










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Resilience has been conceptualized in a multitude of ways, however, current views of resilience focus on the multidimensional nature of this construct, emphasizing that it is both dynamic and multi-systemic (Masten & Narayan, 2012). Following Ungar (2013) resilience is viewed as the capacity of individuals to overcome adverse situations to navigate their way to the psychological, social, and physical resources that sustain their well-being. It is also studied even from a transcultural perspective (Coronado-Hijón, 2017). Recent studies report that, in situations where a disastrous event occurs, the way survivors cope with its consequences will depend both on external (community support) and internal resources (personal resistance) (Rahiem, Krauss, & Rahim, 2018). In relation to the protective factors of resilience, they are considered to be made up both of individual characteristics (e.g., self-efficacy or personality traits) and external factors (e.g., interpersonal relationships and support level) that balance the risks to which individuals are exposed (Rutter, 2012). Most people can recover optimally from and adapt to stressful life events through the effect of protective factors (Bolton, Praetorius, & Smith-Osborne, 2016; Dias & Cadime, 2017; Hamby, Grych & Banyard, 2018).
Resilience assessment, both for the general population and for clinical populations, requires valid measuring instruments with good psychometric properties. In the review conducted by Windle, Bennett, and Noyes (2011), 15 instruments that assessed resilience were identified, but only three of them presented adequate psychometric properties; the other questionnaires had many deficiencies requiring additional validation. In addition, some studies of the measurement of resilience have found some inconsistencies between the risk factors and the protective processes of resilience (Luthar, Cicchetti, & Becker, 2000). Protective factors contribute to individuals' good functioning despite the fact that exposure to stressful experiences could pose a significant risk for the development of a psychopathology (Hjemdal, Fribourg, Stiles, Rosenvinge, & Martinussen, 2006). That is why Lee et al. (2013) believe that, to improve resilience, it is more effective to promote protective factors such as self-efficacy, positive affect, social support, or self-esteem than to reduce risk factors.
Despite the enormous importance of resilience for the individual, there are few instruments to measure it in Spanish that can be applied to both to the general and the clinical population. Among the resilience questionnaires adapted and validated in Spanish are the CD-RISC (Crespo, Fernández-Lansac, & Soberón, 2014) and the BRS (Rodríguez-Rey, Alonso-Tapia, & Hernansaiz-Garrido, 2016). The former evaluates a series of internal individual resources that facilitate recovery, such as personal competence or positive acceptance of change by the individual, among others. And the latter one assesses resilience as an outcome, that is, the ability to recover from a stressful event.
However, there is currently no valid and reliable measure of resilience that includes both internal protective and external factors and that can be applied to the general Spanish population (Dias & Cadime, 2017). Drawing on research of the importance of protective factors in resilience, the Protective Factors for Resilience Scale (PFRS) (Harms, Pooley, & Cohen, 2017) emerges. The authors used a sample of university students to study the factor structure of the scale and a second sample of the community population to confirm it. Different factorial models were analyzed, and authors concluded that, following the definition of resilience proposed by Pooley and Cohen (2010), the best one was that included a personal factor and two external factors related to family and peers; and due to the degree of association between the factors, an overarching construct was explained. Therefore, the factorial structure of the PFRS scale was the 3-order-second factor model. This scale consists of 15 items with a seven-point Likert response scale ranging from 1 (totally disagree) to 7 (totally agree). It presents a model with 3 subscales of five items each: Personal Resources (PR), Family Resources (SR-F), Peer Resources (SR-P). High scores indicate high resources on each of the subscales. The scale showed a high Cronbach alpha coefficient .93, moreover, relations between different variables (coping style, self-esteem and life satisfaction and the scores of the PFRS provided good evidence of the construct validity.
In cancer patients, Harms et al. (2019), have confirmed the same factorial structure, obtaining a Cronbach coefficient of .96, a root mean square error of approximation (RMSEA) of .06; a comparative fit index (CFI) of .99; a standardized root mean square residual (SRMR) of .07; and a goodness-of-fit index (GFI) of .99. The PFRS questionnaire has not yet been validated in Spanish population and there is also no instrument of similar characteristics to assess resilience in this language. The progressive interest in resilience, both for the complexity of its construct and the factors that form it, requires scientific research to focus on the adaptation and reliable validation of instruments to evaluate it, given the protective effect of resilience in different populations (Cronly et al., 2019; Ellis, Bianchi, Griskevicius, & Frankenhuis, 2017; Lee et al., 2017).
Therefore, our goal was to examine the factorial structure of the Protective Factors for Resilience Scale (PFSR) in two Spanish populations, community population and population with chronic disease (understood as long-term and usually slow-progressing diseases).
Method
Procedure
Back-translation of the questionnaire was carried out. Two studies were subsequently conducted. In the first study, the instrument was applied to a sample of Spanish community population; in the second study, it was applied to a sample of Spanish people with chronic diseases.
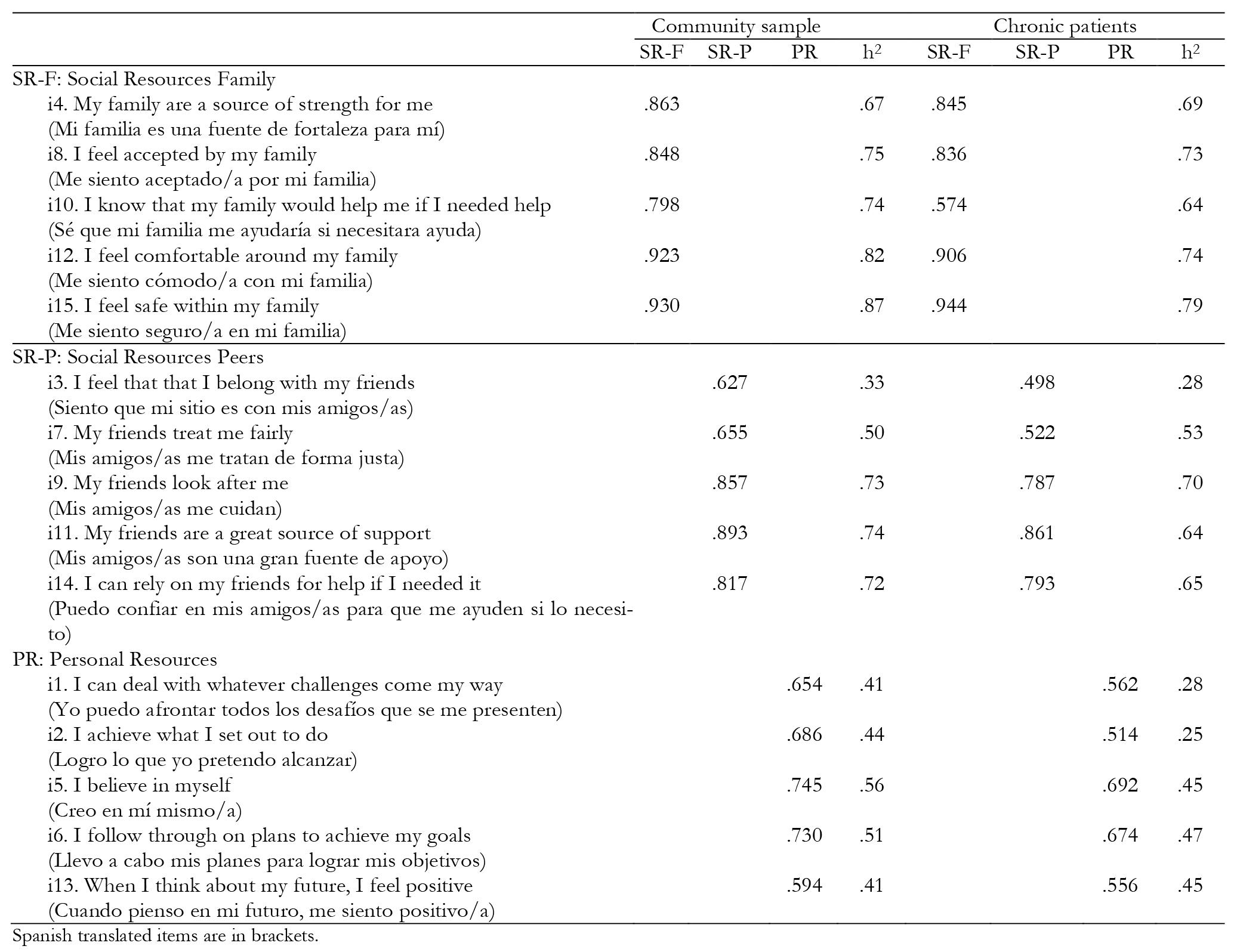
A bilingual translator translated the PFRS from English to Spanish. Two psychologists of the team independently reviewed the translation, then agreeing by consensus on a final version. Lastly, this version was back-translated from Spanish to English by another bilingual psychologist to ensure the equivalence of the translation. Table 1 contains the final Spanish adaptation of the PFSR.
A snowball sampling was used to gather data from December 2018 to February 2019, through digital internet questionnaires. Questionnaires were sent by email, Facebook, Whatsapp asking people fill them in and to send them to their relatives or friends to also be filled in. Finally, 352 healthy individuals and 90 individuals with chronic illness completed all the questionnaires. This research project was approved by the Ethics Committee of the university.
Instruments
The main sociodemographic data (age, sex, marital status, employment, educational level) were collected, and we asked participants whether they had any chronic diseases and, if so, the diagnosis. The following instruments were applied in both samples:
The Brief Resilience Scale-BRS, developed by Smith et al. (2008). This study used the Spanish validation (Rodríguez-Rey, Alonso-Tapia, & Hernansaiz-Garrido, 2016). The goal of this scale is to measure people's resilience to stress. It consists of 6 items with a five-point Likert response scale ranging from 1 (totally disagree) to 5 (totally agree). High scores indicate a high degree of resilience; the coefficient of internal consistency was .84 for the Spanish community sample and .88 in the Spanish sample of chronically ill people.
TheRosenberg Self-Esteem Scale (RSE). This instrument was originally developed by Rosenberg (1965). The Spanish version and adaptation was developed by Vázquez, García-Bóveda, and Vázquez-Morejón (2004). This scale consists of 10 items rated on a four-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). Five items are negatively worded and five are positively worded, obtaining a total score by adding all the items, and reversing the negative statements. In the Spanish community sample, the Cronbach alpha coefficient was .86, and in the Spanish sample of chronically ill, it was .82.
Ryff’s Psychological Wellbeing Scales (PWB). Ryff’s original version consists of 120 items and has an internal consistency of .84 (Ryff, 1989). For this group, the Spanish version validated by Díaz et al. (2006). was used. It consists of 39 items rated on a 6-point Likert scale ranging from 1 (totally disagree) to 6 (totally agree). The total score ranges from 122 (low psychological well-being) to 152 (high psychological well-being). The items in this questionnaire are grouped into 6 subscales that measure Self-Acceptance, Positive Relationships with others, Autonomy, Environmental Mastery, Purpose in Life, and Personal Growth. Both in the Spanish community sample and in the sample of chronically ill people, the internal consistency coefficients of the subscales ranged from .42 to .85. The overall score obtained a Cronbach alpha coefficient of .90 in both samples.
The Life Orientation Test - Revised (LOT-R); the revised version of the LOT (Scheier, Carver, & Bridges, 1994). In this study, we used the Spanish version of the LOT-R developed by Otero, Luengo, Romero, Gómez, and Castro (1998). The questionnaire consists of 10 items rated on a five-point Likert scale ranging from 1 (totally disagree) to 5 (totally agree). The dimension of dispositional optimism is evaluated with 6 items, the remaining 4 items are considered "fillers" and are intended to make the content of the test less evident. Of the 6 content items, 3 of them are worded positively (direction of optimism (O)) and 3 negatively (direction of pessimism (P)). In the community population sample, the Cronbach alpha coefficient for LOT-O was .76, and for LOT-P, it was .64. In the sample with chronically ill people, the coefficients were .80 and .69 for the Optimism and Pessimism scales, respectively.
Data analysis
The same statistical analyses were performed in both studies. The SPSS version 25.0 was used for the descriptive study of the sample, and Exploratory Factorial Analysis (EFA) was performed with Factor 10.10.01 (Lorenzo-Seva & Ferrando, 2006); the extraction method used was unweighted least squares method (ULS) with Promin rotation (Lorenzo-Seva, 1999) and Optimal Implementation of Parallel Analysis (Timmerman & Lorenzo-Seva, 2011) to decide the number of factors. The goodness of fit of the data to the model it was evaluated with the percentage of total variance explained by the factors and the following indices and reference values: Goodness-of-Fit Index (GFI) equal to or greater than .95 (Miles & Shevlin, 1998) and Root Mean Square of Residuals (RMSR) equal to or less than .08 (Hu & Bentler, 1999).
Results
Study 1
The sample consisted of 352 people aged between 16 and 83 (mean age 34.46, SD = 13.29 years), 56.5% living in the province of Alicante, and 43.5% in other provinces. Of these, 67.6% were women; 0.3% stated that they had no studies, 2.8% had primary or similar studies, 25.3% had secondary, high school or similar studies, and 71.6% had university studies. Concerning marital status, 62.2% were single, 28.1% were married or living as a couple, 9.4% were separated or divorced, and 0.3% were widowed. In terms of their work activity, 0.6% were engaged in housework, 38.6% were students, 55.7% were employed, 2.8% were unemployed, and 2.3% were retired. All participants stated that they were not diagnosed with any disease.
Construct Validity
The measures KMO = .82 and Bartlett's statistic = 2738.6 (df = 105, p < .001) indicated that the matrix is suitable for factoring. Parallel Analysis recommended the extraction of three factors. The model fit indices were GFI = .99 and RMSR = .039, values that indicate the fit of the data to the model. The 3-factor solution explained 68.84% of the total variance (factor 1 explained 41.18%, factor 2 explained 14.27% and factor 3 explained 13.39% of the variance). Table 1 shows the rotated loading matrix and communalities, all items were factor loading greater .40. Items which assess social resources family (SR-F) loaded onto factor 1, items which assess social resources peers (SR-P) loaded onto factor 2 and items which assess personal resources (PR) loaded onto factor 3. Correlations between the three factors were: SR-F and SR-P was .492, SR-F and PR was .427, and SR-P and PR was .391; these values suggest the presence of a second order.
Analysis of Internal Consistency
Table 2 shows the values of internal consistency, mean score, standard deviation, minimum and maximum PFRS score, and the subscales in this general population sample. All scores showed adequate internal consistency both in the total scale and the factor scores.

Concurrent and convergent validity
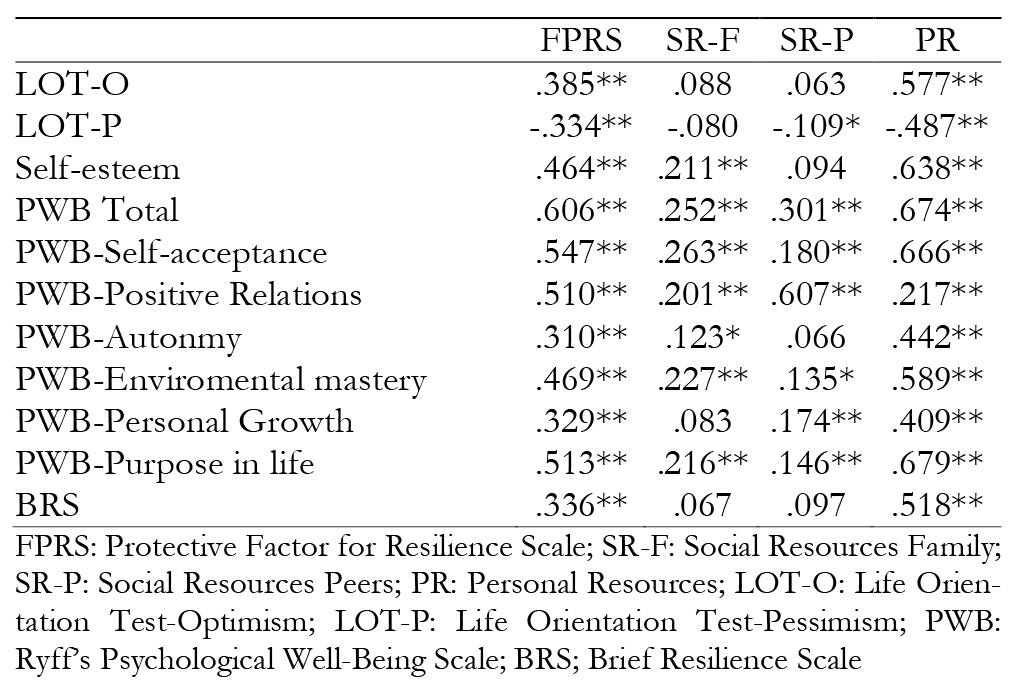
Table 3 shows the correlations between the PFRS and the other instruments applied in the sample. All correlations were positive except for those that related resilience and pessimism (assessed with LOT-P), which were negative. The highest correlations were between the total PFRS score and its PR subscale with the Optimism subscale (LOT-R), Self-Esteem, the total Ryff score and its subscales, especially the correlations with Self-Acceptance, Environmental Mastery, and Purpose in Life. The SR-P subscale had the highest correlation with the Ryff Positive Relationships subscale. The correlation between the PR subscale and the BRS was also high and significant. Therefore, this scale shows adequate evidence of convergent and concurrent validity.
Study 2
The sample consisted of 90 people with chronic diseases; their ages ranged from 17 to 77 years (mean 39.97, SD = 15.40 years); 47.8% resided in the province of Alicante, and 52.2% in other provinces. Of these, 75.6% were; 2.2% had primary or similar studies, 35.6% had secondary, high school or similar studies, and 62.2% had university studies. Regarding marital status, 48.9% were single, 44.4% were married or living as a couple, 6.7% were separated or divorced. In terms of their work activity, 4.4% were engaged in housework, 26.7% were students, 53.3% were employed, 4.4% were unemployed, and 11.1% were retired. All participants reported having a chronic diagnosed disease: 17.8% a rheumatic disease, 16.7% a circulatory system disease, 15.6% an endocrine system disease, 11.1% a digestive system disease, 11.1% a respiratory system disease, 7.8% a neurological disease, 6.7% suffered from some type of allergy, 4.4% a gynecological disease, 1.1% urological disease, 1.1% oncological disease, 1.1% hematological disease, and 5.6% did not indicate the type of disease.
Construct Validity
The measures KMO = .80 and Bartlett's statistic = 991.4 (df = 105, p < .001) indicated that the matrix is suitable for factoring. The model fit indices were GFI = 1.00 and RMSR = .033, values that indicate the fit of the data to the model. The 3-factor solution from Harms, Pooley and Cohen model (2017) was checked. Parallel Analysis recommended the extraction of one or two factors.
The 3-factor solution explained 63.82% of the total variance (factor 1 explained 42.60%, factor 2 explained 11.76% and factor 3 explained 9.45% of the variance). Table 1 shows the rotated loading matrix and communality, all items were factor loading greater .40. Items which assess social resources family (SR-F) loaded onto factor 1, items which assess social resources peers (SR-P) loaded onto factor 2 and items which assess personal resources (PR) loaded onto factor 3. Correlations between the three factors were: SR-F and SR-P was .601, SR-F and PR was .529, and SR-P and PR was .547; these values suggest the presence of a second order.
Analysis of Internal Consistency
Table 2 shows the values of internal consistency, mean score, standard deviation, and minimum and maximum score. As in the general sample, in the Spanish sample of chronically ill patients, the internal consistency coefficients of the total scale and of the three factors were good.
Concurrent and convergent validity
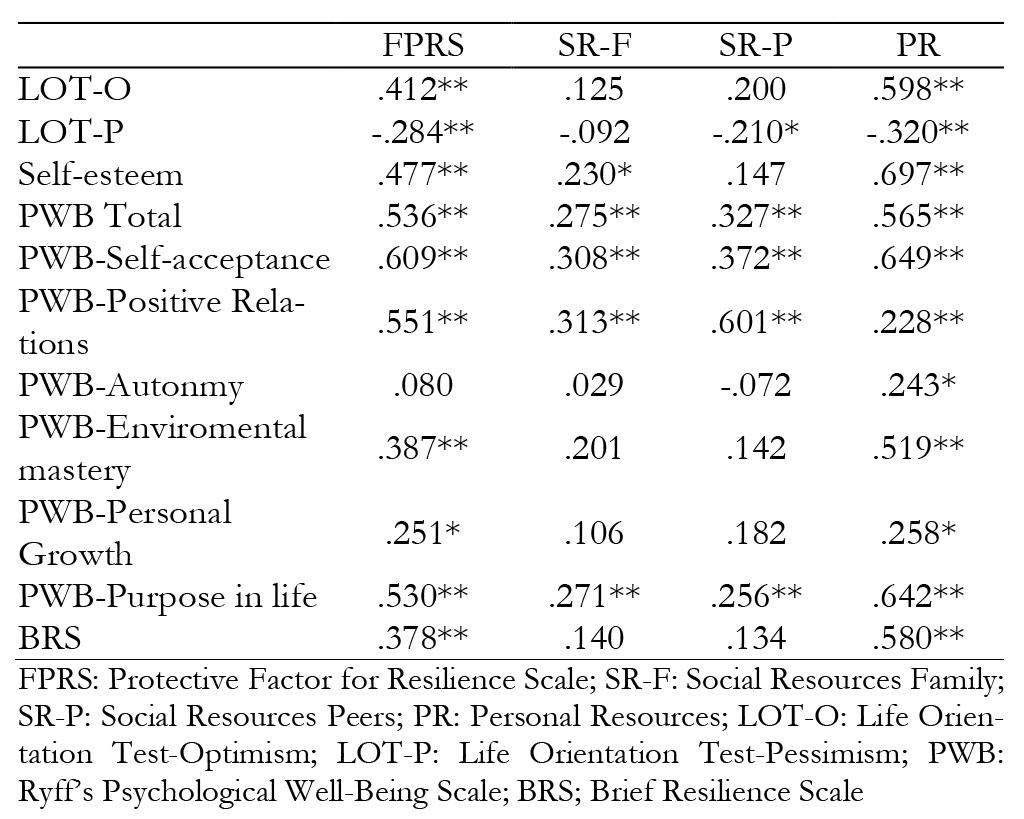
Table 4 shows the correlations between the PFRS and the other instruments applied in the sample. As in the community sample, the correlations between global score of PFRS and Pessimism (assessed with LOT-P) was negative. The positive and statistically significant correlation coefficients ranged from .228, between the PR subscale and Ryff’s Positive Relationships with others, to .697, between PR and Self-esteem.
Discussion
The objective of this study was to verify the psychometric properties of the Spanish version of the Protective Factors for Resilience Scale in Spanish community population and in a Spanish population of chronically ill patients. The results suggest that the scores of the Spanish version have adequate psychometric properties, in terms of reliability and validity.
The data of the Spanish version, analyzed through Exploratory Factorial Analysis (AFE), maintain the same factorial structure as the original questionnaire in both samples, the second-order 3-factor model. The first-order factors were: two external factors (Family and Peer Resources) and one Personal Resources factor and the second-order factor, a total resilience score. The GFI and RMSR were above and under the cut-off points, respectively, it indicated a satisfactory goodness of fit. In the sample of chronic patients, the Parallel Analysis advised to reduce the number of dimensions from three-factor to two-factor. Therefore, a second AFE was performed on this sample. So, it turned out that the SR-F factor was maintained and the SR-P and PR factors were together into one. The correlation between these two factors defined a second-order 2-factor model. The goodness of fit of data to model and psychometric properties were satisfactory as well. Therefore, further research is need to investigate whether this factor structure is a result of the sample size (although the illness samples are usually not very large) and / or if the resilience in chronic patients is explained by other components than the general population.
The analyses to assess the PFRS’s concurrent and convergent validity show that the scale factors are related to the questionnaires that measure similar constructs in both populations. We note that the factor of Personal Resources has high positive relationships with the variables Optimism (LOT), Self-Esteem (RSE), the Ryff subscales of Self-Acceptance, Autonomy, Environmental Mastery, and Personal Growth, and lastly, with the Brief Resilience Scale. This is very consistent, as all these constructs refer to the person's individual resources, thus supporting the validity of this subscale. Also, the external factor of Peer Resources has a high relationship with the Ryff subscale of Positive Relationships, again confirming the construct, as both scales refer to the relationships that are established with other people. Finally, the overall scale score is also adequately related to all the other criterion variables.
These results have different implications. First, they provide a valid and reliable measure to evaluate both internal and external resources associated with resilience for application in Spanish population. In addition, the results also indicate that this scale could be used both in general and chronically ill populations. Also, this scale is much shorter than many scales that evaluate these factors (Windle, Bennett, & Noyes, 2011) and may be much more attractive for use in different contexts, both clinical and non-clinical. However, more studies are needed, with larger samples of patients with different chronic diseases, to confirm the validity of the scale in different diseases and thus, for use in clinical settings.
This study also shows some limitations. The questionnaire was applied at a certain time without further applications, so the predictive validity of the scale could not be analyzed. The items of the PFRS are rated on a Likert format with seven alternatives. In both samples, the higher response categories (6 and 7) were the most frequently chosen in contrast to the lower ones (1 and 2) with very low frequencies, which could lead to a bias in the results. This choice homogeneity could also be affecting the reliability and validity of the scale. It would therefore be interesting to conduct another study to reduce the number of response alternatives from seven to five to determine whether the asymmetry in the choice of responses decreases. Moreover, it has been found that by increasing the number of response categories in Likert scales, reliability improves (Lozano, García-Cueto, & Muñiz, 2008), but when this number exceeds four or five alternatives, reliability does not improve substantially. Therefore, due to the response homogeneity observed in this study and the empirical evidence of the most adequate number of categories to improve the psychometric properties of a scale, a goal for further research would be to study the factorial structure of the scale by reducing the number of response alternatives to five.
In conclusion, the findings of this study support the plausibility of a second-order 3-factor model of the PFRS, and this structure is maintained in both general and chronic Spanish population. Moreover, due to the quality of the psychometric properties of the scale and its brevity, it is preferable to other measures that are currently available for the Spanish population. Nevertheless, it would be necessary to extend this work with sensitivity and specificity studies to support the use of this scale in both samples.

