










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkThe European Journal of Psychiatry
versión impresa ISSN 0213-6163
Eur. J. Psychiat. vol.23 no.4 Zaragoza oct./dic. 2009
Community study on a parasuicidal population: Clinical identification of repetition risk
Francisco Rodríguez Pulido*; Manuel E. Méndez Abad**; Enrique González Dávila***; Marica Grasso****; Ángeles Rodríguez García*****
* Facultad de Medicina. Universidad de La Laguna. Tenerife
** CP La Perdoma. La Orotava. Servicio Canario de la Salud. Tenerife
*** Universidad de La Laguna. Tenerife
**** Médico colaboradora del Área de Psiquiatría
***** Hospital Universitario Nuestra Señora de La Candelaria. Servicio Canario de la Salud. SPAIN
ABSTRACT
Background and Objectives: The greatest predictor of eventual suicide is parasuicide. The aim of this research was to identify the clinical features that can identify people with high parasuicide purpose among a parasuicidal population.
Methods: A total of 48 persons who had commited a parasuicide episode 2-6 years after, were interviewed and classified according Research Diagnostic Criteria. During the interviews, socio-demographic data and psychopathological features were picked up through several scales. Scores on Beck Depression Inventory (BDI), Beck Anxiety Inventory (BAI), Beck Hopelessness Scale (BHS) and The Plutchick Impulsivity Scale (PI) were measured. These persons were then followed-up for two years.
Results: At follow-up, eight persons (16,7%) had repeated at least one parasuicide act. On comparison of repeaters and no repeaters, a higher significant differences in the final values reported in BHS was found but not significative differences were founded in the BAI, BHS or PI scores or in the proportion of the different mental illness (according RDC). An interesting finding is that in the repeaters group the average value in the IP scale tended to be lower than in the non-repeaters, although not significant.
A high percentage (72.8%) related the existence of negative vital events with their suicide attempt, more often, relationship problems with the spouse (42.8%), with their parents (17.1%) or the breakdown of an interpersonal relationship (14.2%).
Conclusions: In persons who have a past history of previous parasuicides, a high value in BHS is associated with the risk of repetition in the subsequent two years.
Key words: Parasuicide; Suicide; Impulsivity; Hopelessness; Community study.
Introduction
Suicide is a serious public health problem that ranks among the top ten causes of death for individuals in many countries. In spite of this data, suicide is still not appropriately registered by the official statistics1-4 and that is also the case for parasuicide5, 6. It is admitted that these behaviors are as the result of complex interactions of genetic, psychological, cultural and environmental factors7. The studies, therefore, require the identification of risk and protection factors to be able to present a high prediction value to prevent the behaviors with significant reduction in the numbers of morbidity and mortality.
In the practice, some investigators have suggested that the most appropriate way of studying the genetic role in complex behavioral syndromes such as suicide, is by focusing on intermediate phenotype like impulsivity8, 9. During these last years, several studies have proven that hopelessness10-12 and a past history of parasuicide13-16 represent other important factors of interest for the study of suicidal behavior. These three factors are outstanding in the historical study of suicidal behavior. The negative vital events maintained in the time, of chronic nature, also act as precipitant of this behavior17.
The study of the impulsivity is very important too. Several works put in evidence that many suicide attempts are impulsive and not planned18-27. Also, research has observed that the suicide attempters with high impulsive traits differ to those with low impulsive traits in relation to more aggressive behaviors28. Furthermore, these attempters, have shown an higher incidence of alcohol and drug abuse or dependence29.
Several theories and works have shown that parasuicide and aggressiveness both have similarities and usually are manifested at the same time30-33. Also, early adverse events in life, play an important role in the development of an abnormal expression of the impulsiveness in childhood that would lead then to the manifestation of aggressive behaviors and suicidal behaviors in adulthood34, 35.
Another very important factor in the study of suicide is the presence of past history of parasuicide. Suicide attempters, in fact, present higher frequency of new episodes of parasuicide (up to 20-30% in the 3-8 subsequent years) and death as a result of suicide (up to 10-14%), with a risk 100 times more elevated that the general population and 22-36 times more elevated that the population with depression. For this reason, at the moment, parasuicide is considered the parameter that better predicts suicide.
The aim of this community study is to identify the clinical features that can decipher people with high parasuicide purpose among a parasuicidal population.
Material and method
Design: Descriptive longitudinal study with two years follow-up.
Parasuicide definition: Non-fatal act in wich an individual deliberately causes self injury or takes a substance in excess of any prescribed or generally recognised therapeutic dosage. The apparent purpose or motivation undelying the act is not taken in account. Individuals intoxicated with alcohol alone are excluded.
Inclusion criteria: Persons ranged in age 18-64 years, of an defined geographical area (north of Tenerife island), who had a history of previous parasuicide (one or several) between 1992 and 1996. The study population was derived from the Epidemiology of parasuicide in Canary Islands5.
Exclusion criteria: Persons with lack of a phone contact, alcoholism, serious drugs addiction, mental retardation, acute or chronic psychosis, serious personality dysfunction or serious organic pathology were excluded.
Subjects: 48 subjects, 8 male and 40 female. 265 cases suited the inclusion approaches but there was only possible to contact 203 people telephonically while 128 declined to be interviewed and the reasons were as follows: no illness (n = 9), unwillingness to review that particular period in their life or not time (n = 92), illness (n = 7) and the remaining 30, accepted but they did not turn up at the appointments. Twenty seven were excluded after the initial interview because of exclusion criteria as follows: psychoses (n = 13), substance or alcohol abuse (n = 4), borderline personality (n = 3), organic disease (n = 5), didn't a parasuicide (n = 1), declined (n = 1) and the other one had died for cancer. The remaining 48 (18,11%) accepted and were included.
Follow up period: The persons were included in the study and interviewed in the Mental Health Units in 1999 and were then followed for two years (untill 2001) and it was observed how many subjects had attempted parasuicide another time.
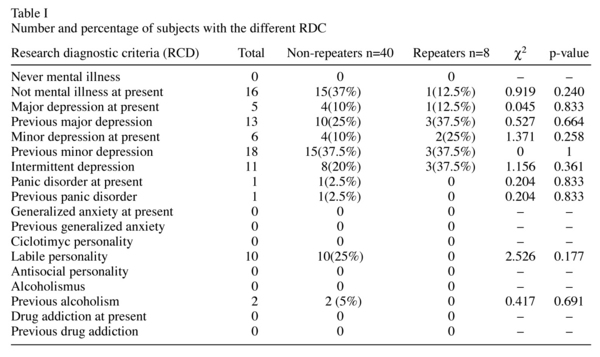
Procedure: All the participants were interviewed in a Community Mental Health Unit in 1999 after having read and signed the informed consent. The participant's socio-demographic data was documented and each person was interviewed to verify if they completed the Research Diagnostic Criteria (RDC) reported in table I. A table of vital events was executed at home and they returned it by prepaid mail. The followed scales were applied:
- The Beck Anxiety Inventory (BAI) provides a quick measure of the levels of the patient's anxiety (36). The final value obtained with the 21 items describing the somatic, subjective and panic-related symptoms referred by the patient.
- The Beck Depression Inventory (BDI) is constituted by a series of questions developed to measure the intensity, the severity and the graveness of the depression in patients with psychiatric diagnosis37. The longer version is composed by 21 questions, each one directed to the value of common specific symptoms in people with depression.
- The Beck Hopelessness Scale (BHS) was designed to study the negative attitude about the future expectations38. It is constituted by 20 items that measure the 3 main aspects of the hopelessness: feelings about the future, loss of motivation and expectations.
- The Plutchick Impulsivity Scale (PI) was used to study the features of impulsive personality39-43. This scale consist of 15 items, with a final value from 0 to 3, being able to reach a final value included between 0 and 45.
- The Scale for Suicidal Ideation (SSI) was designated to measure intensity, pervasiveness and characteristics of the suicidal ideation44. The 21-item scale includes 5 screening items that reduce the length and intrusiveness of the instrument for non-suicidal individuals.
- Müncher Alkoholismus Test (MALT) was used in order to assess the severity of the alcoholism45. The test is constituted by 31 questions, 7 answered by the interviewer and 24 by the subject.
Data analysis: Was carried out by a descriptive analysis of all the subjects and comparative analysis inter-groups (non-repeaters vs repeaters) and intra-groups (multiple previous acts or one previous act). The results are shown in tables with the size sample, the percentages, the average and with their corresponding standard deviation and 95% confidence interval. Student's t-test was used for the comparison of continuous variables and the c2 test (tables 2x2 with correction for continuity of Yates and exact statistic of Fisher) for the comparison of categorical variables. Data were analyzed using SPSS/version 15 and Statistica/version 5 software packages.
Results
At the end of the study, in 2001, eight persons had committed 12 new parasuicides acts. For the data analysis, we divided the persons into these groups:
a) Patients not committing parasuicides during the follow-up period (n = 40; non-repeaters group).
b) Patients committing parasuicide in the follow-up period (n = 8; repeaters group). Of the 48 persons included in the follow-up study in 1999.
c) Fifty per cent (n = 24) had attempted parasuicide at least twice at the time of the interview (multiple previous acts group).
d) Fifty per cent had attempted parasuicide once only (one previous act group).
Table I shows the psychiatric diagnosis of the patients (RDC) in both groups (non-repeaters and repeaters) and no significative differencies were found, but the diagnosis of absence of current mental illness was 37.5% in the repeaters group vs 12.5% in non-repeaters group.
Table II shows socio-demographics characteristics in the six months that preceded the interview. When comparing them appear as factors of risk for parasuicide the female sex (83.3%; c2 = 21.33; p < 0.001) and the medium-low education class level (89.5%; c2 = 30.08; p < 0.001).
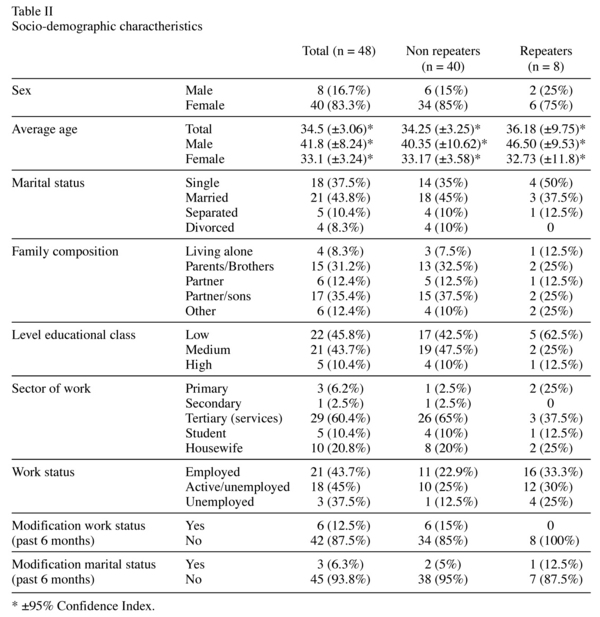
Women have the tendency to attempt parasuicide younger than men (33,1 years vs 41,8 years; t = 2.242; p = 0.030). To be single (OR = 1.859) and the low education class level (OR = 2.257) tended more often to be associated with repeated attempts in the future, although they aren't significant.
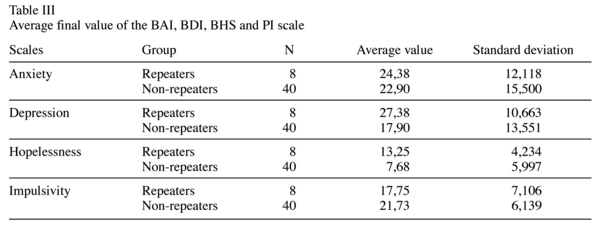
No significative differences in the Anxiety, Depression or Impulsivity psychometrics scales values between the non repeaters and repeaters parasuicides subgroups were found (table III). On the other hand the differences in the final values reported in the scale of Hopelessness are significant (t = 2.497, p = 0.016).
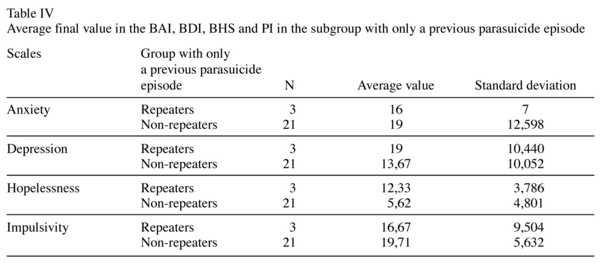
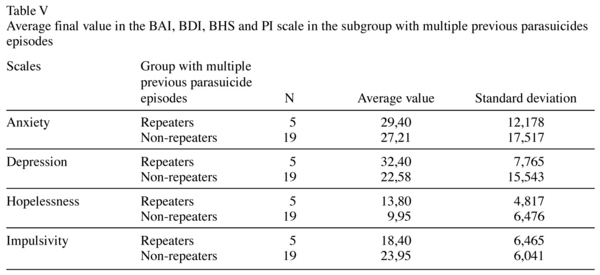
In the subgroup with only one previous act, (table IV) the average value in Hopelessness scale was higher in repeaters than in non repeaters (12,33 vs 5,62; t = 2.306; p = 0.031). No other significant differences were found between these subgroups. As is shown in table V, in the subgroup of multiple previous parasuicides not significant differences were found between non repeaters and repeaters groups.
A high parasuiciders percentage (72.8%) related the existence of one or more negative vital events with their suicide attempt. The more frequents vital events related were: the relationship problems with the spouse (42.8%), with their parents (17.1%), the breakdown of an interpersonal relationship (14.2%) and the problems in the work place (11.4%).
Discussion
Not only in sheer numbers, but also in terms of human suffering, the phenomenon of parasuicide is a public health problem of primordial importance, particularly among adolescents and young adults. The suicidal thought shows a complex relationship among internal genetic-psychopathological factors and external environmental-cultural factors7, and for this reason, it is fundamental to study a sample that should be the most typical representative of the general population, not of specialized hospital services, and that should not be influenced by other variables.
The present study examined the relatioships of clinical variables (as hopelessnes, depression, anxiety or impulsivity) with pa-rasuicide repetition. We explored this problem by dividing the clinical sample into persons who, in the two years follow up, repeated a parasuicide act and those who don't repeat it. A characteristic of this study, is that was carried out with recruitment of subjects in the community environment and also, several years after the parasuicide. A well-known difficulty, is the recruitment of people for clinical studies but these characteristics represent an added methodological difficulty. Indeed, most of the studies on parasuicide are carried out in the hospital environment, where everyone can obtain a wider sample. In this case, the sample, although smaller, it has the advantage of being representative of the general population more so than the samples of other works which recruit amongst hospitalized patients. In spite of these difficulties and limitations, this study is in agreement with the findings of Welch46, where the female sex and medium-low educational class level represent risk factors for parasuicide and also that women have the tendency to attempt parasuicide younger than men. Studying the evolution of parasuicidal behavior in the time following the parasuicide it is observed that the average age of the women decreases and that of the men increases, while single marriage status and low educational class level seem to be the main characteristics of the subject that repeat a parasuicide act.
As is shown in table I, all the subjects have had a diagnosis of mental illness in their personal history. In particular, several studies verify that parasuicide is associated with depression, anxiety and dysfunctions of personality47-49. Our findings replicate those data: up to 42 parasuiciders (87.5%) completed the diagnostic criteria for previous or intermittent depression and, also, a high percentage of subjects completed the diagnostic criteria for current depression (45.8%). We didn't observe drug addictions and diagnoses of alcoholism, which are typically associated with parasuicide because they were part of the exclusion approaches.
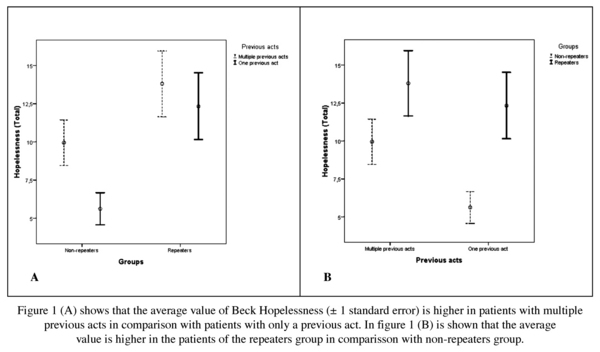
Between non-repeaters and repeaters groups, the final values of the psychometrical scales don't show significant differences in BDI, BAI and PI. We found, however, that the final value in the Beck Hopelessness Scale (BHS) was significantly higher in the repeaters group (figure 1). It is evident that the repeaters group and persons who had committed multiple previous parasuicide have higher levels of hopelessness than that of the non-repeaters group or those with only a previous parasuicide act. Even though the size of the sample is small, those subjects with strong purpose show significantly higher levels of hopelessness. This group exhibits negative perceptions and expectations about themselves, about the environment and about the future. This data are in agreement with the studies that suggests that a negative cognitive, emotional and existential state is the parameter that can better predict the risk of repetition of parasuicide10-12.
On the other hand, an important aspect of the results, is the value of IP scale. Several studies have evidence to suggest that this feature is related to the parasuicidal risk18-27 and this work also demonstrated that the average final values of the Plutchick Impulsivity Scale was higher than 21. This fact confirms that a correlation between the impulsivity level and parasuicide exists.
In addition, the analysis shows a variation of the tendency with time. In fact, we have observed that final value in the repeaters group tended to be less than that of the non-repeaters group (althogh not significant; difference = 3.975; p-value = 0,11). Among the group with multiple previous acts the decrease in the average final value of the IP scale is almost significant if we compare the subjects repeaters to the non-repeaters (difference = 5.547; p value = 0.085) while in the group with only a previous parasuicide act that tendency was less marked (difference = 3.048; p value = 0.426). This data, is partly in agreement with other studies40, 50 and a possible explanation is that the impulsive attempts would be associated with "mo-tor" impulsivity24 and this, after the same attempt, would decrease (as if the subject was not aware that he is at threat of dying, while, after having survived, he learns how to control his impulsivity). We can explain this tendency by considering that the subjects that commited parasuicide impulsively, with time, learned how to control themselves and they didn't attempt it again, while only those with strong intent in this group (with relatively lower impulsivity levels and with higher hopelessness levels) had retried.
Often, the environmental factors, such as the negative and chronic vital events, can act as factors that contribute in a significant way to suicidal behaviors17. The interview, indeed, proved that 55% of the cases referred to have had some negative relationship vital events in the last 5 years and up to 77% related some relationship problems with their spouse, parents or personal relationship breakup as reason of the parasuicide. Other types of vital events that present a connection with parasuicide are considerable less in proportion sensibly inferior (11.1% VE of health and 11.1% labor). This would leave us to think that the people would benefit from confrontation strategies to resolve pro-blems in their interpersonal relationship.
Limitations. There are several limitations that should be considererd in evaluating the present study. Firstly, the small size of the sample: although statistical significance is evident, it limits the capacity to identify possible variables of confusion. Secondly, the recruitment and follow-up of the subjects in the community environment and years after the parasuicide attempt, represent a methodological difficulty and a possible cause of recall bias. Also, the compilation of the table of vital elements at home although, on one hand anonymity is guaranteed, it can also result in the concealment of data and loss of information.
In conclusion, the major findings of this study is that, in the persons who have a past history of previous parasuicides, a high final value in BHS is strongly associated with the risk of parasuicide repetition in the subsequent two years, and they have lower levels of impulsivity, althogh not significant. Further studies, will be required to replicate these results.
References
1. Diekstra RF. The epidemiology of suicide and parasuicide. Acta Psychiatr Scand 1993; suppl. 371: 374-385. [ Links ]
2. Rodríguez Pulido F, Sierra A, Gracia R, Doreste J, Gonzalez Rivera JL. Methodological Problems in the Recording of Completed Suicides: a Study of the Situation in the Canary Islands. Eur J Psychiat 1991; 5 (3): 133-140. [ Links ]
3. Rodríguez Pulido F, Sierra A, Doreste J, Gracia R, González-Rivera JL. Suicide in the Canary Islands: standardized epidemiological study by age, sex, and marital status. Soc Psychiatry Psychiatr Epidemiol 1992; 27: 69-74. [ Links ]
4. Rodríguez Pulido F, Sierra A, Gracia R, Doreste J, Delgado S, González-Rivera JL. Suicide in the Canary Islands, 1977-1983. Acta Psychiatr Scand 1991; 84: 520-523. [ Links ]
5. Rodríguez Pulido F, Méndez Abad ME, González de Chaves F, Montesdeoca Hernández D, González Dávila E. The Epidemiology of parasuicide in Canary Islands. Eur J Psychiat 2006; 4 (20): 203-209. [ Links ]
6. Schmidtke A, Bille-Brahe U, de Leo D, Kerkhof A, Bjerke T, Crepet P, et al. Attempted suicide in Europe: rates, trends and sociodemografic charateristics of suicide attempters during the period 1989-1992. Results of the WHO/EURO Multicentre Study on Parasuicide. Acta Psychiatr Scand 1996; 93(5): 327-338. [ Links ]
7. Chia BH, Chia A, Tai BC. Suicide letters in Singapore. Arch Suicide Res 2008; 12(1): 74-81. [ Links ]
8. Terwilliger JD, Goring HH. Gene mapping in the 20th and 21st centurias: statistical methods, data análisis, and experimental design. Hum Biol 2000; 72: 63-132. [ Links ]
9. Mann JJ, Waternaux C, Haas GL, Malone KM. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry 1999; 156: 181-189. [ Links ]
10. Cester D, Walker RL. Hopelessness, helplessness and haplessness as predictors of suicidal ideation. Omega (Westport) 2007; 55(4): 321-324. [ Links ]
11. Cukrowicz KC, Ekblad AG, Cheavens JS, Rosenthal MZ, Lynch TR. Coping and thought suppression as predictors of suicidal ideation in depressed older adults with personality disorders. Aging Ment Health 2008; 12(1): 149-157. [ Links ]
12. Jamieson PE, Romer D. Unrealistic fatalism in U.S. youth ages 14 to 22. Prevalence and characteristics. J Adolesc Health 2008; 42(2): 154-160. [ Links ]
13. Menninger KA. Man Against Himself. New York: Harcourt Brace World; 1938. [ Links ]
14. Lester D. Murders and suicide: are they really polar opposite? Beba Sci Law 1987; 5: 49-60. [ Links ]
15. Rhine MW, Mayerson P. A serious suicidal syndrome masked by homicidal threats. Suicide Life Threat Behav 1973; 3: 3-10. [ Links ]
16. Mann JJ, Brent DA, Arango V. The neurobiology and genetics of suicide and attempted suicide: a focus on the serotoninergic system. Neuropsychopharmacology 2001; 24: 467-477. [ Links ]
17. Wasserman D. Negative life events (losses, changes, traumas and narcissistic injury) and suicide. In: D. Wasserman, editor. Suicide: an unnecessary death. London: Dunitz; 2001. p. 111-117. [ Links ]
18. Bryant E, Garrison C, Valois R, Rivard J, Hinkle K. Suicidal behavior among youth with severe emotional disturbance. J Child Fam Stud 1995; 4: 429-434. [ Links ]
19. Crosby A, Cheltenham M, Sacks J. Incidence of suicidal ideation and behaviour in the United States, 1994. Suicide Life Threat Behav 1999; 29: 131-140. [ Links ]
20. Kessler R, Borges G, Walters E. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry 1999; 56: 617-626. [ Links ]
21. Kuo W, Gallo J, Tien A. Incidence of suicide ideation and attempts in adults: the 13 year follow-up of a community sample in Baltimore, Maryland. Psychol Med 2001; 31: 1181-1191. [ Links ]
22. Simon T, Swann A, Powell K, Potter L. Characteristics of impulsive suicide attempts and attempters. Suicide Life Threat Behav 2001; 32: 49-59. [ Links ]
23. Wyder M. Understanding deliberate self harm: An enquiry into attempted suicide. Doctoral Dissertation. University of Western Sydney. Sydney. 2004. [ Links ]
24. Baca García E, Díaz Sastre C, Resa E, Blasco H, Conesa D, Oquendo M, et al. Suicide attempts and impulsivity. Eur Arch Psychiatry Clin Neurosci 2005; 152-156. [ Links ]
25. Bertolote J, Fleischman A, De Leo D, Botega N, De Silva D, Tranh H, et al. Suicide attempts, plans, and ideation in culturally diverse sites: the WHO SUPRE-MISS community survey. Psychol Med 2005; 35: 1457-1465. [ Links ]
26. De Leo D, Cerin E, Spathonis K and Burgis S. Lifetime risk of suicide ideation and attempts in an Australian community: prevalence, the suicidal process, and help-seeking behaviour. J Affect Disord 2005; 86: 215-224. [ Links ]
27. Pérez V. The relationship between seriously considering, planning, and attempting suicide in the Youth Risk Behavior Survey. Suicide Life Threat Behav 2005; 35: 35-44. [ Links ]
28. Zouk H, Tousignant M, Seguin M, Lesage A, Turecki G. Characterizaacion of impulsivity in suicide completers: Clinical, behavioral and psychosocial dimensions. J Affect Disord 2006; 92: 195-204. [ Links ]
29. Conner K, Hesselbrock V, Schuckit M, Hirsch J, Knox K, Meldrum D, et al. Precontemplated and impulsive suicide attempts among individuals with alcohol dependence. J Stud Alcohol 2006; 67: 95-97. [ Links ]
30. Brodsky BS, Oquendo M, Ellis SP, Haas GL, Malone KM, Mann JJ. The relationship of childhood abuse to impulsivity and suicidal behavior in adults with major depression. Am J Psychiatry 2001; 158: 1871-1877. [ Links ]
31. Soloff PH, Lynch KG, Nelly TM. Childhood abuse as a risk factor for suicidal behavior in borderline personality disorder. J Personal Disord 2002; 16: 201-214. [ Links ]
32. Van Egmond M, Diekstra RFW. The predictability of suicidal behaviour. Results of a meta-analysis of published studies. Crisis 1990; 11(2): 57-84. [ Links ]
33. De Moore GM, Robertson AR. Suicide in the 18 Years After Deliberate Self-harm. A prospective Study. Br J Psychiatry 1996; 169: 489-494. [ Links ]
34. Rygnestad T. Mortality after deliberate self-poisoning. Soc Psychiatry Epidemiol 1997; 32: 443-450. [ Links ]
35. Van Gastel A, Schotte C, Maes M. The prediction of suicidal intent in depressed patients. Acta Psychiatr Scand 1997; 96: 254-259. [ Links ]
36. Beck AT, Epstein N, Brown G. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol 1988; 56: 893-897. [ Links ]
37. Beck AT, Guthy D, Steer RA, Ball R. Internal consistencies of the original and revised Beck Depression Inventory. J Clin Psychol 1984; 40: 1365-1367. [ Links ]
38. Beck AT, Steer RA. Manual for the Beck Hopelessness Scale. San Antonio, Psychological Corporation. 1988. [ Links ]
39. Plutchik R, Van Praag H. Is there a relationship between seriousness of intent and the lethality of the suicide intent? Psychiatry Research 1989; 27: 71-79. [ Links ]
40. Kingsbury S, Hawton K, Steinhardt K, James A. Do adolescents who overdose have specific psychological characteristics? A comparison study with psychiatric and community controls. J Am Acad Child Adolesc Psychiatry 1999; 38: 1125-1131. [ Links ]
41. Hawton K, Rodham K, Evans E, Weatherall R. Deliberate self harm in adolescents: self report survey in schools in England. Br Med J 2002; 325: 1207-1211. [ Links ]
42. Ystgaard M, Reinholdt N, Husby J, Mehlum J. Deliberate self harm in adolescents. Tidsskrift for Den Norske Laegeforening. Norwegian Medical Journal 2003; 123: 2241-2245. [ Links ]
43. De Leo D, Heller T. Suicide in Queensland 1999-2001: Mortality Rates and Related Data. Australian Institute for Suicide Research. Brisbane; 2004. [ Links ]
44. Beck AT, Kovacs M, Weissman A. Assessment of suicidal intention: the Scale for Suicide Ideation. J Consult Clin Psychol 1979; 47: 343-352. [ Links ]
45. Pacurucu Castillo S, Gorenc KD, Nadelsticher A, Feuerlein W. Alcoholism diagnosis with Malt (Müncher-Alkoholismus-Test) Empiric evaluation study. Rev Neuropsiquiatr 1994; 57: 71-87. [ Links ]
46. Welch SS. A review of the Literature on the Epidemiology of Parasuicide in the General Population. Psychiatr Serv 2001; 52: 368-375. [ Links ]
47. Hathaway SR, McKinley JC. MMPI-2. Inventario Multifásico de Personalidad de Minnesota-2. (Aplicación informática) (Adaptación española). Madrid: TEA Ediciones S.A.; 1998. [ Links ]
48. Johnsson Fridell E, Öjehagen A, Träskman-Bendz L. A 5-year follow-up study of suicide attempts. Acta Psychiatr Scand 1996; 93: 151-157. [ Links ]
49. Corbitt EM, Malone KM, Haas GL, Mann JJ. Suicidal behavior in patients with major depression and comorbid personality disorders. J Affect Disord 1996; 39:61-72. [ Links ]
50. Corruble E, Damy C, Guelfy J. Impulsivity: a relevant dimension in depression regarding suicide attempts. J Affect Disord 1999; 53: 211-215. [ Links ]
![]() Correspondence:
Correspondence:
Dr. Francisco Rodríguez Pulido
Facultad de Medicina. Universidad de La Laguna
Área de Psiquiatría. Campus Ciencias de la Salud
38071 La Cuesta. La Laguna. Tenerife
Tfno: +34 922 319 278
Fax: +34 922 319 279
E-mail: fpulido@ull.es
Received: 15 October 2008
Revised: 9 July 2009
Accepted: 10 July 2009

