










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Chile has one of the highest childhood obesity rates among countries belonging to the Organization for Economic Cooperation and Development (OECD), as half of preschool children are either overweight or obese, with boys having a higher prevalence (1).
The causes of childhood obesity can be categorized into biological, cultural, social, environmental, and psychological ones. Among the biological aspects, birth weight, breastfeeding, and sleep duration have been associated with childhood obesity. Stock et al. (2), in a study that assessed different time points during infancy and early childhood associated with overweight in adolescence, showed that “a greater than expected weight gain at any time in the first years of life was associated with increased BMI in adolescence, and that the effect was strongest after the first year”.
Breastfeeding duration has been found to be protective of childhood obesity. Ma et al. (3), in a cross-sectional study that included 9-11-year-old children from 12 countries, reported that exclusive breastfeeding was associated with lower odds of both obesity and high body fat compared to children who received exclusive formula feeding, independent of breastfeeding duration. With respect to sleep duration, Felso et al. (4), in a recent systematic review including 30 studies, concluded that there was an association between short sleep duration and insulin resistance, sedentarism, and unhealthy dietary patterns.
Of the social factors, the most important one is association with socioeconomic status, usually determined through family income, and parental education and occupation (5). Children whose parents have a lower educational level and/or are unemployed are more likely to have less healthy habits (6). In addition, a lower educational level has been associated with food insecurity, which can co-exist with overweight in low-income children. The potential reasons why low-income and food-insecure children may also be obese include increased intake of cheap, energy-dense foods (7), and/or parents giving their children more food than needed when food is available (8).
An important risk factor that can be regarded as social, cultural, and environmental is physical inactivity which has been shown to be inversely correlated with childhood obesity (9). Sedentary behavior due to increased screen time as well as “lack of physical movement” during school and after school have been shown to be associated with childhood obesity (10).
The role of grandparents has also been described as a potential risk factor of excessive weight gain (11), as they may influence both what children eat (12) and their physical activity level, which can be related to their own health problems and/or security concerns (11,13).
Although, in Chile, excessive weight gain begins in early infancy and is associated with the mother´s pre-pregnancy weight, gestational weight gain, feeding practices, sedentary behavior, etc. (14), and because preventive measures have not yielded positive results (15) and obesity continues to increase, we consider it important to determine if certain biological and social attributes observed when children begin prekindergarten (PK) at 4 years constitute risk factors for later obesity. The results of this analysis may contribute evidence to design special targeted interventions for preschool children with the aim of lowering obesity rates by mid-childhood, when metabolic problems arise as a consequence of obesity (16).
Thus, the aim of this study was to determine the risk of children being obese in 5th grade (10 yrs) according to some biological and social attributes observed when the same children attended prekindergarten (PK) at 4 yrs, so as to determine which specific group of children in PK should be prioritized for targeting. Interventions addressing this group of children may lead to a reduction in obesity prevalence by mid-childhood.
MATERIALS AND METHODS
STUDY DESIGN
This was a retrospective cohort study including 55,623 children when they were 10 yrs, and observed retrospectively when they were 4 yrs of age. The anonymized database was obtained from the Junta Nacional de Auxilio Escolar y Becas, an agency belonging to the Ministry of Education. This agency is in charge of the annual census of anthropometric, socio-demographic, and health variables of children in PK (4 yrs), kindergarten (5 yrs), first and fifth grades (6 yrs and 10 yrs, respectively) from all public schools in the country. The database for this study included children with anthropometric data in PK in 2012, as well as in 5th grade in 2018, plus some social characteristics collected at baseline. These included mother employment (occupied/not occupied), mother schooling, child relationship with persons living at home, person in charge of the child after school, and number of persons living in the same household. These variables originate from a survey administered by the head teacher to the mother or person in charge of the child (17). Trained physical education teachers measured weight and height in their students.
PARTICIPANTS
In Chile, 85 % of all students attend public schools. In 2012, around 78 % of PK children in public schools had socioeconomic and anthropometric data available (18); however, the % with valid data was 65 % (83,267), the baseline population for this study (Fig. 1). Of these, 16,277 were not measured in 5th grade. After excluding non-plausible anthropometric data in both time points, and including children with all the variables, the final population was 55,623 children.

VARIABLES
We considered the following variables collected at baseline: age, sex, weight, height, maternal educational level (≤ 8, 9-12, and > 12 yrs), maternal employment status (with/without), mutually exclusive categories showing relationship of the child with persons living in the same household (living with both parents and siblings, only mother, and presence of a grandparent), person in charge of the child after school, and number of household members (< 5 and ≥ 5), as indicated by Mota-Sanhua et al. (19).
We also considered weight, height, and age when the child attended 5th grade. Overweight and obesity were defined according to BMI for age and sex, using the 2017 WHO Standard (20).
STATISTICAL ANALYSES
We describe the variables when the children attended PK as relative frequencies (%), absolute frequencies, mean and standard deviation, separately for boys and girls. We determined if there was a significant difference between each variable by sex using relative frequencies for all comparisons except BMI Z-score, for which we used a t-test; p < 0.05 was considered significant in all comparisons.
We did two logistic regression models and determined goodness of fit with Hosmer-Lemeshow, calculating the risk that children in PK (all of them) have for developing obesity in 5th grade as OR (95 % CI). Both models included: mother education and occupation, person that takes care of the child after school, child relationship with persons living in the same household, and sex, while the second model considered in addition the presence of obesity in PK. Both models were adjusted for birth weight and number of household members. We determined 2 models in order to show that the variables included do not change if the model is adjusted or not by the presence of obesity in PK. STATA 16.1 was used. A p < 0.05 was considered significant.
The study was designed and conducted in accordance with the principles of the Declaration of Helsinki. It was reviewed and approved by INTA´s Ethics Committee of the University of Chile.
The database is anonymized, so there was no need to obtain consent to participate. The study was approved by INTA, University of Chile´s Ethics Committee. (Nº 14, December 16, 2020).
RESULTS
The flow diagram of participants is presented in figure 1; the final population corresponds to 66.8 % of the children included at baseline. Although a significant proportion of children did not comply with the inclusion criteria, when we compared the mean BMI Z-scores of included and excluded children in PK (with plausible anthropometric data, using t-test) we found no significant differences (p = 0.07).
Table I shows the description of anthropometric variables and some social characteristics when the children attended PK.
Table I. Nutritional status and some variables associated with obesity in children attending prekindergarten, by sex.
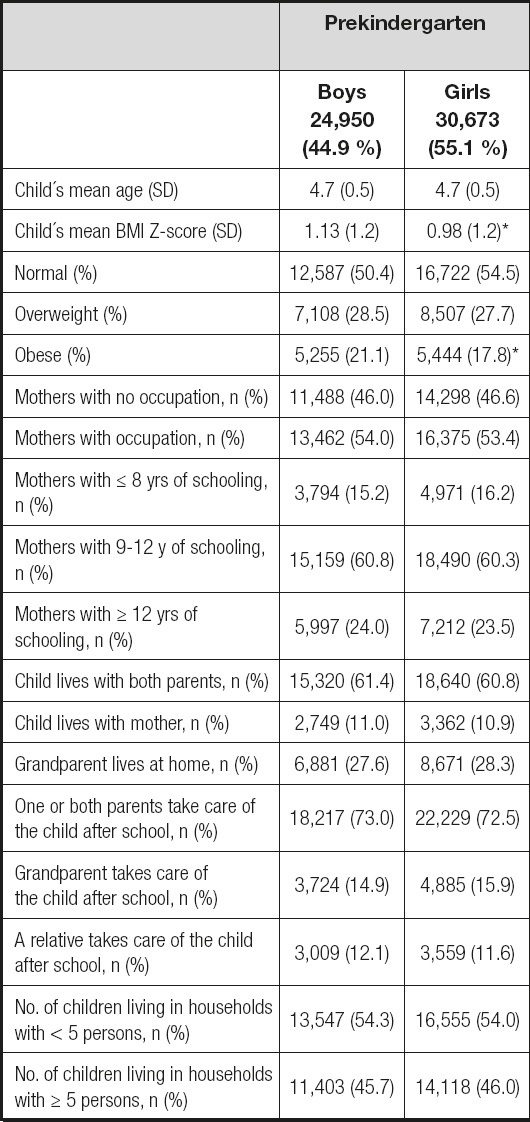
*p < 0.05 between boys and girls.
The prevalence of overweight and obesity, as well as the mean BMI Z-score in both sexes was very high; the latter two were significantly higher in boys. Slightly more than half of the mothers had an occupation, one quarter had higher education, and 60 % of the children lived with both parents, whereas in 25 % of households a grandparent lived at home, with over half of them being in charge of the child. Apart from the prevalence of obesity and mean BMI Z-score, there were no significant differences in social characteristics by sex.
The prevalence of obesity in 5th grade was very high—34.4 % and 22.7 % for boys and girls, respectively. Not only was prevalence significantly higher in boys, but also the rate of increase during the period—13.3 and 5 percentage points in boys and girls, respectively (not shown).
Table II shows the results of two logistic regression models to determine the risk of developing obesity in PK children when they reach 5th grade. The results from the first model show that the risk was 1.43 times higher in children whose mothers had ≤ 8 yrs of schooling and 1.16 times higher if mothers had 9-12 yrs of schooling. The presence of a grandparent also increases the risk by 1.13 times, whereas in children whose mothers had an occupation the risk increased slightly (1.04 times). Boys have a significantly higher risk (1.74 times).
Table II. Regression models to determine obesity risk in 5th grade, according to characteristics observed in the same children in prekindergarten.

*p < 0.05;
aAdjusted by birth weight and number of persons living in the same household.
The second model shows that if a child was obese in PK, the risk of being obese in 5th grade was 5.3 times greater than for a non-obese child. The OR for the other variables were similar than those observed in the first model, although in this model, children whose mothers had an occupation did not show an increased risk.
DISCUSSION
The main results of this study showed that being obese at 4 years is the greatest risk factor for obesity at 10 years; the likelihood is 5.3 times higher than for a non-obese child.
However, there are also other important risk factors such being a boy, having a mother with a low educational level and living with a grandparent.
As observed in our study, an increased risk of obesity in mid childhood if maternal education is low has been documented in a study of European children whose aim was to assess if low maternal education was associated with overweight and obesity risk at 4-7 years of age among children born to mothers with low versus high education. The authors found that low maternal education constituted a high risk of early childhood adiposity with a mean risk difference of 7.78 % in early childhood overweight between the groups (21).
One of the possible mechanisms by which low maternal education is associated with increased obesity is through inadequate feeding styles as shown by Saxton et al. (22). The authors assessed four aspects of feeding style: control, emotional, instrumental and encouragement/prompting to eat, applying the Parental Feeding Style Questionnaire to 180 mothers. The results showed that mothers with low education had significantly lower scores in control over feeding and significantly higher scores for emotional feeding, suggesting that these aspects may negatively influence diet quality and quantity among children.
A higher prevalence of obesity in boys has been reported in several studies. In Canada, Poland and China, over a 25-year period (1985-2010) the prevalence has been consistently higher among boys aged 7-18 (23). In the USA, results from 2 nationally representative cohorts of US kindergarten-aged children showed a nearly 20 % increase in obesity prevalence (11.6 % to 13.9 %), from 1998 to 2010, similarly for boys and girls, however the prevalence was higher among boys (24).
A higher prevalence in boys can probably be attributed to both sociocultural (25) and biological factors, which may begin as early as the fetal and postnatal periods with females generally having greater “fat mass and less fat-free mass, which is in turn associated with less energy intake and lower calorie needs for females than males” (26). Also, females exhibit higher circulating concentrations of leptin, a hormone that is related to fat mass and thereby adiposity (27).
The relation between maternal employment and childhood obesity is unclear (28). Studies from the USA, Canada, Germany, Japan, Spain, and the UK have shown a positive association while others in Australia, China and Denmark have shown no association. These conflicting results reported in rich countries (except China) are probably influenced by the characteristics of the labor market, such as the proportion of women in the work force as well as working hours (29).
In our study, maternal employment showed a small risk of obesity. However, when we included the presence of obesity in PK in the model, maternal employment no longer constituted a risk factor.
In our study, preschool children living with a single mother did not have an increased risk of obesity at 10 years of age; however, some studies have shown the opposite, such as one that analyzed the US Kindergarten Cohort of the Early Longitudinal Study. In determining the effect of the number of parents and siblings on the BMI trajectory from kindergarten through fifth grade, the study showed that children living with single mothers were more likely to be obese than were children living with 2 parents (26 % versus 22 %) (30).
Although our data indicated that predominantly parents looked after the child, more than half of the mothers had an occupation, so probably grandparents played a role in child upbringing. There is evidence that some grandparents may use unhealthy feeding practices to regulate emotions (31), using food as a reward (32) and pressure to eat (33), as well as influencing the child´s physical activity level (11).
In Chile, there have been numerous interventions to prevent childhood obesity at the national as well as local levels. The network of primary health centers covers around 75 % of the children aged 0-6 yrs in the country; as part of the regular health check-ups in that age group, the norm states that obese children (starting at 2 yrs) should attend two educational sessions with a nutritionist and in case they also present a risk factor such as insulin resistance, they will be seen by an MD (34). In general, this program has been regarded as efficient because over the years it has complied with the norm in terms of process, that is, educational sessions by nutritionists have been carried out and budget allocated for this activity has been spent accordingly; however, this intervention has not resulted in a reduction of obesity rates (35). Also, as part of primary health, the Vida Sana Program was implemented in 2011 with the goal of reducing the incidence of risk factors for developing diabetes and hypertension in adults and children. The Vida Sana Program (PVS) underwent an evaluation, published in 2020, which concluded that the contribution of PVS activities in 2017 to improving the nutritional status and fitness of children and adolescents (6-19-year-olds) was small, as only half of the participants showed improvement after 6 months of intervention (36). In 2013, the Elige Vivir Sano Program (Choose a Healthy Lifestyle) was implemented and still remains in place. The goal of this intervention is to promote a healthy lifestyle for all family members. It includes the following components: health communication, health education, social marketing, and physical activity (37). A report based on 2019 data concluded that this program could not be evaluated because the goal was not stated and that the process indicators did not comply in terms of quality and relevance (38).
Based on these evaluations it is fair to conclude that in spite of the interventions implemented addressing obesity in childhood, these have not been effective, and the prevalence has increased in all age groups (39).
This study ratifies the high prevalence of obesity among Chilean preschool children. We show that in addition to obesity at a young age, three other characteristics, that is, being a boy, having a mother with low education, and having a grandparent living at home are significant risk factors for obesity in mid-childhood. A strategy to reduce obesity rates in mid-childhood could be to prioritize this specific group of preschool children by intensifying the already existing intervention at the health centers. Because of its wide coverage, this strategy has a higher likelihood of implementation and could lead to a decrease not only in obesity by mid-childhood, but also in children developing chronic diseases such as metabolic syndrome and hypertension (40).
The most important strength of this study is its large population (55,623) of PK children followed for 6 years. Also, these results may be extrapolated to around 65 % of 4-year-old children attending public schools in Chile (18).
This study has limitations. It is based on secondary data and there was a loss of almost 20 % of anthropometric data, as these were not collected in 5th grade. In spite of that important loss, the anthropometric measurements are considered to be valid, as shown in a study that compared the data to those determined by trained personnel (41). In addition, the prevalence of overweight and obesity determined by this study are very similar to the ones obtained from other studies that included children of the same age group (14,42).
We only explored certain variables in PK from the survey because of missing data, especially those related to father characteristics, which may be potential risk factors. Other variables, namely, dietary intake, sedentary behavior, and TV time are not collected by the survey.

