those women in the third tertile in the CQI were less likely to have inadequate consumption for magnesium, manganese, and copper, after adjustments to the regression model.
The carbohydrate consumption in grams was similar in all tertiles, ranging from 74 to 79 g, suggesting that the quality of dietary carbohydrates may have been the factor that contributed to the adequacy of micronutrient consumption. Women in the third tertile had a higher consumption of solid carbohydrates; this can be explained by the fact that solid foods generally have a low GI, good fiber content, and micronutrient composition, and include foods such as fruits, vegetables, and cereals (36). Liquid carbohydrates, which are usually in the form of sugary drinks such as sweetened soft drinks and fruit juices, are less nutritious and have a high GI (14,36).
Regarding the components of CQI and the adequacy of micronutrients, there are studies that have assessed the relationship between GI and the adequacy of micronutrient consumption. These studies found that individuals with diets containing a high glycemic index are more likely to have inadequate consumption of several micronutrients (12,13,37). A study with children and adolescents in Australia showed that individuals who exceed 20 % of the total energy intake from free sugar consumption are more likely to have inadequate consumption of micronutrients (38), while a study using NHANHES data from 2009-2014 (39) found a significant association between the intake of added sugars and the percentage of the population below the EAR for only 3 of the 17 micronutrients evaluated: calcium, magnesium, and vitamin D.
Over time, assessment of the quality of dietary carbohydrates has become more relevant than assessment of their quantity (14). Thus, increased consumption of sources of carbohydrates with added sugar and sugary drinks is known to be associated with obesity, diabetes, cardiovascular diseases, and inadequate micronutrient consumption (10,40). In contrast, foods such as fruits, vegetables, whole grains, and tubers are options for sources of good quality carbohydrates, which also have favorable micronutrient compositions (14). Thus, the CQI is an instrument that captures different dimensions of dietary carbohydrates by evaluating GI, fibers, liquid carbohydrates, whole grains, and other characteristics of carbohydrates. The CQI can be quite useful, as it evaluates the characteristics of the carbohydrates in the diet in a more holistic way.
Despite the promising results, the present study has some limitations. The data used here were obtained using a cross-sectional design, and it was thus not possible to evaluate temporal sequences. In addition, the assessment of food intake was susceptible to measurement errors; although adjustment measures like training of interviewers and removal of intrapersonal variance were adopted, there may still have been inaccuracies in the consumption data. Another limitation of our study is that we did not collect information on the use of dietary supplements.
We observed that the participants had an inadequate consumption of most of the micronutrients evaluated. However, those in the third tertile of the CQI demonstrated a higher prevalence of adequacy, showing that the quality of carbohydrates was correlated to the adequacy of consumption of micronutrients, especially magnesium, manganese, and copper, when potential confounding variables were controlled. Thus, we believe that the CQI is a promising tool in the evaluation of quality in dietary carbohydrates given its ease of determination, allowing the assessment of dietary adequacy to aid in the prevention and control of many diseases and conditions in which food is an important factor.
In conclusion, the results of the study demonstrated that higher CQI values were associated with improved adequacy in the consumption of most of the micronutrients evaluated in the women monitored by the SUS, with emphasis on magnesium, manganese, and copper, after performing necessary adjustments using regression models. Our findings suggest that CQI can be a useful tool for assessing the quality of dietary carbohydrates and for identifying inadequacies in micronutrient intake. Moreover, the estimation of CQI highlights the relevance of an increased consumption of whole grains and fibers and a decreased consumption of added sugar in ensuring adequate micronutrient consumption, in addition to a reduction in the health risks associated with dietary intake of excess sugar and simple carbohydrates.

