










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 no.12 Madrid dic. 2009
PICTURES IN DIGESTIVE PATHOLOGY
Small bowel obstruction secondary to ileal endometriosis: multisection computer tomography evaluation
Endometriosis ileal como causa de obstrucción de intestino delgado: diagnóstico por tomografía computarizada multicorte
C. L. Fernández-Rey, S. A. Álvarez-González, P. Díaz-Solís, A. Blanco-González and S. Costilla-García
Services of Radiodiagnosis and General Surgery. Hospital Universitario Central de Asturias. Oviedo, Asturias. Spain
Approximately 10 to 15% of pre-menopausal women are affected by endometriosis, which in rare cases can cause intestinal obstruction (1). The presence of ectopic endometriotic tissue in the loops of the small bowel affects the serosa (visceral peritoneum) and muscularis propria, but never penetrates the mucosa (2). Fibrosis and secondary adhesions are the major causes of obstruction (2). Ileal involvement is uncommon and usually affects the terminal ileum within 10 cm of the ileocecal valve (3). Intestinal endometriosis should be suspected in cases of young nulliparous women with abdominal or pelvic pain (3,4).
Imaging diagnosis is difficult. However, multisection computer tomography (CT) provides high spatial resolution and multiplanar reformation images, which can be very demonstrative and characteristic.
Case report
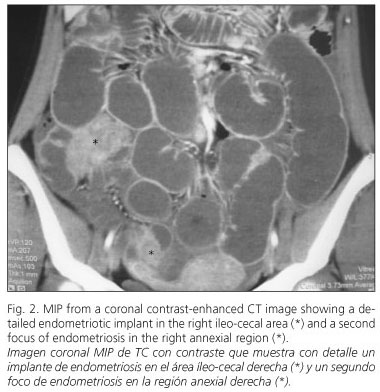
We report the case of a 22-year-old woman without any significant prior medical history who presented with abdominal pain and high leukocytosis. A contrast-enhanced multisection CT was performed, which revealed significant small-bowel dilatation and multiple nodular contrast-enhanced lesions located in the pelvis (Fig. 1). One of the lesions affected the right annexial region while the remaining lesions were located in the visceral peritoneum involving the small bowel. The largest lesion measured approximately 3 cm in diameter and involved the appendiceal region and terminal ileum, this being the transition point of the obstruction (Fig. 2). The diagnosis after CT examination was small-bowel obstruction secondary to intestinal endometriosis. Surgery confirmed the CT findings, identifying multiple endometriotic implants in the serosa of the small bowel, especially at the level of the terminal ileum (Figs. 3 and 4). A segment of terminal ileum and the appendix were resected. Histopathological examination of the resected specimen revealed endometriotic implants involving the appendix and terminal ileum.



References
1. Ruiz-Tovar J, Pina Hernández JD, Lobo Martínez E, et al. Endometriosis intestinal. Rev Esp Enferm Dig 2007; 99(12): 732-3. [ Links ]
2. Martimbeau PW, Pratt JH, Gaffey TA. Small-bowel obstruction secondary to endometriosis. Mayo Clin Proc 1975; 50(5): 239-43. [ Links ]
3. Scarmato VJ, Levine MS, Herlinger H, Wickstrom M, Furth E E, Tureck RW. Ileal endometriosis: radiographic findings in five cases. Radiology 2000; 214: 509-12. [ Links ]
4. Woodward P J, Sohaey R, Mezzetti TP. Endometriosis: radiologic-pathologic correlation. Radiographics 2001; 21: 193-216. [ Links ]

