










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.96 no.8 Madrid ago. 2004
| PICTURES IN DIGESTIVE PATHOLOGY |
Adenomatous polyp in the gallbladder
M. Menduiña Guillén, P. Alaminos García and M. Valenzuela Barranco
Departament of Medicine. University of Granada. Spain
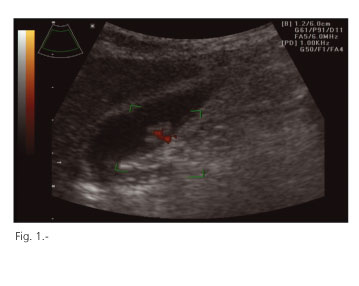
A 65-year-old woman with no medical history of interest was attended in our outpatient Gastrointestinal Clinic because of a persistent pain in the right upper quadrant of the abdomen for several days. Physical examination was normal. Hemogram, coagulation tests and blood biochemistry -including transaminases and alkaline phosphatase- did not show meaningful alterations. An abdominal ultrasound was performed in which a pediculous polypoid mass of approximately 2 cm in size, without posterior shading, was detected in the gallbladder. A color power Doppler identified an arterial vessel within the polyp (Fig. 1). A cholecystectomy was performed and histology revealed an adenomatous polyp.
The presence of a mass within the gallbladder is a relatively infrequent finding, and a malignancy should be excluded. Gallbladder adenomas are clinically and ultrasonographicaly similar to other polypoid masses. They represent only 4% of all gallbladder polyps. However, its malignant potential determines the clinical and diagnostic steps to be taken in patients with this incidental finding (1). The therapeutic strategy can be summarized as follows (1): a) all polyps larger than or equal to 1 cm in size represent an indication for cholecystectomy, as they may possibly be adenomas; b) gallbladder polyps smaller than 1 cm in asymptomatic patients require a (mid) yearly follow-up using ultrasounds; cholecystectomy should be performed if they grow to a size > 1 cm during follow-up; and c) in case of biliary symptoms and/or cholelithiasis an indication for cholecystectomy exists, regardless of size. At the present time, ultrasonography is without doubt the technique of choice in the study of the biliary system (1), as it has a high sensitivity and specificity in detecting the majority of intra- as well as extra-hepatic biliary diseases. However, the introduction of color Doppler systems has significantly improved the study of gallbladder conditions. Color Doppler ultrasonography can be used in the diagnosis of gallbladder masses simultaneously with conventional ultrasonography, and is extremely useful to differentiate between cancers and benign lesions (2). Some investigators try to differentiate between benign and malignant lesions by means of the vascularization pattern obtained by color Doppler ultrasonography. The absence of blood flow in a mass is known to be suggestive of a metastatic lesion. In addition, the presence of a signal of high blood flow within gallbladder masses or within the gallbladder wall is highly suggestive of primary cancer. A low blood flow suggests a benign lesion (2-5).
REFERENCES
1. Gil Grande LA, García-Hoz Rosales F, Bárcena Marugan R. En: Segura Cabral JM ed. Ecografía abdominal. Norma Madrid 1996; 4: 105-64.
2. Hirooka Y, Naitoh Y, Goto H, Furukawa T, Ito A, Hayakawa T. Differential diagnosis of gallbladder masses using colour Doppler ultrasonography. J Gastroenterol Hepatol 1996; 11: 840-6.
3. Levy AD, Murakata LA, Abbott RM, Rohrmann CA, Jr. From the archives of the AFIP. Bening tumors and tumorlike lesions of the gallbladder and extrahepatic bile ducts: radiologic-pathology. Radiographics 2002; 22: 387-413.
4. Li D, Dong BW, Wu YL, Yan K. Image-directed and color Doppler studies of gallbladder tumors. J Clin Ultrasound 1994; 22: 551-5.
5. Veno D, Tomiyma T, Tanos S, Wada S, Kimura K. Diagnosis of gallbladder carcinoma with color Doppler ultrasonography. Am J Gastroenterol 1996; 91: 1647-9.

