










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 no.6 Madrid jun. 2009
LETTERS TO THE EDITOR
Giant appendiceal mucocele. Implications for diagnosis and therapeutics
Mucocele apendicular gigante. Implicaciones diagnósticas y terapéuticas
Key words: Mucocele. Appendix. Treatment. Mucinous cystadenoma. Pseudomyxoma peritonei.
Palabras clave: Mucocele. Apéndice. Tratamiento. Cistoadenoma mucinoso. Pseudomixoma peritoneal.
Dear Editor,
Appendiceal mucocele (AM) is a cystic dilatation of the lumen of the vermiform appendix of obstructive aetiology that causes a retrograde accumulation of mucoid material. AM is found in 0.2-0.3% of all appendicectomies and accounts for around 8% of all appendiceal tumours (1). AM may be of non-neoplastic origin (retention cysts and mucous hyperplasia) or due to tumours (mucinous cystoadenoma or mucinous cystadenocarcinoma), these latter two accounting for two thirds of all AM. An incorrect therapeutic approach or poorly defined or incomplete histological diagnosis can result, in the medium or long term, in a pseudomyxoma peritonei syndrome (PMP), wich accounts for 1% of all colorectal cancers in the US.
Case report
The patient was a 47 year-old, with no prior digestive symptoms or abdominal pain reported. Routine follow-up laboratory analysis by her gynaecologist showed carcinoembryonic antigen levels (CEA) of 20.2 ng/ml. Accordingly, she underwent: a) an abdominopelvic ultrasound study that showed the presence of a 6.5 x 5.6 cm retrouterine mass appearing to belong to the right adnexa; b) a full colonoscopy thatwas completely normal; and c) a diagnostic laparoscopy that revealed the presence of a mass on the caecum and ascending colon that was highly vascularised an with a smooth, whitish surface. Both adnexae appeared normal and the uterus was hypoplastic.
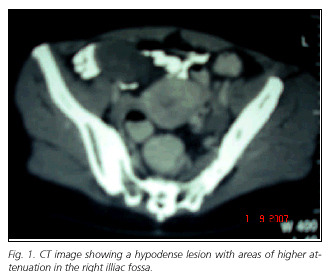
At this point she was referred to our service for surgery. Computerised tomography of the abdomen and pelvis showed a 11 x 8 cm encapsulated, pelvic mass, anterosuperior to the bladder and proximal to the terminal ileon, with no signs of infiltration of neighbouring organs, ascites or adenomegaly (Fig. 1). At elective surgery an AM with a maximum diameter of 12 cm was noted with no free fluid or implants in the pelvis or parietocolic folds. A right, oncological ileocolectomy was performed with a ileo-transverse anastomosis. The post-operative period was uneventful and the patient was discharged on the fifth post-operative day.
Gross examination of the colectomy specimen showed a markedly dilated caecal appendix measuring 9 x 5,5 cm occupied by mucoid material. The patology report was "appendiceal mucinous tumour of uncertain malignant potential with a secondary mucocele" being not possible to certificate the degree of local infiltration due to the calcium in the appendiceal wall. The eight lymph nodes isolated from the resected specimen were free of neoplasm (Fig. 2).

After a follow-up of three years, the patient remains asymptomatic and her most recent tumour markers and computerised tomography are completely normal.
Discussion
Appendiceal mucocele was first described as a pathological entity by Rokitansky in 1842 and definitively named by Feren in 1876 (2). It is a gross descriptive term referring to the dilatation of the lumen of the vermiform appendix caused by an abnormal accumulation of mucous. Higa (1973) considered AM according to one of the four causative histopathological processes (1,3): a) simple or retention mucoceles (15-20% of cases); b) mucoceles due to mucous hyperplasia (5-25%); c) mucoceles secondary to a mucinous cystoadenoma (50%), characterised by the presence of a dysplastic adenomatous epithelium with production of mucin; and d) mucoceles associated with mucinous cystoadenocarcinoma (11-20%), differing from mucinous cystoadenoma by the presence of high-grade cell dysplasia and oftenly by stromal invasion beyond the muscularis mucosae (1). Given the poor histological criteria defining invasiveness of mucinous tumours associated with AM, some researchers have used a third category of lesions (mucinous tumours of uncertain malignant potential), which reflects the occasional difficulty defining these lesions as either benign or malignant according to other variables apart from clinical behaviour.
AM is found in 0.2-0.3% of all appendicectomies and its prevalence is higher in women (a ratio of 4:1), with over 75% of cases are detected in the fifth and sixth decades of live (2). The clinical presentation of AM varies and is normally non-specific. Historically, 50% of patients are symptomatic and present the AM as an incidental finding during surgery, an imaging study or colonoscopy. In a review of 135 patients with AM, Stocchi et al. found that 51% were asymptomatic and, among those who did have symptoms, the most frequent were abdominal pain (27%), a palpable abdominal mass (16%), weight loss (13%) and nausea or vomiting (9%).
The endoscopic and radiological findings of AM have been clearly defined. The most specific finding in a plain abdominal radiography is a mass in the lower right quadrant with a curvilinear parietal calcification (50% of cases). Ultrasound examination shows a cystic mass with posterior enhancement, poorly defined wall and variable internal echogenicity depending on the composition of the mucous, with giant AM showing the typical, pathognomonic "onion-skin sign". Computerised tomography, the most specific study for its diagnosis, usually reports a well-encapsulated cyst with low attenuation in the appendix, with the above-mentioned calcifications in the wall. The presence of nodes with a greater density in the wall of the AM suggest malignancy (mucinous cystoadenocarcinoma), whilst increased volume in one or both ovaries, or the presence of mucinous ascites in the pelvis or right hemidiaphragm invariably indicates rupture of the mucocele. Concerning size, generically, AM < 2 cm are rarely malign whilst those > 6 cm are associated with mucinous cystoadenoma or mucinous cystoadenocarcinoma and have a rate of rupture above 20%.
Treatment of AM is always surgical due to the potential of low-grade mucinous neoplasms to progress to mucinous cystoadenocarcinoma and to the increasing risk of rupture and the development of the PMP syndrome. Sugarbaker et al. established as a starting point the integrity or otherwise of the AM (4). An intact AM, i.e., is a benign process and presents no risk to the patient, whereas a ruptured AM causes the content to exit into the peritoneal cavity; this content can be simple acellular mucous (simple or mucous hyperplasic AM) or contain epithelial cells with variable degrees of atypia, depending on whether the cause of the AM is a mucinous neoplasm with a low grade of malignancy or a mucinous cystoadenocarcinoma. In the review undertaken by Misdraji et al. involving 107 appendiceal mucinous neoplasms, the 39 patients with an intact AM had an event-free long-term evolution, whereas survival in those who had extra-appendiceal dissemination due to rupture was limited by the development of mucinous tumours on the perinoeal surface (5). As a general rule, the extension of surgery should be limited to resection of the appendix and the lymph nodes in the mesoappendix. In a recent review of 501 patients with malignant epithelial tumours of the appendix, González-Moreno et al. showed that right colectomy was associated with no benefit in survival compared with simple appendicectomy (6). More extensive surgery should be considered in two situations: positivity of the appendiceal resections margins, which should require caecectomy to the healthy margin, and gross involvement of the lymph nodes confirmed by intraoperative biopsy, which would necessitate right colectomy (4).
C. Jiménez Mazure, C. P. Ramírez Plaza, M. Valle Carbajo and J. Santoyo Santoyo
Department of General and Digestive Surgery. Hospital Regional Universitario Carlos Haya. Málaga, Spain
References
1. Higa E, Rosai J, Pizzimbono CA, Wise L. Mucosal hyperplasia, mucinous cystadenoma, and mucinous cystadenocarcinoma of the appendix. A re-evaluation of appendiceal "mucocele". Cancer 1973; 32(6): 1525-41. [ Links ]
2. Ruiz-Tovar J, García Teruel D, Morales Castiñeiras V, Sanjuanbenito Dehesa A, López Quindós P, Martínez Molina E. Mucocele of the appendix. World J Surg 2007; 31(3): 542-8. [ Links ]
3. Stocchi L, Wolf BG, Larson DR, Harrington JR. Surgical treatment of appendiceal mucocele. Arch Surg 2003; 138: 585-90. [ Links ]
4. Dhage-Ivatury S, Sugarbaker PH. Update on the surgical approach to mucocele of the appendix. J Am Coll Surg 2006; 202(4): 680-4. [ Links ]
5. Misdraji J, Yantiss RK, Graeme-Cook FM, Balis UJ, Young RH. Appendiceal mucinous neoplasms: a clinicopathologic analysis of 107 cases. Am J Surg Pathol 2003; 27: 1089-103. [ Links ]
6. González-Moreno S, Sugarbaker PH. Right colectomy does not confer a survival advantage in patients with mucinous carcinoma of the appendix and peritoneal seeding. Br J Surg 2004; 91(3): 304-11. [ Links ]

