










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkThe European Journal of Psychiatry
versión impresa ISSN 0213-6163
Eur. J. Psychiat. vol.30 no.3 Zaragoza jul./sep. 2016
ADHD symptoms in children aged 5 to 15 years in Zhabei District, Shanghai
Wen-Lan Jina,b; Gai-zhi Lia; Ya-Song Dua; David Coghillc; Shun Aud and Xiang-Yang Zhonge
a Shanghai Mental Health Center, Shanghai Jiaotong University School of Medicine, Shanghai China
b Shanghai First People's Hospital, Shanghai Jiaotong University, Shanghai China
c Departments of Psychiatry, Ninewells Hospital and Medical School, University of Dundee, Dundee United Kingdom
d Chinese Mental Health Associations, London United Kingdom
e Zhabei District, Shanghai Teachers Training College, Shanghai China
This study was supported by the United Kingdom Dundee University Research Fund "Increasing awareness of ADHD in China" (2008.09-2013.08) and the Shanghai Shen Kang Hospital Development Center's grant for "Attention deficit hyperactivity disorder intervention technology promotion and application" (SHDC12010225).
ABSTRACT
Background and Objectives: The prevalence of attention deficit hyperactivity disorder (ADHD) and its related factors remains unclear in Shanghai.The aim of this study was to investigate the positive rates of ADHD symptoms and the associated factors in a sample of children aged 5 to 15 years in Zhabei District, Shanghai.
Methods: The participants were selected by cluster-stratified sampling of the general information and responses gathered from questionnaires on ADHD symptoms. The questionnaires examined summed up to 9,627. The positive rates of inattention and hyperactivity-impulsivity symptoms and the socio-demographic factors were compared.
Results: The positive rates of most ADHD symptoms decreased with age. Children between 5 and 7 years and between 7 and 9 years exhibited the highest ADHD positive rates. Boys showed a higher positive rate of ADHD symptoms compared to girls. Children who were local residents showed a higher rate than nonlocal residents and those of other nationalities. This might be related to the integration of immigrants and those belonging to lower socioeconomic classes. The positive rates of ADHD symptoms decreased with the educational level of the parents, while the parents'; level of education was associated with the severity of the ADHD symptoms. Problems of inattention were more common than problems of hyperactivity, as indicated by the positive rates.
Conclusions: The improper educational guidance of ineffective parents, as well as simple and crude attitudes to education, may place children in such a conflicting state, gradually creating psychological problems and resulting in a lack of self-confidence and ADHD.
Keywords: ADHD; Symptoms; Children.
Introduction
Attention deficit hyperactivity disorder (ADHD) is among the most common and intensely investigated but diagnostically controversial neurobehavioral conditions of childhood 1. ADHD is the most common behavioral problem that is clinically observed by child psychiatrists in outpatient children. The core symptoms of ADHD include inattention, hyperactivity, and impulsivity, with the age of onset being before 7 years 2. The prevalence rate of ADHD is controversial. High variability is observed despite the 3-5% range indicated by the Diagnostic and Statistical Manual of Mental Disorders (DSM IV), and this range is probably the most widely accepted range by the scientific community. According to various studies, prevalence rates of 2% to 30% have been obtained in the general population 3,4. No reliable laboratory examinations exist to help diagnose ADHD; thus, the diagnosis of ADHD requires reporting and evaluations by parents and teachers, assessments, and the research method of consolidating information 5. ADHD diagnoses are increasingly complicated because of comorbid disorders, such as learning disabilities, conduct disorder, oppositional disorder, and anxiety. The prevalence of ADHD in different countries and regions vary significantly, which is probably a result of different studies employing different methods and diagnostic criteria for diagnosing the disorder 6. ADHD causes not only many problems in the afflicted children, such as poor classroom behavior, academic underachievement, interpersonal communication barriers, and serious effects on academic performance and everyday life, but the condition also presents learning-related difficulties to the parents and teachers. ADHD may persist into adulthood; affect performances in academic, social, occupational, and familial spheres; and increase the use and abuse of alcohol and psychoactive substances and the risk of accidents7. ADHD has drawn considerable interest from child psychologists, teachers/educators, psychiatry experts, and parents and has become a global problem8. The objective identification of the characteristics of ADHD symptoms in childhood is important to prevent and manage the disorder9.
ADHD can influence family relationships, including marriages and parent-child relationships, parental awareness (decreased parental function and increased parental pressure), and the psychopathological state of parents, involving varying degrees of relationships. Although the mutual influence of child and family characteristics remains poorly understood, the effects of gender, culture, ADHD subtype, and family factors on the syndrome have been reported10. Family is the primary environment of children, and it shapes their psychological and behavioral characteristics. Parents influence the actions of their children and know the behavior of their children better than others11.
Methods that are more efficient must be employed to monitor the prevalence of ADHD and understand its implications on public health. A thorough understanding of the epidemiologic features of ADHD symptoms in children is important for prevention and management. Population-based epidemiologic studies can develop an understanding of ADHD, including its natural history, treatment, and consequences12. With a screening survey questionnaire of parents in Zhabei District in Shanghai, we investigated the symptoms and factors influencing ADHD symptoms among children between 5 and 15 years of age in order to provide clues to the basic theory of ADHD and other behavioral problems in children.
Materials and methods
Subjects
From April to May 2009, we conducted a multistage (stratified, clustered, and random) sampling in kindergartens, primary schools, and high schools of 5- to 15-year-old children in the Zhabei District, Shanghai, China, which has a population of 1 million. We sampled 15,112 students from 12 kindergartens, 12 primary schools, and 8 junior middle schools and sent their parents questionnaires. Collectively 12,954 questionnaires were retrieved, of which 778 were invalid, 2,189 were unanswered, and 9,627 (63.7%) were valid. This study was conducted in accordance with the Declaration of Helsinki and with approval from the Ethics Committee of Zhabei District in Shanghai. Written informed consent was obtained from all of the participants.
Research methods
The general questionnaire inquired about age, gender, nationality, educational level, family background, rearing pattern of parents, child development history, learning conditions, and other general demographic information. Each questionnaire was accompanied by an informed consent agreement.
The questionnaire on ADHD symptoms and diagnostic criteria was adapted from the DSM-IV. The questionnaire included nine questions each on attention and hyperactivity problems13.
The following procedure was performed: 1) questionnaires were printed in a standardized format; 2) they were distributed to the school principals or psychology teachers; 3) project investigators were responsible for giving the instructions to the parents on how to complete the questionnaire; and 4) with the assistance of the psychology teachers, the completed questionnaires were retrieved.
Questionnaire quality evaluation
First, we randomly selected a set of 10 to 11 children from each grade of one kindergarten, primary school, and junior middle school. We investigated and analyzed 114 children for the pilot study. Completed questionnaires that were returned summed up to 103. The questionnaire revealed the reasons for the high rate of invalid questionnaires: no informed consent from parents, incomplete basic personal information, numerous unfilled entries, lengthy questionnaire entries, low response rate to open-ended questions. In addition, some parents perceived questionnaires as troublesome or time-consuming, and were unwilling to complete the questionnaire. To improve the questionnaire, we modified the informed consent form and provided complete instructions, asked more general-information questions about the children, omitted open-ended questions, and provided key explanations on irregular entries or errors while training parents to avoid incomplete and incorrect entries.
Statistical analysis
The self-administered questionnaires were recorded with the Windows XP platform. All raw data were entered into and quantified with Excel's built-in applications. A trained data entry clerk performed the original data entry and storage and, after checking, copied the data to a disc. The statistical analysis, including the descriptive analysis, Student's t-test, and chi-square test, were conducted with SPSS 13.0 (IBM Corporation, Armonk, NY, USA).
Results
Respondent information
The relationships of the respondents to the children were the following: father (35.9%), mother (58.1%), and others (3.3%). No response recorded (2.8%). The gender of the respondents was male (37.9%) or female (59.7%). No response recorded (2.4%). The gender of the children and adolescents were male (48.8%) or female (48.6%). No response was recorded in 2.6% of the cases. The age of the respondents was 25 years to 80 years, with a mean age ± SD of 38.7 ± 6.9. The location of the children's residences was urban (69.5%), rural (27.7%), or foreign (0.3%). No response was recorded in 2.5% of the cases.
Positive rates of ADHD symptoms
The highest positive rate obtained among the nine attention deficit symptoms was 56.7% ("in homework, work, or other activities, often cannot pay close attention to detail or has errors caused by carelessness"); the lowest positive rate was 14.5% ("often does not follow instructions to complete work, home chores, or other tasks [not due to defying behavior or not understanding the instructions]"). The positive rates for the other items were between 19.4% and 42.7%.
The highest positive rate obtained among the nine hyperactivity symptoms was 25.1% ("eager to answer the question before the person finishes asking"), whereas the lowest was 7.2% ("often leaving the seat in classrooms or other occasions where they should be seated"). The other symptoms exhibited positive rates between 8.6% and 24.2%.
Age distributions of attention deficit and hyperactivity symptoms
The questionnaire on ADHD symptoms was based on the DSM-IV diagnostic criteria (1 to 9 for attention deficit symptoms and 10 to 18 for hyperactivity symptoms; Appendix 1). Table 1 lists the 18 positive rates for all of the age groups. Children aged between 5-7 years exhibited the highest positive rate of hyperactivity symptoms, whereas those between 5-7 years and between 7-9 years obtained the highest positive rates of attention deficit symptoms. Children from 13 to 15 years obtained the highest positive rate for the 9th entry. Between 13-15 years, the positive rate of attention deficit and hyperactivity symptoms declined gradually.

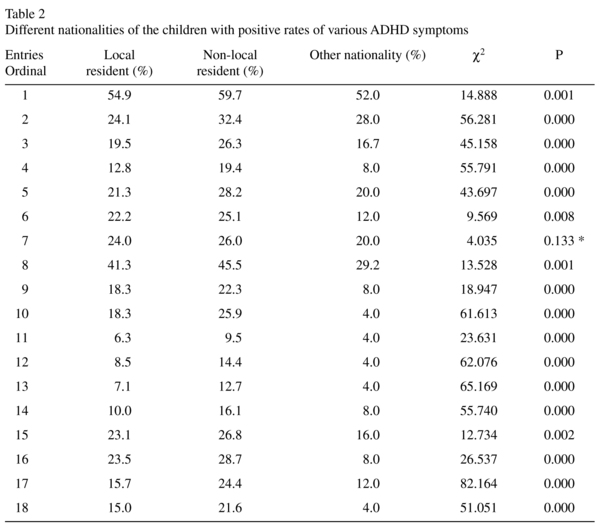
Differences in the positive rates of ADHD symptoms in different nationalities
The nationalities of the participating children were classified into local residents (69.5%), non-local residents (27.7%), other nationalities (0.3%), or no response (2.5%). Among the 18 entries, the positive rates of ADHD symptoms in children who were non-local residents were higher than those in children who were local residents and of other nationalities (Table 2). No statistical difference was found in responses to question 7 (P > 0.05); however, significant differences were observed in response to the other 17 questions (P < 0.01).
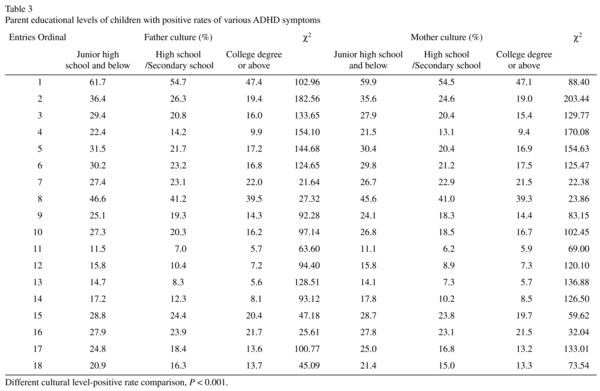
Differences in sex and educational levels of the parents of children with ADHD positive rates
The positive rate in males was higher than that in females, with a large significant difference (P < 0.001). Regarding the educational level of the parents, a significant difference in the symptoms was indicated (P < 0.001). As the educational level increased, the positive rate of the 18 symptoms decreased (Table 3).
Discussion
In our study, we found that attention problems obtained a generally higher positive rate than hyperactivity problems, suggesting that parents are more concerned about insufficient attention. Of all of the ADHD symptoms, attention problems affect academic performance and cause discontent among teachers. Compared to teachers, parents consider the symptoms of their children more seriously9.
In our study, the highest positive rate was recorded for children between 5 to 7 years as well as those between 7 to 9 years. Importantly, in this survey, items 10 to 18 in Table 1 showed that 5-7 year-old preschool-aged children had more hyperactivity/impulsivity symptoms, which was consistent with previous findings14. These results indicated that professionals should pay more attention in identifying the symptoms in preschool-aged children. Children of this age group lack self-control and exhibit hypofunction in the reflection of environmental inhibitive information. These children have difficulty accepting constraint and control. Active performance is observed as weak, whereas passive attention dominates, leading to a lack of concentration in class, which is manifested by frolicking with other students, looking around, ignoring rules and regulations, leaving their seats, answering questions without raising hands, and becoming easily excited. The impulsive behavior of these children interferes with the activities of other children, causing peer conflict. At this age, children also have defective perception and memory capacity, easily causing learning difficulties and a decline in academic performance. Students are often overloaded with schoolwork, engaged in various extracurricular training during their spare time, and experience psychological pressure; hence, they are prone to attention problems7.
Our study revealed that boys obtained significantly higher positive rates compared to girls, which was consistent with the higher prevalence of ADHD in males than in females. This gender difference is primarily due to the following reasons. 1) Because of the influence of social and cultural factors, boys are encouraged to participate in physical activities, similar entertainment, and games. They are mostly associated with outdoor activities, disciplinary action, and other violations of social norms. However, girls mainly participate in indoor activities and tend to be quiet, and, thus, are easily ignored by parents and teachers15. 2) Studies worldwide have attributed the higher incidence of ADHD in boys compared to girls to social and cultural factors. Another reason may pertain to society's standards for girls, including their evaluation and expectations. Family expectations are higher for boys, and excessive fondness for them can lead to violence and other psychological and behavioral problems. More attention deficit problems and fewer hyperactivity problems are observed among girls. Therefore, ADHD is diagnosed only when the child reaches middle school or when learning tasks are greatly emphasized16. Girls are more likely to be inattentive without being hyperactive or impulsive compared to boys. For many years, girls with ADHD have been ignored and overshadowed by hyperkinetic and impulsive boys, but have recently attracted interest in the understanding of the similarities and differences in prevalence, symptoms, familial risks, comorbidities, and treatments of ADHD between the two sexes. ADHD symptoms are not sex-specific; however, the identification of girls with ADHD symptoms is hampered by the parent-teacher bias and confusion17.
The occupation and education level of parents determine their lifestyle, career choices, concern for their children, child-rearing style, and family relationships. Therefore, the quality of parenting has a significant effect on the child's psychological and behavioral development. Different family environments produce different effects on the development of children. Poor environments contribute to the development of hyperkinetic symptoms or the exacerbation of existing symptoms among children, and rearing factors affect disease development and prognosis18. Therefore, the effects of parental involvement on the psychological and behavioral aspects of children are self-evident. In the family, the mother cares for the primary-school-aged child; thus, the quality of maternal parenting dramatically affects the child19. The educational level of the parents is inversely related to the positive rate of ADHD symptoms. The improper educational guidance of ineffective parents, as well as simple and crude attitudes to education, may place children in a conflicting state and gradually create psychological problems that result in a lack of self-confidence and ADHD. The positive rates that are attributed to children who are non-local residents exceed those that are attributed to children who are local residents and those of other nationalities. The reasons for this may include the following: immigrant households in Shanghai integrating with mainstream society to varying degrees, which leads parents to set higher expectations from their children; the non-local residents may mostly belong to lower socioeconomic classes or dysfunctional families.
The level of understanding of ADHD among families markedly differs. Some parents have positive expectations of their children but also desire to conceal their weaknesses from others. These parents refuse help in characterizing their children's behavior and regard the assessment scale as unreliable. In contrast, other families exaggerate the problems of their child. Another reason for the difference may be the inappropriateness of having parents assessing their own children's behavior in school. This study selected a school-based sample without conducting interviews with the teachers, which may have led to inaccurate results. More scientific assessments should be conducted by parents, teachers, and clinicians together under the guidance of doctors so that parents assess the behavior of their children at home and teachers evaluate the children's behavior in school20.
Due to the cross-sectional nature of this study and the shared variance from relying solely on parent reports, it will be critical for future research to replicate our findings with longitudinal and multi-informant data, such as using teachers' reports and standardized assessments. The number of clinical interviews conducted was also insufficient to determine the prevalence of ADHD. Thus, ADHD screenings should be performed in multiple settings in order to identify children who require further investigation.
Gaizhi Li did the same works as Wen-Lan Jin.
References
1. Skounti M, Philalithis A, Galanakis E. Variations in prevalence of attention deficit hyperactivity disorder worldwide. Eur J Pediatr. 2007; 166(2): 117-23. [ Links ]
2. Levin H, Hanten G, Max J, Li X, Swank P, Ewing-Cobbs L, et al. Symptoms of attention-deficit/hyperactivity disorder following traumatic brain injury in children. J Dev Behav Pediatr. 2007; 28(2): 108-18. [ Links ]
3. Cardo E, Servera-Barceló M. The prevalence of attention deficit hyperactivity disorder. Rev Neurol. 2005; 40: S11-15. [ Links ]
4. Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007; 164(6): 942-8. [ Links ]
5. Spencer TJ, Biederman J, Wilens TE, Faraone SV. Overview and neurobiology of attention-deficit/hyperactivity disorder. J Clin Psychiatry. 2002; 63 Suppl 12: 3-9. [ Links ]
6. Robison LM, Sclar DA, Skaer TL, Galin RS. National trends in the prevalence of attention-deficit/hyperactivity disorder and the prescribing of methylphenidate among school-age children: 1990-1995. Clin Pediatr (Phila). 1999; 38(4): 209-17. [ Links ]
7. Cornejo JW, Osío O, Sánchez Y, Carrizosa J, Sánchez G, Grisales H, et al. (Prevalence of attention deficit hyperactivity disorder in Colombian children and teenagers). Rev Neurol. 2005; 40(12): 716-22. [ Links ]
8. Biederman J, Petty CR, Evans M, Small J, Faraone SV. How persistent is ADHD? A controlled 10-year follow-up study of boys with ADHD. Psychiatry Res. 2010; 177(3): 299-304. [ Links ]
9. Soma Y, Nakamura K, Oyama M, Tsuchiya Y, Yamamoto M. Prevalence of attention-deficit/hyperactivity disorder (ADHD) symptoms in preschool children: discrepancy between parent and teacher evaluations. Environ Health Prev Med. 2009; 14(2): 150-4. [ Links ]
10. Gottesman MM. Helping parents make sense of ADHD diagnosis and treatment. J Pediatr Health Care. 2003; 17(3): 149-53. [ Links ]
11. Fernández A, Quintero J, Hornero R, Zuluaga P, Navas M, Gómez C, et al. Complexity analysis of spontaneous brain activity in attention-deficit/hyperactivity disorder: diagnostic implications. Biol Psychiatry. 2009; 65(7): 571-7. [ Links ]
12. Rowland AS, Lesesne CA, Abramowitz AJ. The epidemiology of attention-deficit/hyperactivity disorder (ADHD): a public health view. Ment Retard Dev Disabil Res Rev. 2002; 8(3): 162-70. [ Links ]
13. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. American Psychiatric Association, Washington, DC, 1994; 46-53. [ Links ]
14. Lahey BB, Carlson CL, Frick PJ. Attention deficit disorder without hyperactivity, in DSM-IV Sourcebook. (Widiger TA, Frances AJ, Pincus HA, Ross R, First MB and Davis W, eds.) American Psychiatric Press, Washington, DC.1997; 3: 63-188. [ Links ]
15. Cohen P, Cohen J, Kasen S, Velez CN, Hartmark C, Johnson J, et al. An epidemiological study of disorders in late childhood and adolescence -I. Age- and gender-specific prevalence. J Child Psychol Psychiatry. 1993; 34(6): 851-67. [ Links ]
16. Breen MJ, Altepeter TS. Situational variability in boys and girls identified as ADHD. J Clin Psychol. 1990; 46(4): 486-90. [ Links ]
17. Staller J, Faraone SV. Attention-deficit hyperactivity disorder in girls: epidemiology and management. CNS Drugs. 2006; 20(2): 107-23. [ Links ]
18. Concannon PE, Tang YP. Management of attention deficit hyperactivity disorder: a parental perspective. J Paediatr Child Health. 2005; 41(12): 625-30. [ Links ]
19. Johnston C, Mash EJ. Families of children with attention-deficit/hyperactivity disorder: review and recommendations for future research. Clin Child Fam Psychol Rev. 2001; 4(3): 183-207. [ Links ]
20. de Nijs PF, Ferdinand RF, de Bruin EI, Dekker MC, van Duijn CM, Verhulst DC. Attention-deficit/hyperactivity disorder (ADHD): parents' judgment about school, teachers' judgment about home. Eur Child Adolesc Psychiatry. 2004; 13(5): 315-20. [ Links ]
![]() Correspondence:
Correspondence:
Ya-Song Du
Department of Child & Adolescent Psychiatry
Shanghai Mental Health Center
Shanghai Jiaotong University School of Medicine
600 Wan Ping Nan Road Xuhui District
Shanghai 200030 China
Tel: +86 21 64387250
Fax: +86 21 64387986
E-mail: yasongdu@163.com
Received: 2 September 2015
Revised: 8 June 2016
Accepted: 17 June 2016
