










 Servicios personalizados
Servicios personalizados
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Despite the importance that society generally places on sexuality, the sexual behaviour of over the 65s has not been extensively explored in the scientific literature. One thing that has probably contributed to that is the fact that until twenty or thirty years ago, it was an age group with little demographic representation. However, from the middle of the 20th century, longer lifespans, leading to significant demographic changes, has provided an important space for older people, and their sexuality. Today, most of the world’s population lives longer than previous generations, and continue sexual activity into advanced ages (Freixas & Luque, 2009). Sexuality, not just intercourse but including expressions and behaviours such as gestures of tenderness, kissing, fondling and caressing, does change but is maintained throughout life (Sáez, 2010) and is an integral part of an individual’s development (Cayo, Flores, Perea, Pizarro & Aracena, 2003).
Apart from its reproductive side, sexuality as a relational, hedonistic, ego-integrative aspect of humanity makes up a plan of personal growth that doubtlessly will contribute to older people’s quality of life (Cayo et al., 2003). On these lines we can refer to large studies performed in the United States of America (Lindau et al., 2007) and the United Kingdom (Mercer et al., 2013; Mitchell et al., 2013) which note that older people engage in intimate relationships and believe sexuality to be an important component of their lives, leading to the conclusion, also in Spanish samples, that sexual activity can be a predictor of general health and quality of life in these older people (Palacios et al., 2012). It is worth placing the importance of this current research in this context, the aim of which is to understand the factors that can potentially explain sexual inactivity in older populations.
The little tradition of research on the topic of sexuality in old age has focused on sexual dysfunction in both men and women, and on the link between health and sexual activity. Since the beginning of the 21st century, and as the availability and efficacy of drugs to treat male erectile dysfunction have increased, men’s active sex lives and that of their partners have been extended (Lindau & Gavrilova, 2010). In light of the development of the literature about sexual dysfunction, research has addressed the link between health, individual wellbeing and sexual activity in older populations. The results of various studies have contributed to the claim that, in effect, sex, especially linked to a sexual partner, is related to health (Palacios et al.,2012). An individual’s health problems, or problems in either one of a couple, are reported as the greatest obstacle to sexual activity in the population aged between 50 and 92 (Gott & Hinchliff, 2003).
Assuming an increase with age in the umbers of sexually active men and women reporting sexual health problems (Lee, Nazroo, O’Connor, Blake & Pendleton, 2016), research seems to suggest that suffering from various chronic ailments common in the older population (e.g. arthritis, CVA and diabetes) and the perception of poor general health are associated with reduced sexual functioning and activity, especially in men. Sexual activity is related to the perception of physical and sexual health in those over 65 such that both men and women who believe themselves to be in poor health are less likely to be sexually active (Palacios et al., 2012; Schick et al., 2010). Low levels of sexual activity and problems of sexual functioning, especially in men, have been associated with poor perceived health (Steptoe, Breeze, Banks & Nazroo, 2013). While men in good self-perceived health are predominantly sexually active with their partner, those in perceived poor health report higher frequencies of masturbation (Schick et al., 2010). In women there is also an association between reduced frequency of oral sex and intercourse and the perception of poor health (Schick et al., 2010). This can be interpreted as the link between sexual inactivity and the perception of health which we hypothesise in this study (Ekström et al., 2018; Ginsberg, Pomerantz & Kramer-Feeley, 2005).
Despite sexuality being an important part of most people’s lives, stereotypes about older people generally disregard the value of sexual activity for quality of life and emotional wellbeing (Lee et al., 2016). The attitudes older people have towards sexuality may be one of the variables which affect their sexual activity. Various studies have indicated a very stigmatised view of sexuality on the part of older people, in women (García, 2000, 2005; Leyva-Moral, 2008; Rodríguez-Llorente, Piñeiro, Rodríguez, Regueiro, Estévez & Freire, 2018) and in men (Syme & Cohn, 2016).
Modern society maintains many stereotypes about sexual behaviour in old age, and these are also reflected in the attitudes of older people, affecting their sexual practices. Leyva-Moral (2008) stated that the sexual behaviour of many older women could be affected if they were convinced of the truth of certain ideas such as older women who were interested in sex were those who were addicted to it in youth, or that sex before marriage or sex outside of a stable relationship were bad. Even when it comes to evaluating the capacity to enjoy sex, many studies have reported a stereotypical belief in women that men have naturally higher sexual drive than women (e.g. Rodríguez-Llorente et al., 2018). Research has shown that sexual activity is still important to older people, and despite society having ever more permissive attitudes, there continues to be a stigma about sexual activity in old age. It is important, therefore, to thoroughly examine these types of variables related to beliefs and attitudes, and how they affect sexual activity as people age.
Finally, in this study we also explore a series of sociodemographic variables such as age, civil/partnership status, educational qualifications and place of origin in order to identify the extent to which these conditions predict sexual inactivity in the previous year in a sample of older people. Previous research leads us to hypothesise, for example, that the lack of a partner could be a key factor in explaining sexual activity (Ekström et al., 2018; Ginsberg et al., 2005; Huang et al., 2009; Palacios et al., 2012; Smith, Mulhall, Deveci, Monaghan & Reid, 2007) or that age may be one of the variables with most explanatory weight for this inactivity (Ginsberg et al., 2005; Palacios et al., 2012).
Given that sexual behaviour is learned from the specific sociocultural surroundings (Gagnon, 1990), it would not be unusual for certain cultural differences to be explanatory factors for this activity in older people. These cultural differences in the sexual sphere may mould older people’s sexual expression and behaviour (Sandfort, Hubert, Bajos & Bos, 1998). We have comparative studies which demonstrate differences between countries and regions in terms of permissiveness related to sexual behaviour (Baumeister & Mendoza, 2011; Haavio-Mannila & Kontula, 2003) which lead us to hypothesise the impact of the sociocultural environment on sexuality (Fischer, Traen, & Martin, 2018). Because of that, the place of origin may be an explanatory variable for older people’s sexual attitudes and behaviour.
The level of education has also been shown to be one of the variables to explore when explaining sexual activity in older people, with the understanding that sexual activity may be positively correlated with older individuals’ educational levels (Palacios et al., 2012; Wang, Lu, Chen & Yu, 2008).
Our overall objective with this study is to understand the factors that may potentially explain sexual inactivity in a sample of older people. We are particularly interested in discovering:
- Whether various sociodemographic factors (place of origin and geographic region, educational and economic level, civil status/partner status, and age) are associated with sexual inactivity in the previous year.
- Whether self-perceived health is an explanatory factor in sexual inactivity in the previous year.
- Whether attitudes towards sexuality are also an explanatory factor for a lack of sexual activity in the previous year.
Method
Design
This study followed a quantitative empirical-analytical approach, with a correlational-descriptive design via survey. It is transversal, as the data were collected at a single point in time.
Participants
The sample was non-probabilistic by convenience. It was made up of 200 older people (men and women) resident in the city of Santa Rosa (El Oro, Ecuador) who were members of the Association of Pensioners and Retirees of the city of Santa Rosa. Inclusion criteria were set at being over 64 years old and having the evident capacity to respond to the questions coherently. Most of the men and women in the sample (79.5%) were from the coastal region (la costa) and the remainder (20.5%) were from the highlands (la sierra) of Ecuador. Sociodemographic studies have characterised people from the coastal region as more open and uninhibited than those from the highlands, who are more reserved and conservative in many areas such as sexuality.
The mean age of the women in the sample was 71.8 (SD = 5.52), with ages ranging from 65 to 91. The mean age of the men in the sample was 70.7 (SD = 5.42), ranging from 64 to 90. As Table 1 shows, there were no significant differences in the proportions of men and women in the age ranges in terms of economic level, origin, zone or sector.
Significant differences were found between men and women in terms of civil status, current partnership status and educational level (χ2 = 43.495, p < .000; d = 1.02; χ2 = 29.804, p < .000, d =.78 and χ2 = 16.157, p = .003, d = 0.56, respectively). While 63% of men were married, only 29% of women were, and 39% of the women were widowed compared to 9% of men. These differences are consistent with the 67.7% of the men reporting having a sexual partner, while 71% of the women reported the opposite (see Table 1).
Table 1. Frequencies and proportions in the interaction between sociodemographic variables and gender.

Significant differences were also noted in the educational levels of the men and women in the sample. Almost half (45%) of the men reported finishing secondary education or university, only 23.2% of the women reported the same.
There were also significant differences between men and women regarding previous partners (χ2 = 43.495, p = .001; d = 0.51). Almost three-quarters (70%) of the men had partners in the past, but less than 50% of the women reported having previous partners.
Instruments
The instrument chosen for this study was a translation of the SRA-Q (Lee et al., 2016) which was carried out by the Educational Psychology Research Group (GIPED) at the University of A Coruña (Spain). This translation modified the original items, designed for British populations, for Spanish-speakers. The original instrument was created using other validated instruments (Mitchell, Ploubidis, Datta & Wellings, 2012; O’Connor et al., 2008; Waite, Laumann, Das & Schumm, 2009) and ensures gender specificity by offering one questionnaire for men and another for women. In total the men’s scale has 50 items, the women’s scale has 44. The men’s scale asks about ability to achieve and maintain erections, the women’s scale asks about ability to be sexually aroused. Both versions include items about orgasm and the respondent’s overall sex life in recent months as well as their sexual experiences during their lives. Given our study objectives, we only used questions related to sexual activity and attitudes towards sex.
To determine sexual inactivity in the sample we used the item “In the last twelve months, have you engaged in sexual activity (intercourse, masturbation, fondling or petting)? from the SRA-Q, with a dichotomous yes/no response that we coded as sexual activity YES = 0 and sexual activity NO = 1.
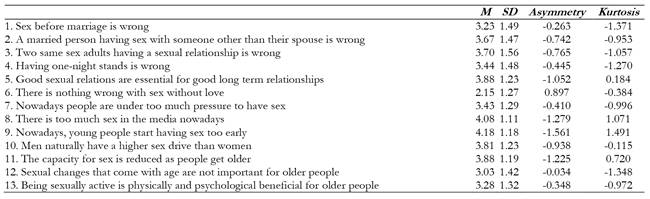
We used 13 items (α=.62) from the SRA-Q (Lee et al., 2016) to examine attitudes towards sexuality. These were presented as a series of statements such as: “It is wrong to have sexual relations before marriage”; “Men naturally have a higher sex drive than women”; “Two adults of the same sex having sexual relationships is wrong”; and “There is too much sex in the media nowadays”, with responses on a five-point Likert-type scale from 1 = completely disagree to 5 = completely agree.
For the evaluation of perception of health, which is also of interest in this study, we used two questions: (a) My general health is currently… and (b) My sexual health is currently…; in both cases we used a Likert scale with five response options from 1 = excellent to 5 = very poor (α=. 60). Concern about sexual health was evaluated with the SRA-Q item: Even if you have not had any sexual activity in the last three months, how concerned are you about your sex life overall? with a five-point Likert scale response from 1 = not concerned at all to 5 = extremely worried.
Finally, in order to examine various sociodemographic aspects of the sample, we included a series of questions about place of origin, zone or sector, civil status or current partner status, educational level and economic level.
Procedure
Firstly, the management of the Retiree’s Association of Santa Rosa (El Oro, Ecuador) signed their informed consent. Then the participants were informed of the aims of the study, confidentiality and the ethical management of the data. Once it was confirmed that they met the inclusion criteria, the self-report form was presented and the instructions for completing it were read aloud.
The questionnaire was completed individually, anonymously and voluntarily. The researchers were present during the administration of the test instruments to answer any questions and ensure that the subjects completed their questionnaires independently. No subjects participated without their express agreement once they were aware of the objective of the research.
Data Analysis
First, we examined the properties of the items used to measure attitudes towards sexuality and perception of health. The predictor equations for sexual inactivity in the previous year were established via logistical regression, following the forward stepwise regression process based on the Wald statistic. Three logistical regressions were performed taking sociodemographic variables, perceived health and attitudes towards sexuality as predictors and including in each case as the criterion, the dichotomous sexual activity variable (sexual activity YES = 0, sexual activity NO = 1) in response to the item: In the previous twelve months, have you engaged in any sexual activity (intercourse, masturbation, petting or fondling)?
Two indicators were used to assess model fit: (a) Nagelkerke’s R2 , which indicates the percentage of variance explained by the models (Nagelkerke, 1991), and (b) the percentage of correctly classified cases, which lets us determine how useful the predictor variable is in estimating the criterion in each proposed model.
All of the statistical analyses were performed using SPSS (Version 20).
Results
Once we had determined that 60.5% of the sample had not had any sexual activity in the previous year, the next step was to explore the impact of sociodemographic factors, perceived health, and attitudes towards sexuality on this sexual inactivity.
Impact of place of origin, zone, economic level, educational level, civil status / partner status and age on sexual inactivity
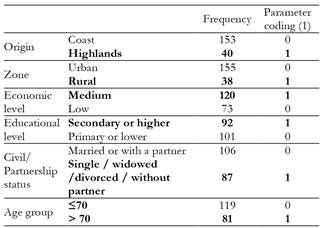
For the sociodemographic variables, a logistical regression model was produced to make estimations about sexual inactivity in the previous year (sexual activity = 0 / sexual inactivity = 1). The dichotomous categorical predictor variables for the regression equations are codified as in Table 2.
Table 2. Frequencies and coding of parameter (1) for the sociodemographic variables included in the regression equation.
The final sociodemographic model correctly classified 71% of the sample (χ2 = 47.150, p = .000) with a high level of sensitivity when estimating sexual inactivity in the previous year (81.5%) (see Table 3).

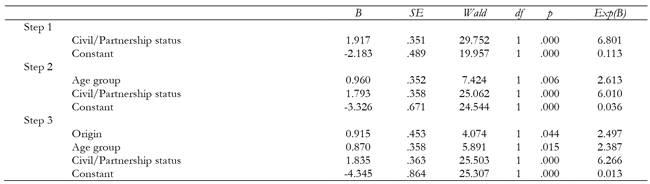
Analysis of the final step suggests the inclusion of only three variables: civil status, age and place of origin, giving us to understand that the other sociodemographic variables added at the beginning (zone, economic level, educational level) do not seem to provide predictive information about sexual inactivity.
The forward stepwise regression procedure based on the Wald statistic shows that not having a partner is the variable that most explains sexual inactivity during the previous year (W = 25.503; p < .01), although age and place of origin also appear in the model (W = 5.891; p = .015 and W = 4.074; p = .044, respectively) (See Table 4). With a percentage of explained variance around 30% (Nagelkerke’s R2 = .295), looking at the codification of the parameters, we can say that not having a partner -being single, widowed, or divorced-, being over 70, and coming from the highlands would increase the likelihood of sexual inactivity in the sample in the previous year.
Impact of perceived health on sexual inactivity
Having confirmed that the distribution of the items was normal (see Table 5), considering the perception of overall health, current sexual health and concern about sexual health, a logistical regression model was produced to estimate sexual inactivity during the previous year (sexual activity = 0 / sexual inactivity = 1). With a good success rate (73.5%), the model of perceived health would correctly classify 64.2% of the sample (χ2 = 26.163, p < .000) (see Table 6).


We see that the combination of current poor perceived health (W = 16.635; p < .01), together with low concern about sexual health (W = 5.056; p = .025), can explain to a certain extent (Nagelkerke’s R2 = .178) sexual inactivity in the sample in the previous year (see Table 7).

Influence of attitudes towards sexuality on sexual inactivity
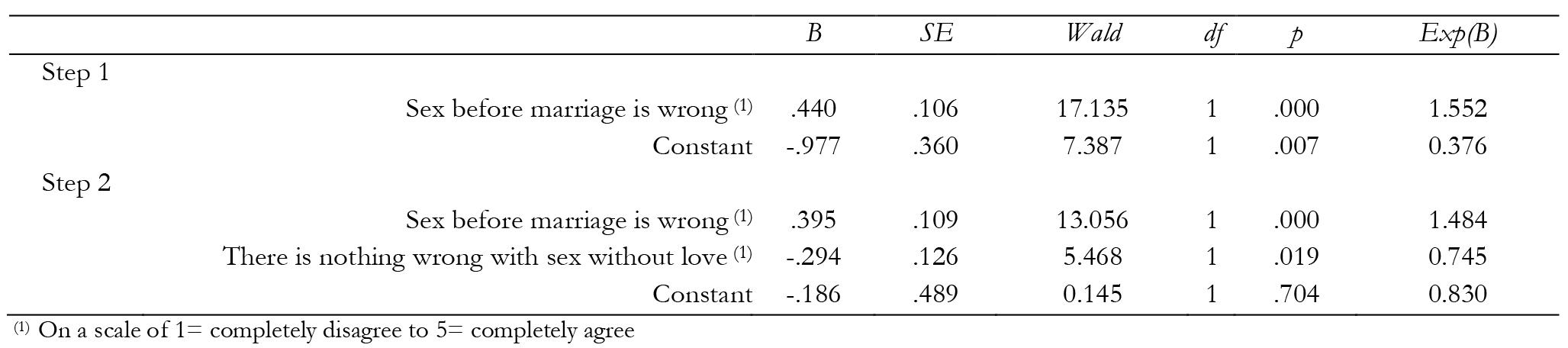
Once the properties of the items had been examined (see Table 8), in order to explore whether attitudes towards sexuality were linked to inactivity a stepwise regression model was produced looking at the measures used in this study. We can confirm that beliefs about sex before marriage and sex without love can affect current sexual inactivity to some extent (Nagelkerke’s R2 = .161).
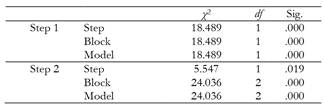
This model of attitudes towards sexuality would correctly classify 68.3% of the sample (χ2 = 24.036, p < .000) with a high level of sensitivity (83.2%) when estimating sexual inactivity in the previous year (see Table 9).
Similarly, considering sex before marriage wrong (W = 13.056; p < .000), or sex without love wrong (W = 5.468; p = .019) can also limit a subject’s sexual activity (see Table 10). No significant relationships were found between other beliefs about sexuality and sexual inactivity.
Discussion
The aim of this study was to understand the extent to which various sociodemographic variables, self-perceived health, and the attitude towards sexuality affect sexual inactivity in older people. The levels of inactivity in our sample were similar to those found in other research (Palacios et al., 2012; Smith et al., 2007). Our results confirm the lack of a partner, age, and place of origin to be the variables that best predict sexual inactivity in older people. It is also worth highlighting that sexual activity may also be affected by the perception of and concern about sexual health, as well as by beliefs about premarital sex, and sex outside loving relationships.
Having a partner, age and origin had significant explanatory power in sexual inactivity in the previous year (R 2 = .295). The percentages of variance of sexual inactivity explained by the model of perceived heath (R 2 = .178) and the model of attitude towards sexuality (R 2 = .161) were similar and both lower than the variance explained by sociodemographic conditions.
The predictive capacity of the lack of a partner on sexual inactivity confirms the findings of a large number of previous studies (Ginsberg et al., 2005; Huang et al., 2009; Ekström et al., 2018). In Smith et al. (2007), for example, the reported reasons for sexual inactivity in older women included a lack of desire and/or not having a partner, and in older men they included erectile dysfunction and not having a partner. In a sample of older Spanish people, Palacios et al. (2012) also reported that not having a partner was a predictor of sexual inactivity in both men and women. A study by Huang et al. (2009) concluded that, in effect, not having a sexual partner contributed more to sexual inactivity than, for example, health problems.
Although not having a partner is the sociodemographic variable that explains sexual inactivity in the previous year best, our results show that age and origin also enter into the explanatory equation for sexual inactivity. This is also in line with other research. Age was one of the reasons with most explanatory weight in sexual inactivity in studies by Ginsberg et al. (2005) and Palacios et al. (2012). In terms of origin, our results show that coming from the highland region of Ecuador rather than the coastal region can be associated with greater sexual inactivity in the previous year. It is likely that the reserved, conservative nature usually evident in those from the highlands, with a more negative view of sex, would have an impact on sexual activity.
Culture is no doubt an important framework for the understanding of sexuality (Agocha, Asencio & Decena, 2014) and while there are various studies that have looked at differences in permissiveness and acceptance of sexuality between countries and regions (e.g., Baumeister & Mendoza, 2011; Haavio-Mannila & Kontula, 2003), they are susceptible to change in currently highly globalised societies. In this respect, despite expecting to find substantial differences between older people form the North, centre, and South of Europe, a recent study by Fischer et al. (2018) did not find origin to be a predictor variable of sexual activity in male-female couples aged between 60 and 75 in Norway, Denmark, Belgium and Portugal.
Our study also looked at the relationship between perception and concern about sexual health and sexual inactivity in the previous twelve months, as other studies have done before (e.g., Dominguez & Barbagallo, 2016; Lee et al., 2016; Lindau et al., 2007; Lindau & Gavrilova, 2010). Our results show that perceived poor sexual health, together with low concern about it, enter into the equation explaining sexual inactivity in the previous year, albeit with criterion sensitivity slightly lower than the models related to attitude or sociodemographics.
Our findings are in line with previous research indicating that those who reported not having engaged in sexual activities in the previous year reported worse sexual health and worse overall health, while more sexually active men and women reported better health (Lindau & Gavrilova, 2010; Ginsberg et al., 2005; Ekström et al., 2018; Palacios et al., 2012). In addition, research by Rodríguez-Llorente et al. (2018) with a Spanish sample aged between 65 and 90 found that the perception of health in those who had engaged in any kind of sexual activity in the previous year was significantly better than those who had not.
Finally, when it comes to attitudes towards sexuality, we should bear in mind that the stereotypes of an asexual old age are still present in older people’s perspectives. Research has found that older people interiorise sexual stereotypes related to their age which become significant obstacles to them being able to freely express and enjoy their sexuality (Gewirtz-Meydan et al., 2018; Snyder & Zweig, 2010). Despite starting to be included in research agendas, and despite stigmatised views of sexuality being explanatory factors in sexual inactivity, the attitudes of older people about the role and value of sex in their lives continues to be a little-explored topic.
Looking at our results, negative views about sex before marriage and sex outside loving relationships can be specifically associated with sexual inactivity to the same extent as having a partner and age. In fact, the sensitivity of the attitude model (negative beliefs about sex before marriage and sex without love) estimating the probability of sexual inactivity is similar to that of the sociodemographic model (not having a partner -being single, widowed, or divorced, being over 70, and coming from the mountains). Thus we see the potential of our results as a basis for health interventions as well as socioeducational initiatives, as people’s beliefs and attitudes about their sexuality may be a more parsimonious predictor of sexual inactivity than the traditional sociodemographic factors.
Older people who recognise sexual activity as an important indicator of their wellbeing and quality of life, and those with positive attitudes towards sexuality in old age, are more likely to continue being sexually active with the passage of time (Fischer et al., 2018; Kontula & Haavio-Mannila 2009). However, beliefs that associate sexuality with loving partnerships and matrimony would tend to explain sexual inactivity in older populations and could also underlie recurrent differences research has found in sexual activity between older men and women.
In the light of these results, we believe that the challenge for health professionals in this area is to recognise the importance of sexuality in old age through fluent, effective communication with older people about their concerns and worries about their sexual lives (Bauer, Haesler & Fetherstonhaugh, 2016). Our results may assist the recognition of the importance of working to break down social barriers in front of certain age groups about what old age should be like which prevent them from freely expressing their sexuality.
Although the results of this study seem to be robust, they should be taken with a certain amount of caution due to some limitations in the nature of the study data, the sample used and the measuring instrument. This was a transversal study, which severely restricts any causal inferences. It would be interesting to begin longitudinal follow-up studies which would allow us to observe the explanatory potential of attitudes to sexuality, perceived health, and various sociodemographic variables such as origin, civil/partnership status, and age, and to see the extent to which we can suppose progressive changes in individuals’ sex lives.
We would admit that the results might have been significantly different if our sample had been obtained randomly and had been more fully representative of the population it came from. Sampling by convenience and small sample sizes are only justified by the difficulty of getting self-reported information about a clearly sensitive topic.
Finally, data collection was done by self-report. Although this is a commonly-used methodology in psychology, and possibly essential for measuring beliefs and behaviours that are difficult to observe in other ways, our findings need to be replicated using complementary strategies and resources of other types. In addition, the variables in this study were evaluated through a relatively small set of items, which might compromise the robustness of these measures. These types of measures created from self-reported information can be highly subjective in older populations, as one must assume that their perceptions and reality may not completely coincide.

